Celebrating over 1 Million Downloads and 50,000 Free CEUs on the Sound Bites® Podcast | NEW: Get 1 years’ worth of CEUs with the new 15-CEU Podcast Course
The Science Behind Appetite and Other Factors that Influence our Food Intake
We hear a lot of bold claims about food and eating behavior: certain foods are “addictive,” ultraprocessed foods are driving obesity, and eating something sweet only makes you crave more sweets. We’re also told we can retrain our taste buds for things like salt and sugar, but is that really true? With the rise of GLP-1 medications and growing conversations around “food noise,” it’s becoming clear that appetite, cravings, and weight regulation are far more complex than many people realize. So what’s really driving our eating behaviors? How much is shaped by biology versus our environment or psychology? And what factors influence hunger, fullness, food preferences, and ultimately—how much we eat?
Tune in to this episode to learn about:
the concept of palatability and hyperpalatability
the truth about “addictive” foods
the role of appetite in GLP-1 medication effects
the importance and generality of hedonic shifts
various aspects of appetite regulation
sensory science, taste function, texture and food form
food noise vs. food cue reactivity
brand new research on protein and satiety
Rick Mattes MPH, PhD, RD
Dr. Mattes is a Distinguished Professor of Nutrition Science at Purdue University and Head of the Ingestive Behavior Research Center. His research focuses on the areas of taste function, hunger and satiety, food preferences, regulation of food intake in humans and human cephalic phase responses. He has authored over 300 publications. Dr. Mattes earned an undergraduate degree in biology and a Masters degree in Public Health from the University of Michigan as well as a doctorate degree in Human Nutrition from Cornell University. He conducted post-doctoral studies at the Memorial Sloan-Kettering Cancer Center and the Monell Chemical Senses Center.
Resources
Some links may be affiliate links. As an Amazon Associate, I earn from qualifying purchases.
In this particular case, if you think about how taking these foods out of the diet would impact segments of the population, you realize there’s really an ethical issue here. People who are food insecure have less resources available to them for cooking, for storing food, and so on.
If any food that contains a preservative is viewed as ultra-processed and should therefore, be avoided, that’s going to lead to increased foodborne illness. It’s going to lead to increased food waste, and where there are people who are hungry, food waste is not an acceptable option.
And about third of US households are single parents with children now, and convenience may have a negative connotation in some people’s minds, but it is an essential consideration for these kinds of families. Convenience is important to meet the stresses of daily life.
[Music Playing]
Voiceover (00:59):
Welcome to Sound Bites, hosted by registered dietitian nutritionist, Melissa Joy Dobbins. Let’s delve into the science, the psychology, and the strategies behind good food and nutrition.
Melissa Joy (01:21):
Hello, and welcome to the Sound Bites Podcast. Today’s topic is about different factors in food that have been said to influence or impact calorie intake, and therefore, weight, such as how processed a food is, the palatability or hyper palatability of a food, and hedonics or the enjoyment of food.
We often hear that certain foods are addictive and that ultra-processed foods are the cause of obesity. We hear that we can retrain our taste preferences for salt and sugar, but then we hear that having something sweet makes you want more sweet foods and beverages.
And with the popularity of GLP-1 medications, we’re hearing more about food noise and realizing that hunger and weight are more complex than many people realize. So, how much of eating behavior is driven by biology versus environment versus psychology, and what are the different variables involved in hunger, satiety, and ultimately, how much we eat?
My guest today is Dr. Rick Mattes. Dr. Mattes is a distinguished professor of nutrition science at Purdue University, and head of the Ingestive Behavior Research Center. His research focuses on the areas of taste function, hunger and satiety, food preferences, and regulation of food intake in humans.
He has authored over 300 publications. He earned an undergraduate degree in biology and a master’s degree in public health from the University of Michigan, as well as a doctorate degree in human nutrition from Cornell University. Welcome to the show, Dr. Mattes.
Dr. Rick Mattes (02:56):
Pleasure to be here.
Melissa Joy (02:57):
Can I call you Rick?
Dr. Rick Mattes (02:58):
Certainly.
Melissa Joy (02:59):
I’ve known you for a while. I don’t know that I can say we’ve known each other, but I met you years ago. I’ve seen you present many times and I’m just thrilled to get reconnected with you recently at a conference because I saw you speak at the IFT FIRST Conference last summer about hyper-palatability, and you’ve been on my list ever since then.
Before we get into today’s conversation, I would love for you to share with our listeners a little bit about your background and the work that you do, and any disclosures that you might have to note.
Dr. Rick Mattes (03:30):
So, I started out planning a career in public health and doing program evaluation when I was coming out of school, the WIC program was just beginning, and it fascinated me. But I got sidetracked after attending a psychology course on sensory function and nutrition, and have been on that trajectory ever since.
Following my doctorate, I went to the Monell Chemical Census Center in Philadelphia. It was at the time sort of the center of the universe for taste and smell research, and I spent 13 years there looking at the relationship between taste and smell and nutrition, and then moved to Purdue, and I’ve been here ever since, so almost 31 years. And as you said, I’ve been doing research in this area all that time.
Melissa Joy (04:18):
Wow, wow. Yeah, I guess I didn’t realize that your entire career has been devoted to this topic to sensory and taste, which is just fascinating. I’ve had some experts on the show over the past 11 years and it’s just fascinating. Really excited to dig into your research.
Let’s start maybe with a brief overview of your work in this field. If you had to tell somebody at a cocktail party what kind of work you’ve been doing or that you’ve seen in the literature in this field on taste or hunger or food preferences.
Dr. Rick Mattes (04:52):
So, I started off with the belief, the hope that we could use measurement of taste and smell as a way to help, diagnose, and manage a number of chronic diseases. And there are hypotheses out there that there should be some alteration of salt taste in people with hypertension and of sweet taste and people with diabetes, of fat taste with people with obesity, bitter taste for people with thyroid disorders, sour tastes for people with kidney disorders.
There are a lot of hypotheses out there, and I started working in that area, and ultimately, sort of migrated more to the study of food preferences rather than measures of sensitivity that is thresholds or scaling intensity ratings.
Those are both important and they’re interesting to study, but in my view, they’re really the substrate upon which hedonic judgments are made. We don’t eat food because we can barely taste a sweet note or because it’s a particular intensity – we rate it on whether we like it or not.
And so, I started to look at that more and link that to appetitive sensations and taking it one step further than to food choice, food intake, and energy balance.
Melissa Joy (06:11):
Very interesting. Before we focus on some of these current day buzzwords and theories regarding food intake, you alluded to a little bit of this, but are there some big changes that you’ve seen over the course of your career related to this area, maybe regarding weight or obesity, or specific nutrients? Obviously, fat was in the hot seat, then it was carbs and then sugar.
Dr. Rick Mattes (06:34):
Yeah, precisely. I’m old enough to have seen the cycle more than once. We like to vilify either tastes of foods, and they do seem to oscillate. When I first started my career, I was interested in salt taste and hypertension, and salt was viewed as the most problematic nutrient in foods that was supplanted by sugar, and then it was supplanted by fat, and then salt sort of reemerged.
And we’re still worried about sugar and fat, but we don’t seem to solve the problem. We make some advances, and then something else comes up and we’re distracted before we really find resolution. I think the biggest change has certainly been these GLP-1 medications. They have really changed the expectations of how to manage body weight, and so far, seem to hold a great deal of promise.
Melissa Joy (07:27):
I was a little surprised to find that some of your research is regarding GLP-1s, but when I think about it, it’s not surprising because of all of the overlap or connections there. So, we are going to talk about that and we’re going to talk about salt and sugar as well.
So, we’re talking about fat was the villain, sugar whack-a-mole, just changing over time, and now really we’re hearing about ultra-processed foods, and that seems to be the poster child right now. Why do you think ultra-processed foods are the main focus, and simple question with probably not a simple answer – but do you think it’s helpful for people to focus on that or to limit or to avoid them?
Dr. Rick Mattes (08:05):
Sure. This is a strong interest of mine right now. Normally, I disregard passing fad issues in nutrition. They come and they go, and the less said about them, the better because they have no substance. And I would have taken that same tact with ultra-processed foods, except it seems to be very sticky. It has really caught hold.
And there are many nations now around the world that are writing into their national dietary guidelines language that reflects this view that there are a class of foods that can be labeled ultra-processed that really should be avoided because they are contributing to a wide array of adverse health outcomes. My view is that this is not a helpful concept for a number of reasons.
In my mind, before one wants to set national policy about nutrition, there should be a confluence of evidence from different types of science. So, you want epidemiological evidence to establish that there is an association, a question that should be studied, and what groups may be at particular interest at greater risk for the problem.
