Celebrating over 1 Million Downloads and 50,000 Free CEUs on the Sound Bites® Podcast | NEW: Get 1 years’ worth of CEUs with the new 15-CEU Podcast Course
Weight Loss & Maintenance Insights from a GLP-1 Expert and User
In this episode, we explore GLP-1 weight loss medications, including emerging conversations around microdosing, the “mental load” of weight management, and what it really takes to maintain weight loss long term. Hear expert insights on how these medications work, what happens after weight loss, and practical strategies to support sustainable results. Whether you’re considering GLP-1 medications, currently using them, or supporting patients or clients, this evidence-based conversation helps cut through hype, misinformation, and confusion.
Tune in to this episode to learn about:
personal insights from a GLP-1 user who is also a dietitian
how GLP-1 medications work
new meds in the pipeline including oral versions
scams and frauds – meds that don’t work from patches to certain pills
pros and cons of compounded meds
the difference between “food noise” and “mental load”
the microdosing trend – what is it, does it work, what’s the controversy
GLP-1 foods – what are they and where are they
key mistakes to avoid
how to emphasize protein, fiber and fluids when feeling full
weird side effects and unexpected benefits
potential nutrient deficiencies and recommended supplements
considerations for long-term weight loss maintenance
the evolving role of the dietitian in patient care
how increased access is often hand in hand with decreased care
resources for health professionals and the public
Ana Reisdorf MS, RD
Ana Reisdorf is a registered dietitian, entrepreneur, and content strategist who has built her career at the intersection of nutrition, media, and online business. Before launching GLP-1 Hub, Ana ran a successful content agency staffed by a team of 10 dietitians, where she helped health and wellness brands create evidence-based, consumer-friendly content at scale. Through that work, she developed deep expertise in translating complex nutrition and health information into content that is both credible and engaging.
After years of building in the content and marketing space, Ana shifted her focus to create GLP-1 Hub, a platform dedicated to helping people navigate weight loss medications with practical, trustworthy guidance. What began as a new direction has grown into a multi-platform brand featuring podcast content, educational resources, social media, and a growing community centered on long-term success with GLP-1s. Ana combines her clinical nutrition background, editorial experience, and entrepreneurial mindset to cover topics like protein, muscle retention, side effects, lifestyle habits, mindset, and sustainable health beyond the scale. Her unique background as both a dietitian and business owner gives her a distinct perspective on what audiences need, what brands are looking for, and how to create content that genuinely connects.
Resources
Some links may be affiliate links. As an Amazon Associate, I earn from qualifying purchases.
These medications are life-changing. They’re helping people who have been struggling for so long, finally get to a weight that’s better. But then they also are being abused by people who don’t really need them, and I think that that continues the stigma for the ones who do.
Just this week, a neighbor said to me, “Oh, I work so hard to look like this, why do all these women just get to use this medication” and they don’t. And I understand her point of view but at the same time, like, “Why are all these women using this medication they don’t need?”
[Music Playing]
Voiceover (00:33):
Welcome to Sound Bites, hosted by registered dietitian nutritionist, Melissa Joy Dobbins. Let’s delve into the science, the psychology, and the strategies behind good food and nutrition.
Melissa Joy (00:56):
Hello, and welcome to the Sound Bites Podcast. Today’s episode is all about GLP-1 weight management medications. Now, I’ve done episodes on this topic before but we’re going to take