And then you’d like to have randomized control trials to establish causality. And if indeed, there is a causal relationship, then the next step you’d like is mechanistic work. How would you intervene if indeed there really is a problem here? What changes would you make? And to be targeted with those so that you can increase efficacy and efficiency. So, where do we stand on this issue of ultra-processing and those three branches of science?
In my opinion, there is an abundance of epidemiologic evidence, no shortage of studies showing an association between consumption of these ultra-processed foods and many, many health outcomes. I’m going to focus on obesity since that’s kind of my area of work.
But I would argue that the epidemiology still has a number of important questions to answer. There is a large quantity of evidence, but the quality and the robustness of that evidence is to my mind, still lacking. So, if you look at the effect sizes in these epi studies, they’re very small.
With obesity, they’re often in the relative risk or hazard ratio area of 1.02, 1.03, maybe 1.05. There are many things that we know are contributing to obesity with effect sizes larger than that. Things like exercise and sleep duration and stress. So, the first point is that this ultra-process of food is not the gorilla in the room. Maybe it’s a contributor, but it’s not dominant.
Second, the evidence is not consistent. In the United States, for example, ultra-processed food intake is high. Yes, it is high, it’s somewhere in the mid-50% of energy from these kinds of foods, but it was at that same level for about a 20-year period when BMIs were going up markedly.
So, in epidemiology, you draw association when two trend lines are kind of moving in the same direction, and that’s not what has happened in the United States. And we have recently, there were a couple of papers published in the Lancet in November of 2025 garnered a good deal of attention that laid out the issue of ultra-processed foods.
So, we looked at that evidence for sales of UPF around the world, and we overlaid on that the obesity rates from the World Health Organisation over about a 20-year time span. And yes, I take it on face value that sales of these foods have gone up, but they did not predict obesity rates globally.
And then if you look at the meta-analyses that have been done (and there have been some very substantial ones), they generally argue that the quality of the evidence is very weak to weak, sort of at best, they show moderate level of data. So, I don’t think that we want to be making policy decisions on weak data.
And the final point to make on this issue is there are some segments of the population that really benefit from the consumption of ultra-processed foods, not the least of which are vegans and vegetarians. In the United States, they get about 40% of their energy from ultra-processed foods. And these are populations that we think are particularly healthy and have great longevity, so it’s not necessarily hurting them.
So, I would put all that together and say the epidemiology is abundant but not convincing. And then we can look at the randomized control trials, and there have been maybe four or five that were educational interventions trying to teach individuals how to avoid these foods, and then measuring health effects. In about half of those, they weren’t able to implement the intervention, people just wouldn’t follow the diet. And then the others, it had no impact on body weight.
And then if you move into the actual feeding trials, there is the very popularly cited Kevin Hall study, the first trial that was published in this area. He’s to be given credit for doing the first study and a difficult metabolic ward study at that. But the reality is it’s 20 people. It was a two-week intervention, no washout between the two arms of the intervention.
And as they note in their report, there was a negative trend in energy intake in the arm when people were on ultra-processed foods. So, overall, there was a 500-kilo calorie increment in the arm consuming ultra-processed foods compared to minimally processed, but it was decreasing at 25 kilo calories a day.
So, if the trial had been run just a bit longer than the two weeks, there would’ve been no difference at all. So, it’s a transient effect. And the next study that came out, out of Japan was only half the size, half the duration – actually, I think it was either eight or nine people in a one-week intervention. And that one also showed only a transient effect of energy intake. At the end of the week, there was no difference between them.
And then there were a couple other trials. One found no effect of putting people on a diet high and ultra-processed foods on body weight, and another found an actual decrease in body weight. Now, albeit less than the decrease in body weight when they put people on the minimally processed, but they still lost weight.
So, we have randomized control trials showing increased body weight, no change in body weight and decreased body weight. We are far from being able to look at the randomized control trials and conclude that there is a robust causal relationship between consumption of these foods and body weight. And then our belief is that there is no credible scientific evidence base on any mechanism driving this relationship.
And you mentioned hyper palatability at the start of this discussion, and now is a good place to address it. First off, there is no definition of hyper-palatability. It is intentionally a sensationalist descriptor to garner attention and raise concern, but there is no scientific definition of it. And in fact, it’s quite misinformed.
It assumes that palatability is a property of a food, and casual experience will show that’s just not the case. The palatability of a food differs between two people, and certainly between two cultures. It differs within the same person depending on metabolic state and life experience and so on. These are all things that indicate palatability is a characteristic of an individual, not a property of a food.
So, the whole notion that we can attribute excess energy intake to a property of a food that doesn’t exist, I think undermines the credibility of that mechanism. More recent evidence on other proposed mechanisms. For example, there’s talk about ultra-processed foods being easily ingested and digested. The most recent evidence shows that it’s not the processing that’s responsible for that, it’s food form.
Yes, we swallow liquids quicker than solids and semi-solids quicker than solids, and they require less time to pass through our stomachs and so on. But it’s not because of the processing, it’s just the physical form of the food. And if you sort of go down each of the proposed mechanisms that you see in the literature, there just isn’t a science base that substantiates it.
And I would normally say, well, if it’s benign and maybe avoiding these foods is helpful to some people, then it’s not worth raising an issue, but it’s not. In this particular case, if you think about how taking these foods out of the diet would impact segments of the population, you realize there’s really an ethical issue here.
People who are food insecure have less resources available to them for cooking, for storing food, and so on. If any food that contains a preservative is viewed as ultra-processed and should therefore, be avoided, that’s going to lead to increased foodborne illness, it’s going to lead to increased food waste.
And where there are people who are hungry, food waste is not an acceptable option. And about third of US households are single parents with children now. And convenience may have a negative connotation in some people’s minds, but it is an essential consideration for these kinds of families.
Convenience is important to meet the stresses of daily life. And these foods are, yes, they’re convenient, and they provide a lot of shortfall nutrients that maybe were taken out of foods during processing and so on, but now have been fortified and enriched. And those foods are important sources of those nutrients for these populations.
So, there are real concerns, tangible concerns with taking these foods out of the diet. And to remove 50% of the foods that contribute 50% of the energy in their diet without knowing how people will adjust to that is also a dangerous concept. It cannot be assumed that we will automatically shift to making very healthful food choices.
You can have a diet composed of very nutrient-rich foods, but not very diverse and still get into nutritional problems. We cannot assume that just taking these foods out will lead to necessarily a very healthful diet and to replace it without doing the research and without knowing how to guide people in making that transition.
Melissa Joy (19:54):
So, taking that out of the diet could lead to a variety of things like you said, that we don’t even know. So, we could be making a situation even worse.
Dr. Rick Mattes (20:05):
That’s correct.
Melissa Joy (20:06):
So many things that you said, I jotted some notes as you were talking. When I started getting involved in the ultra-processed foods conversation and seeing the Nova classification system, which I’ve talked about on the podcast before, and seeing like, okay, not all ultra-processed foods are created equal, and almost thinking like okay, some of these are clearly a term we don’t use anymore: junk foods.
And some of them are things like flavored yoghourt, and tofu, and whole wheat bread and things that clearly we know are nutritious, nutrient-rich (you’ve used that term, I love that term as well). So, I kept wanting to go back to, well, how much nutrition does this food provide versus how processed is it?
And then I heard the term hyper-palatability, and before I heard you speak about it at IFT first last summer, my understanding of hyper-palatability, which I had an episode on the podcast with Dr. Mark Messina, was kind of that speed of eating, and he was talking about soy foods, and he said, “You can’t drink a glass of soy milk faster than you can drink a glass of regular milk. You can’t eat a soy burger faster than a regular burger.”
But when I heard you speak at IFT and you were talking more about what I hear other people referring to is the food craving or that food is addictive, or it’s engineered for us to crave it and that sort of a thing. And you were talking more about I guess I would say the palatability and again, the hyper-palatability, and you explained what you did just now, that that’s not a characteristic of the food.
It’s going to vary from person to person, and I might find something very desirable (I guess that’s a better word) than somebody else. And so, it’s a moving target in that sense, and it’s all over the map.
Dr. Rick Mattes (21:50):
Yeah, very much so. When you do sensory studies, you ask people how much they like say lemonade with different levels of sugar in it. You’ll get some people that like very little sugar, some people that like a moderate amount, and some people that like a very strong amount.
If the food industry truly had figured out what was this magic formulation to make a food irresistible and to drive access intake, which segment of the population have they formulated it for? It’s not everybody. And that’s true for any food that you can think of.
The example I often use is coffee. You get these pods – and I don’t endorse any company, but I think different companies make pods, and there are dozens of these kinds of pods. So, obviously, there are people that differentiate between them. And each of those people may put a small amount of sugar, a medium amount of sugar, or a large amount of sugar in their coffee.
They may put no cream, little cream, or a lot of cream, and they may use skim milk, the whole milk. There are literally thousands of variations of a cup of coffee. How can we talk about there being a hyper-palatable version of that? It just doesn’t have any scientific standing.
Melissa Joy (23:08):
Yes, and again, I felt like, oh, maybe this hyper-palatability is the elephant in the room sort of a thing. And maybe it’s not just about the nutrients in the food, but I like how your research and what you started talking about that we’re going to talk a little bit more about, is things that impact, like you said, the food form, versus processing.
So, we were at a meeting a couple weeks ago, the International Food Information Council had this convening, and we were talking about convenience foods and diet quality, and everything under that umbrella. And a few of the panelists talked about some of the research that’s going on with different textures and things like that, which I think, okay, that maybe this hyper-palatability conversation will lead us down different paths, and we might find something there.
Are you seeing much in your research or in the literature, whether it’s yours or others, more about the food forum, like the texture of food and how quickly we can eat or drink something?
Dr. Rick Mattes (24:12):
This has been a pretty highly researched and interesting topic for a couple decades now, and I think what really sparked interest in it was concern about sugar sweetened beverages. And the question was why are they problematic?
And to my mind, the real issue is not the sugar so much as the vehicle. We do not monitor and regulate energy well when it is ingested in the form of a beverage.
Melissa Joy (24:44):
Meaning our bodies aren’t really registering like, oh, that was 500 calories I just drank versus when we’re eating 500 calories. Yeah, I’ve seen that in the research.
Dr. Rick Mattes (24:53):
And again, I try very hard to just look at what is obvious in our day-to-day lives, that makes that make sense or not make sense. And if you think about individuals that have to increase their energy intake, maybe a patient with cancer, maybe an elderly person with early satiety, we don’t give them bars and solid foods as supplements.
We give them beverages. We try to get extra energy into them with a beverage because it is not tightly regulated, because they can take in more energy before they satiate. It’s just common knowledge, but it’s taken science a good deal of time to recognize that, and to come to grips with it.
Melissa Joy (25:42):
I’m going to ask this question kind of knowing it’s not a really valid question, I guess. Can you give some examples or an example of a food that people might assume is hyper-palatable, but it’s actually not?
Dr. Rick Mattes (25:55):
In my opinion, no food is hyper-palatable. Hyper-palatable is determined by the person.
Melissa Joy (26:00):
The person. That’s what I thought you were going to say.
Dr. Rick Mattes (26:01):
For one person, a bug can be hyper-palatable, and for another person, it’s a milkshake.
Melissa Joy (26:06):
Yeah, that’s what I thought. So, one of the things you also mentioned about fortified foods and enriched foods, and I talk about this a lot as well. Okay, we know the difference between junk foods and nutrient-rich foods. Stop anybody on the street and they can pretty much identify which foods are kind of junk foods and which foods are going to provide some sort of nutrition just inherently.
But to your point about even if it’s processed, packaged, ultra-processed, it might be fortified or enriched with important nutrients that are filling nutrient gaps and especially for certain populations like you said that are food insecure.
Can you talk a little bit more about that? Because again, it’s kind of like what we talked about at this diet quality and convenience food convening. My listeners are a mix of dietitians and the general public, and other health professionals as well. What message do you think is getting lost in that conversation? Because I feel like it doesn’t get its day in court.
Dr. Rick Mattes (27:06):
I’m an old-time dietitian. I believe that any food can fit in a helpful diet. I understand you’re using the term to raise an issue “junk food,” but I don’t use that term myself.
Melissa Joy (27:22):
I know.
Dr. Rick Mattes (27:22):
And there are certainly foods that we should not eat often or in large quantity.
Melissa Joy (27:28):
I don’t use the junk food term anymore, but I feel like, gosh, maybe that would help clarify things for people. Maybe let’s call them indulgent foods, I like that.
Dr. Rick Mattes (27:36):
Fine. So, there are foods that are indulgent foods and they play a role in quality of life. And when used in the right frequency and the right quantity, don’t pose any adverse health consequence, and enrich life.
Epicurus from about 300 B.C. said, “The goal of life is to find happiness.” And unfortunately, people misconstrue his message and think that he’s the father of hedonism and that excess is the goal of life, and that’s not at all what he said. He believes in a very simple life, but one that seeks out pleasure, and food is an important source of pleasure in our lives. We socialize around it, we have personal experiences with it.
So, the foods that give us satisfaction are not ones to be denigrated, but we have to learn how to use them intelligently. And so, that’s where the messaging falls apart, I think where we try to classify foods to make a message simple, we end up creating a mindset of good food, bad food, and bad foods are to be avoided at any cost, and that’s just not the way I view a healthful relationship with food.
Melissa Joy (28:54):
Very good. Yes, I was going to ask about GLP-1s next, but I think this is a perfect shift into talking about hedonic shifts. You have a new paper on this, so explain what this is, and maybe we can get into some of the research that you’ve seen on salt and sugar, and you mentioned sugar sweetened beverages, but I want to get into non-nutritive sweeteners too, because people have a lot of questions about that.
Dr. Rick Mattes (29:18):
So, it makes sense for humans to have the capability to learn to like the available food supply. If we were hardwired to only be willing to eat sweet food, say, and we were living in northern climates where for months of the year, there are no plants, so there is no source of sweetness – we would be at a great disadvantage in terms of survival.
So, we have to learn to what is available to us, and we call that learning and hedonic shift. And there are many mechanisms that can drive that. But the one we’re particularly interested in is just mere exposure. So how frequently you’re exposed to a given level of sweetness or saltiness will determine your preferred level of sweetness or saltiness.
And the evidence is, I think, strongest for salt taste at present. So, if you in a controlled experiment expose people to high levels of saltiness in their food, then they will track up and come to prefer that in their diet. But by the same token, if you reduce their exposure to saltiness, they’ll learn to like lower levels of salt in their food.
And in that, is a very important observation, and that is that this phenomenon works in both directions, and it is ever recalibrating. And so, it’s not like you can train your palate to like, say low levels of salts, and then you’re home free for the rest of your life.
Every time you eat, you are recalibrating. And so, if you’re not ever vigilant and only allowing yourself to be exposed to lower levels of salt and you start experiencing higher levels, you will track up again. So, it is a mechanism that can be used, but it’s one that, as I say, requires purposeful conscious decision to maintain a level of exposure.
Melissa Joy (31:18):
Otherwise, you’re kind of starting over each time to reduce your preference for salt.
Dr. Rick Mattes (31:23):
In the UK, in the early 2000s, the government decided that they were going to ratchet down the level of salt in the food supply in a slow controlled manner so that people were kind of unaware of this, and they were taking advantage of this hedonic shift phenomenon that with a slow reduction, you were learning to like lower levels of salt and food, and they got the population sodium level down about 15% over a decade.
Unfortunately, a new government came in that was less enthusiastic about government controls of one sort or another, and those programs were eliminated, and indeed, the population sodium level started to rise again.
But there is now a national public health effort that documents that this phenomenon can be used successfully, and that was with salt. There are also data for fat that very clearly show it’s the level of exposure to fat that determines the fat preference, not the metabolic consequence of eating fat.
So, if you put two groups of people one on a low-fat diet, and they’re allowed to use fat mimetics, so they maintain the oral experience of fat-
Melissa Joy (32:42):
The mouth feel-
Dr. Rick Mattes (32:43):
Yep, and taste actually, and you put another group on the same low-fat diet and don’t allow them to have that sensory exposure, it’s the group that’s deprived of sensory exposure that actually shifts down and it comes to prefer lower levels of fat in their food. So, the evidence is good there too, though there haven’t been large scale national efforts to try to exploit that with fat.
Now, the most interesting and most recent data indicates that sweet is not like salt or fat. There does not appear to be an hedonic shift for sweetness. I can’t say that there is an abundance of evidence on this, but the two best studies that have been published both came to the same conclusion, that putting people on reduced sweetness diets did not lead to a reduction in the preferred level of sweetness.
Now, whether we are just off the mark and these two studies happen to not find reality, or this is something special about sweetness, we don’t know yet. There are mechanisms that can be hypothesized that would argue that sweet is indeed unique, but we don’t have science yet to explain this, but it’s got some important implications. One of the concerns – you mentioned you were interested in low-calorie sweeteners?
Melissa Joy (34:14):
Yes.
Dr. Rick Mattes (34:15):
Their function is to maintain a level of sweetness and food without delivering calories. I mean, that’s by definition why we use them. One argument then against the use of low-calorie sweeteners is that they do exactly that. They encourage, preserve the high level of preferred sweetness level in our foods.
Melissa Joy (34:36):
And we hear that a lot.
Dr. Rick Mattes (34:39):
So, one could argue, well, then if we take them out, we can take advantage of this hedonic shift. But if the evidence is correct that there is no hedonic shift for sweetness, that’s no longer an argument against the use of low-calorie sweeteners.
And if low calorie sweeteners have the benefit of reducing sugar intake for people concerned about dental health and diabetes and so on, and energy intake for people who are concerned about body weight, then the argument against their use is now not as strong as it may have been.
Melissa Joy (35:13):
When we were talking earlier, I mentioned I did an episode, it’s episode 214, so about a hundred episodes ago, the Science of Sweetness with Kees de Graaf and Colin Rehm. You know Kees and you know his work, he’s been researching sweetness for about 30 years or so, I think.
I know we’ve heard about as a clinical dietitian telling people, if you use less salt, you’ll adjust to it. Haven’t heard much about the fat intake, but we hear all the time that if we use low-calorie sweeteners, it’s just going to make us want sweet things. And so, that was a huge aha for me to learn about Kees’s work. And thank you for explaining that here as well.
Dr. Rick Mattes (35:51):
A casual observation, again, on the fat story, there was concern about drinking whole milk and fat levels of milk. And so, a lot of people switch to reduce fat milk and skim milk, and they actually come to prefer that over time.
Melissa Joy (36:07):
Anecdotally too, yeah.
Dr. Rick Mattes (36:09):
Yeah, a casual observation that supports the hedonic shift for fat.
Melissa Joy (36:13):
And maybe there’s two different things going on there. One’s the hedonic shift and one is just a taste preference because you do hear people say, “Oh, I really cut back on sugar in my diet, and now when I have something sweet, I don’t like it.” So, maybe there’s different things going on there.
Dr. Rick Mattes (36:29):
As I say, there isn’t an abundance of evidence on the hedonic shift for sweetness, it’s just the two best studies on it don’t show it. There will be other data coming out (I hope soon) that will either confirm or raise new questions about this, but it’s a topic that’s actively under study.
Melissa Joy (36:48):
Wonderful. We’re going to talk about GLP-1s, and there’s also a brand-new paper or a critical review that just came out about protein that I know that you authored part of it on the satiety part of this critical review. So, tell me about your work or your research that involves GLP-1s. What are you seeing that you think is important to share with us?
Dr. Rick Mattes (37:10):
Yeah, so as I said at the onset, these medications are quite remarkable in their ability to promote weight loss. And the question then becomes, what is the mechanism? If we understand the mechanism, then that can guide future drug development and ways to improve these medications and reduce side effects and so on.
So, one of the observations that’s been made, there are shifts in food preferences in people that are using these medications. Interestingly, one often here is that there’s a reduced appeal of sweetness and a fattiness, and increased appeal of minimally processed foods, as a matter of fact, fresh fruits and vegetables and grains and so on.
So, it got us to thinking, well, is that shift in food preference linked to an actual change in taste and smell function? There is very good theoretical basis to suspect that it would be. Taste cells synthesize and secrete GLP-1.
There are GLP-1 receptors on neurons adjacent to those taste cells. The olfactory bulb is one of the most dense areas of insulin receptors on these medications are designed to help manage diabetes through a modulation of insulin. So, there’s good reason to believe taste and smell would be altered. And the preliminary studies that came out were mixed.
Some said heightened sensitivity, some said diminished, but most of it was based on studies that measure identification. So, the degree to which given a sample, you can say, “Oh, this is sweet, or salty or sour, bitter, or whatever,” and that measures of threshold or intensity and the like.
So, a graduate student in my group, Giorgia Rutigliani has just completed a trial where she looked at taste and smell function in people that were just about to start GLP-1 medications and people that had been on them for six months, and indeed, showed that particularly for sweet, there was a decreased threshold for sweetness and trends for the other taste qualities; for salty and sour and bitter or for fatty, but only statistically significant for sweet.
Though it’s still a relatively small sample size and one study, so I think there’s more work to be done there. But interestingly enough, there was no change in olfactory function. And the one other published study that was pretty robust also reported no change in olfactory function.
So, we have some suggestion that there’s an alteration of taste likely in the direction of diminished taste, at least measured by threshold and identification, maybe not so much by intensity. But we have this divergence now between taste and smell, and we’re going to have to look into that further.
The other point to make, we also measured appetite and food noise in the people that were using these medications, and we don’t find a big effect on appetite. And when you look at the literature, it’s actually a pretty minor shift in measured appetite. I know when people are on these drugs, they say, “Oh my gosh, I …”
Melissa Joy (40:35):
“I am not hungry.”
Dr. Rick Mattes (40:37):
I feel full longer and faster and so on. So, I don’t dispute their claims, the question is whether they’re reporting what we actually traditionally call hunger and fullness, or they’re reporting on something else.
When you measure hunger and fullness, the way we traditionally do that, give people a challenge meal and have them rate how hungry and full they are every say 30 minutes for several hours and so on, what you see is there’s maybe a 10, 20% reduction in hunger, a level that’s really just kind of at the cusp of being big enough to induce a behavioral change, that is alter your food intake. It’s not overwhelming.
And so, what I really think is going on is that these medications are altering food noise, and people are confusing food noise and they’re recording it as hunger, but in fact, it’s this decreased thoughts about food and what am I going to eat again? Who am I going eat with? What am I going to eat? How is it going to be prepared? All of these pervasive thoughts that are persistent in many people’s minds, and that these drugs seem to help abate.
Melissa Joy (41:50):
So, I did a recent episode on GLP-1s with Ana Reisdorf, and I’ve heard about food noise, and I always say I’m just so excited that these are words that we really didn’t have in our … I mean, separate words, but this phrase we didn’t have in our vernacular until the GLP-1s kind of brought this to light.
And as a dietitian, I’m excited that A, people who have experienced decreased food noise have this relief, and B, people who have no idea that that exists are kind of learning that that’s a thing. But Ana was talking more about food noise in the sense of mental load in a bigger way.
So, I was thinking of food noise, like you said, it’s like thoughts about food cravings, kind of obsessing about food. Not just I’m hungry, but how are you seeing food noise described in the literature and or how do you define it or think of it?
Dr. Rick Mattes (42:44):
The way I see it is, it’s more about food cue reactivity. It’s all of the external stimuli that we experience in everyday life. The people talking about food, seeing signs about it, smelling it when you walk past a bakery, just all of the cues that are unavoidable in everyday life, but prompt people to think about food in perhaps an unhealthy way. And these medications seem to reduce our responsivity to these external cues.
And there was a very nice study out of Japan, I think it was last year, that showed a decreased responsivity to external cues in people that had started these medications. I really think this is an important part of the study that we have to better characterize because it will have very clear and obvious therapeutic potential if indeed what I’m proposing is true.
Melissa Joy (43:46):
Very interesting. I love this food cue reactivity. I think that really depicts more … I mean, it’s not as media-friendly or whatever, but from a science standpoint, it really explains more what’s going on there.
This mental load that Ana and I were talking about is maybe what happens after the food cue reactivity is where then I see it as all the mental gymnastics about what I should or shouldn’t do. Not the, “Oh, I’m craving this, or I want this for dinner, or I’m planning this.” But sort of like the dieting mental talk is what I’m thinking that that’s decreased as well with these, because the food cue reactivity is decreased, right?
Dr. Rick Mattes (44:27):
The food cue reactivity is setting the stage for the necessity and the responsivity to all of those concerns.
Melissa Joy (44:36):
Yeah, very interesting. So, after we had our pre-interview call the other day, I saw that our colleague, Dr. Stu Phillips had posted on social media about this protein paper, and I saw that you were one of the authors on this paper.
So, this is a critical review, if you will, just published May 8th, and I’ll just read the title for our listeners – Examining Widely Held Propositions on Human Dietary Protein Needs and Benefits: A Critical Review of The Science That Shapes Both the Data and Our Understanding of a Macronutrient. And this review looked at commonly held beliefs or ideas about proteins such as how much we need, what types are best, if too much is bad for us, and so on.
So, tell us a little bit about this endeavor and the section you authored on satiety.
This was an attempt to answer a number of outstanding questions, and not just the community of consumers, but amongst clinicians, policymakers, and others. And there’s a lot of misinformation out there about protein, and it’s an important topic because protein seems to be on the front of people’s minds these days.
They’re putting protein into everything and are concerned that they’re not getting enough, and what types and sources and so on. It’s really a dominant discussion point when we’re talking about diets these days. And one of the questions that was posed was, is protein the most satiating of the macronutrients? And that was the particular point that I was asked to address.
Precisely, precisely, and is that true? So, I try to address it in sort of three stages. The first is we have to recognize that we’re not particularly good at measuring appetite. We all use that term comfortably thinking that we’re all talking about the same thing, and that’s not the case.
When I teach a course in this area, I often do a little mental experiment where I ask people to think, what’s the sensation you’re feeling if you’ve gone say six hours in the afternoon without eating, and everyone writes it down, and then you read it out.
And some people are saying, “Well, my stomach is growling.” Some people are saying, “I have a headache.” Some people are saying, “I feel weak.” All different sensations in all different parts of our bodies. And it leads one to question whether in fact, this is a common sensation at all.
When we measure it the way we do with these visual analogue scales, what you often find is that people give answers that they think you are expecting. So, if you say, “Please rate this on how hungry you are, and please rate how strong your desire to eat is now,” you would feel foolish not giving the same rating to both of those.
They sound like the same concept, but for people who study appetite, we define them very differently. Hunger is the sensation that motivates the initiation of an eating event, and it’s driven mostly by energy deficit. Desire to eat is the motivation to ingest in the absence of hunger. It’s driven more by sensory cues and cognition.
But if we don’t define these terms for the people we’re testing, they conflate them and give us answers that are not really responding to what we’re trying to get at. And I think the literature is full of data that is not high-quality data for that very reason.
So, before we can talk about protein being the most satiating, we have to figure out how to measure satiation. The second point is that we have to recognize that in the current environment, hunger and satiety are not actually that important in determining food intake. If you ask people why they initiate eating events, you get a whole array of responses. Hunger is one of them, but also boredom.
Nutritional needs, any number of factors. And hunger is only about 25% of the responses. And for fullness, the most common reason people say they stop eating, it’s not fullness. It’s “The food is gone,” they’ve eaten it all.
[Laughter]
We may initiate eating events based on interoceptive signals, but we may terminate eating events more by external factors like food availability. So, we could talk about protein being the most satiating because we’re thinking we can use this to manipulate energy intake, but we may be fooling ourselves because that satiety value may not really be as important in driving food intake as we’d like to believe.
But is protein more satiating measured the way we conventionally measure it? And I would argue no. And believe me, there are a lot of people who disagree with me, but one of the arguments that I use to substantiate my view is that if you put protein in a beverage, it has very little satiety value.
If you put it in a solid food, yes, that stimulus can be satiating, but it’s not the protein, it’s the vehicle that is driving that. So, I think we have to be careful. We so often confound what the food that’s providing the protein is from the protein itself.
I didn’t get through the entire article, but I did read that section. And one of the things that’s important is I think some of the research is looking at protein on its own or the protein food on its own. And then other research is looking at mixed meals and people typically eat mixed meals for the most part. So, that’s another consideration, right?
Yeah, absolutely. There have been a number of meta-analyses on this, and if you go back to the original papers, you find that in the meta-analysis are reports based on comparing, say milk with a sweetened beverage, and they talk about the protein then of the milk as being higher. And so, that’s why milk is more satiating than a sweetened beverage.
But those two drinks are entirely different conceptually why we drink them, what we expect of them, their appearance, their texture, all kinds of properties other than the protein. They also differ in fat.
And they differ in the kind of sugar that’s present. So, it’s not fair to isolate the protein in those kinds of trials. And many of these meta-analyses that come to the conclusion that protein is special are based on trials where protein wasn’t sufficiently well-isolated to be the explanatory variable.
I’ve got it right here. And the whole point was these are things that we hear all the time, let’s look and see what the research really shows, where is it strong? Where is it weak? Where is it plausible? Where is it not?
So, it’s just fascinating and I will put a link to this in the show notes at soundbitesrd.com. But like I mentioned, it’s like the optimal intake and there’s even stuff like per meal. And so, a lot of great information and amazing people that worked on this whole project with you. I’ll definitely put that in the show notes.
That’s really, really cool. What would you say, other than obviously the satiety part that you were working on, what was your biggest takeaway from this entire review and anything that kind of surprised you.
That it’s probably not necessary to have a high protein intake at every eating event; that at low and high levels of protein intake, it’s not serving an anabolic process. Yes, there are differences between protein sources, but one can meet protein needs with different kinds of protein sources, just it has to be done intelligently. Really, point by point, there are interesting observations. It is, I think a paper worth reading.
Yeah, I got about halfway through. But I mean, it’s a decent … I mean, I don’t want to say it’s an easy read, but it’s not a difficult read. And I do want to note that a lot of the groups who came to the table, there’s some protein industry folks there. So, whenever I’m interviewing a researcher or anybody who works with different industry, what do you say if somebody read this information and said, “Well, it was funded by the food industry?” What do you say to people in response to that?
Yeah, I would hope that we’re more sophisticated than that. That we judge science based on the science, not who funded it. Government funded studies can be very poor studies. They’re not good just because the government-funded them. And industry-funded studies can be excellent science, they can be bad science too. But the bottom line is the science, and I’ll just share an anecdote.
I was on the 2020 Dietary Guidelines Advisory Committee, and every time a committee is seated, there are people that will raise concern that some of the members of that committee have industry ties or done industry sponsored research, and so should be disqualified from service on that basis.
And that certainly occurred when the committee I was on was formed, and it reached a level of concern that actually ASN felt it necessary to respond to the vitriol that was being published. But then the committee came out with recommendations to reduce added sugars in the diet more than what the previous committee had recommended, and to reduce the amount of alcohol that people should be consuming.
And those same groups now all of a sudden thought we were quite wise and reasoned scholars to come to those conclusions. So, it shows they have an agenda. It’s not that they’re concerned about the science or that we’re incapable of conducting good science or interpreting the science. They were more concerned that we would just not support their a priori views on some of these topics.
Very good. Thank you for sharing that. I always appreciate hearing all the nuances involved in that. And I mean, in this case in particular, your section shows protein may not be the satiety factor that everybody thinks it is. So, it’s certainly not like everything was like rah, rah protein. So, it’s important to look at the strength of the study and the methods and all of those other things besides just funding.
Well, as we’re wrapping up, what is it that you want our listeners to take away from this conversation, whether they’re the general public or a healthcare professional, just thinking about the work that you’ve dedicated your career to and where things are in the appetite and behavior conversation today?
My career has been work at the interface between biology and behavior. And I have to say that the more I study biology, the more I believe in behavior, as the dominating influence on dietary behavior and so on.
We’ve tried innumerable manipulations of diet to achieve different goals and rarely do they meet our expectations. And so, the best advice has been probably is and probably always will be balanced, moderation and variety.
Looking for magic bullets has not proven useful thus far, and I don’t think it’s a good strategy going forward. I think what we need to do more is to engage communications experts and have them help us get that message about balanced moderation and variety out in a way that can be operationalized and is appealing to consumers. They would be better served by that.
Yes, balanced variety and moderation, it sounds kind of boring, it sounds kind of basic, but we need PR makeovers, and we need to make it a little bit more compelling and a little bit more meaningful. And I think that’s some of what was going on at the IFIC convening that we were at a couple of weeks ago.
So, I’ll put some resources in the show notes for everybody listening at soundbitesrd.com, and the protein paper and any other research articles that you think might be helpful for our listeners, I’ll throw links to those in the show notes. Thank you so much for coming on the podcast and sharing all of this interesting and important information.
For more information, visit soundbitesrd.com. This podcast does not provide medical advice. It is for informational purposes only. Please see a registered dietitian for individualized advice. Music by Dave Birk, produced by Jag In Detroit Podcasts. Copyright, Sound Bites, Inc. All rights reserved.
LISTEN, LEARN AND EARN
Listen to select Sound Bites Podcasts and earn free CEU credits approved by the Commission on Dietetic Registration (CDR) for registered dietitian nutritionists and dietetic technicians, registered. Get started!
Get Melissa’s Sound Science Toolkit here!
Partnerships:
Sound Bites is partnering with the Association of Diabetes Care and Education Specialists (formerly the American Association of Diabetes Educators)! Stay tuned for updates on the podcast, blog and newsletter!
Sound Bites is partnering with the International Food Information Council! Stay tuned for updates on the podcast, blog and newsletter!
Sign up for my monthly newsletter and episode eblasts so you never miss an update!
Listen on Stitcher (Android)
Install the Stitcher App
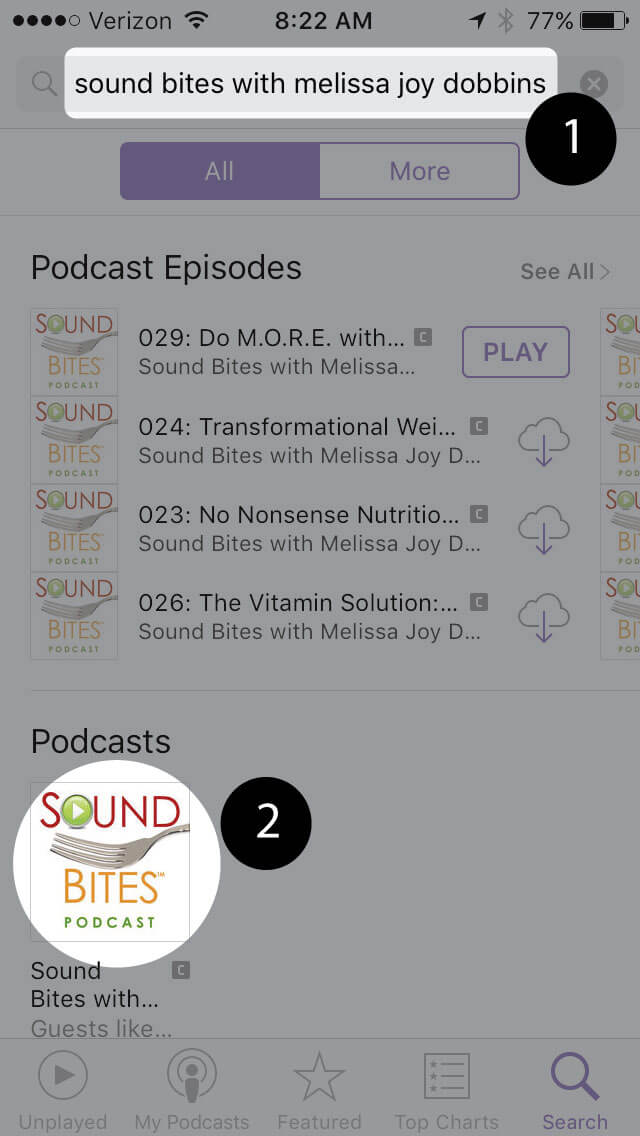
1. Search for “sound bites with melissa joy dobbins” 2. Choose Play Current Episode or Add to Playlist
Choose “Play Episode”
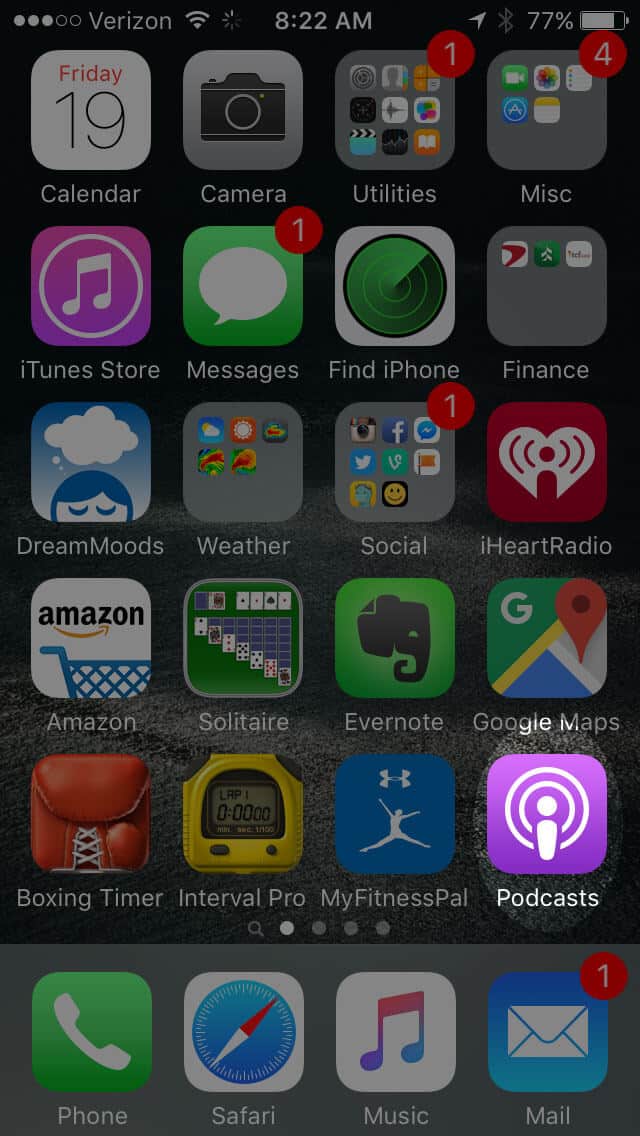
Subscribe & Review on iPhone
Open the “Podcast” app on your iPhone
Search for “Sound bites with melissa joy dobbins”
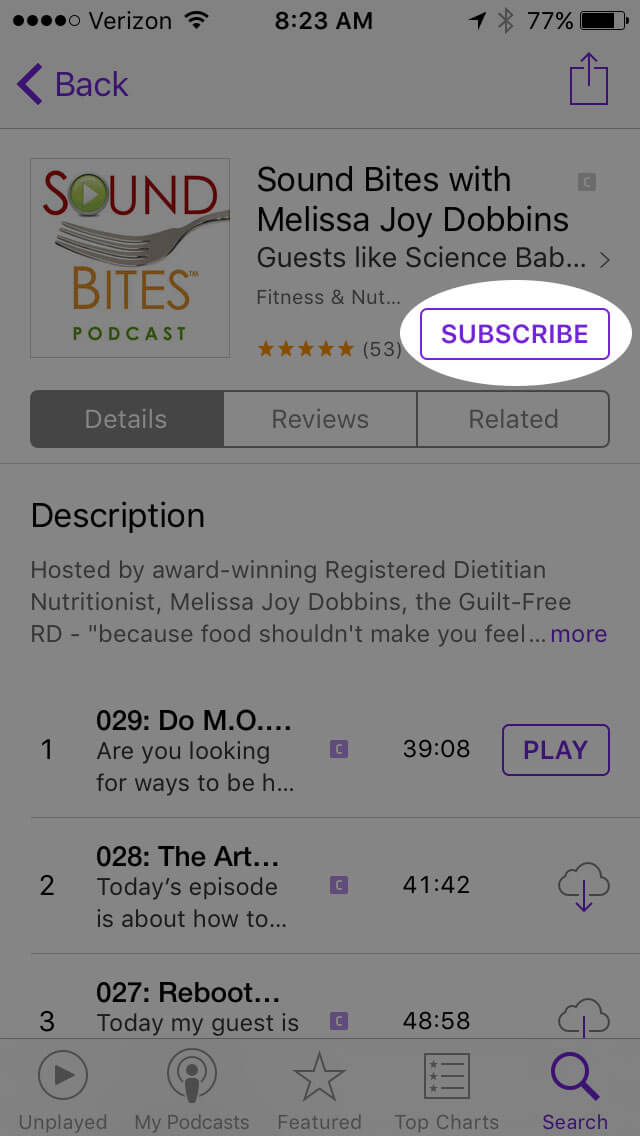
Open the podcast and click “Subscribe” and your done!
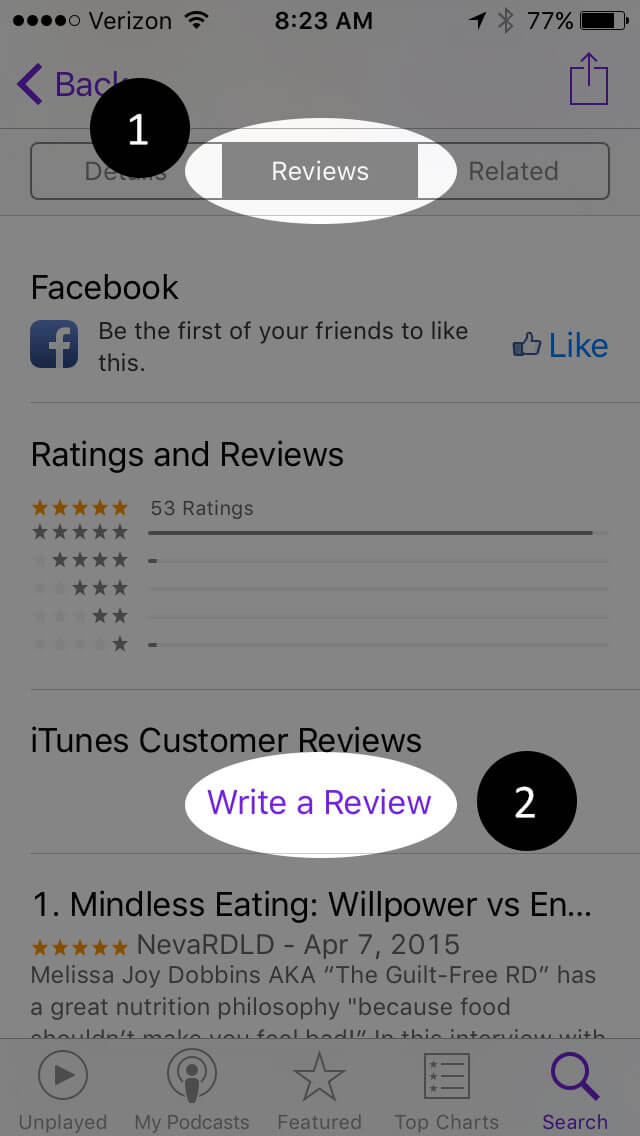
Write a Review
Click “Reviews”, then “Write a Review”.
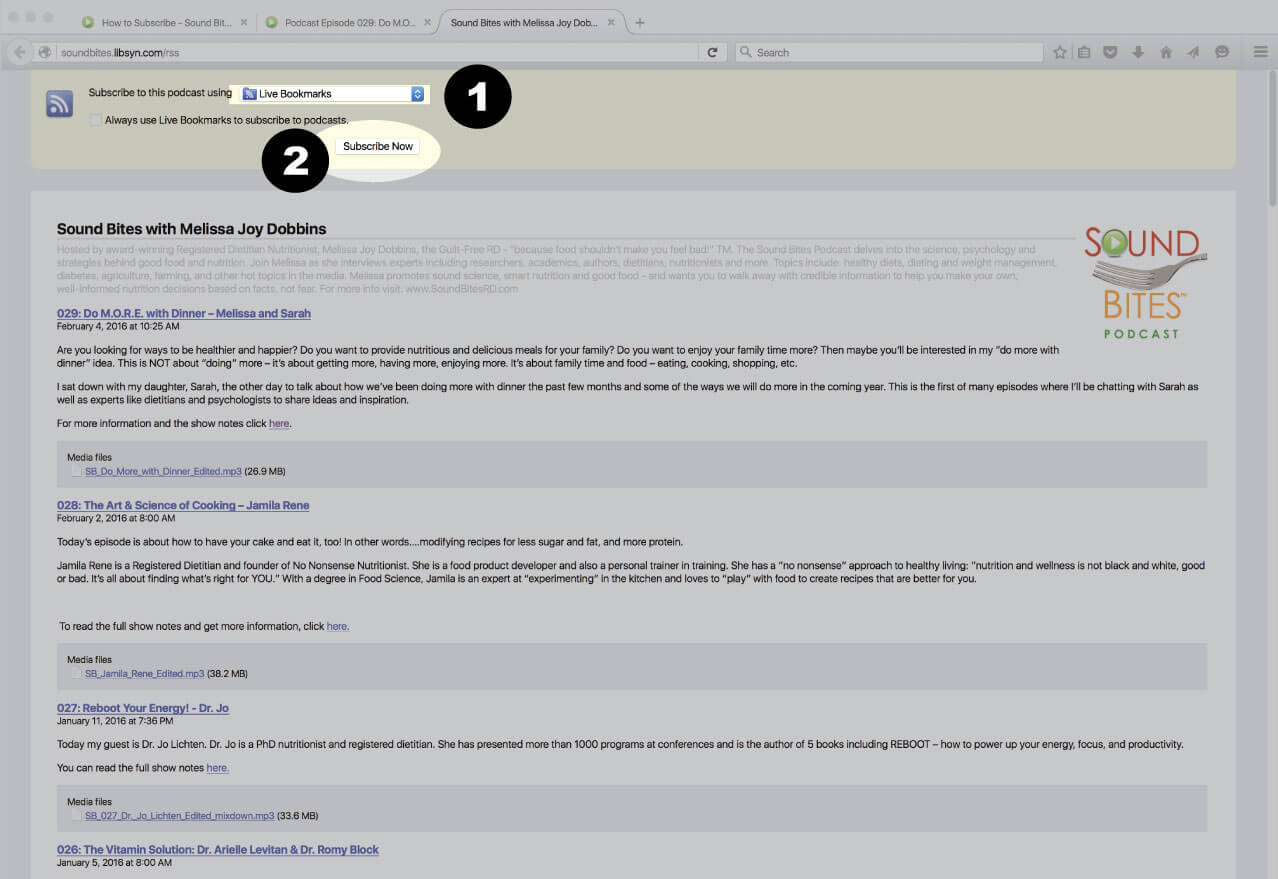
Subscribe via RSS Feed
Navigate to any podcast player . Click on the RSS feed icon.
Click on the RSS feed icon.
Click on RSS Feed
Choose which application you would like to use to receive the RSS feed
Click “Subscribe Now”
Confirm settings and subscribe.
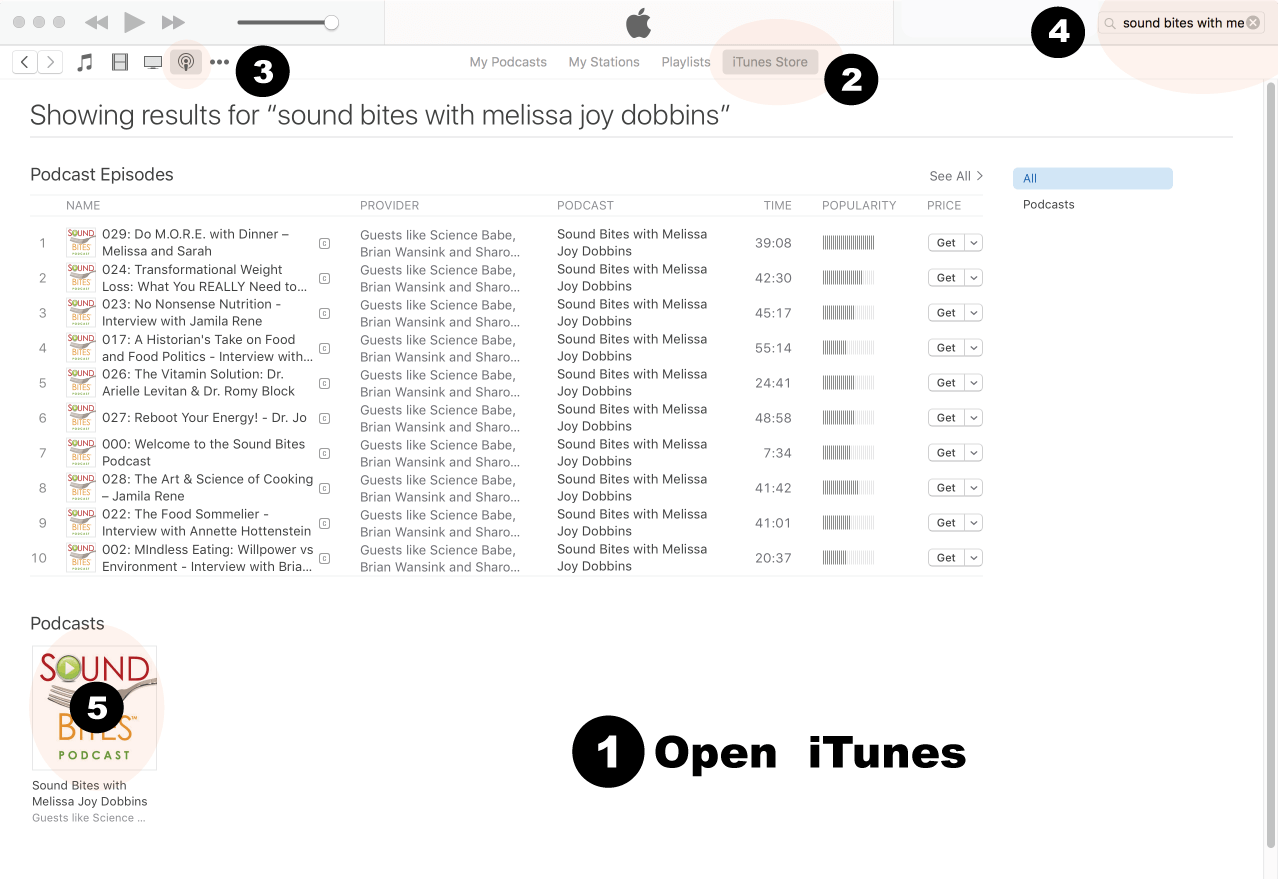
How to Review in iTunes
Open iTunes desktop application
Click iTunes Store
Click on Podcasts
Search for “Sound bites with Melissa Joy Dobbins”
Click on podcast image
Search for Sound Bites podcast in iTunes
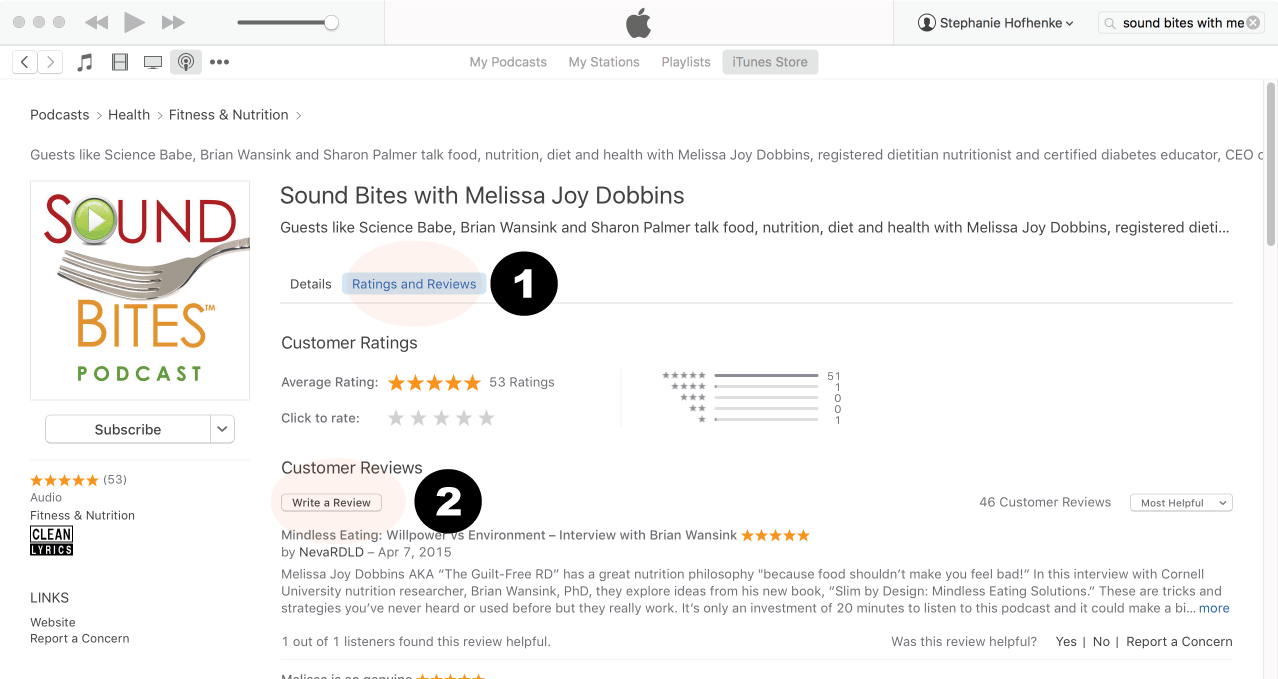
Click Ratings & Reivews
Click Write a Review
View reviews and write your own review.
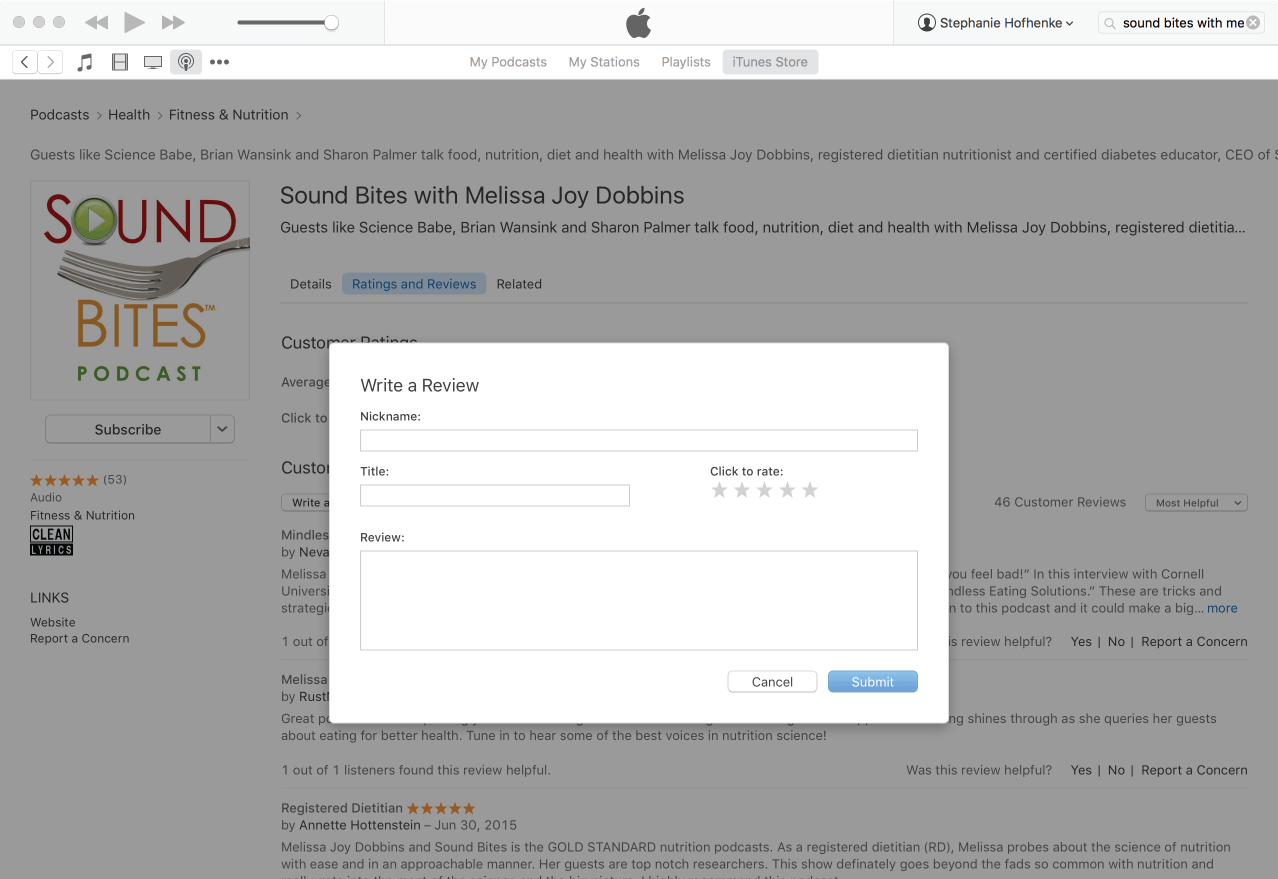
Write your review…. Thank you!
Write your review!
How to subscribe via iTunes
Click here to view the Sound Bites Podcastin iTunes, then click the blue “View in iTunes” button. This will open your iTunes application directly to Sound Bites Podcast. Click the “Subscribe” button, and your done!
 Dr. Mattes is a Distinguished Professor of Nutrition Science at Purdue University and Head of the Ingestive Behavior Research Center. His research focuses on the areas of taste function, hunger and satiety, food preferences, regulation of food intake in humans and human cephalic phase responses. He has authored over 300 publications. Dr. Mattes earned an undergraduate degree in biology and a Masters degree in Public Health from the University of Michigan as well as a doctorate degree in Human Nutrition from Cornell University. He conducted post-doctoral studies at the Memorial Sloan-Kettering Cancer Center and the Monell Chemical Senses Center.
Dr. Mattes is a Distinguished Professor of Nutrition Science at Purdue University and Head of the Ingestive Behavior Research Center. His research focuses on the areas of taste function, hunger and satiety, food preferences, regulation of food intake in humans and human cephalic phase responses. He has authored over 300 publications. Dr. Mattes earned an undergraduate degree in biology and a Masters degree in Public Health from the University of Michigan as well as a doctorate degree in Human Nutrition from Cornell University. He conducted post-doctoral studies at the Memorial Sloan-Kettering Cancer Center and the Monell Chemical Senses Center.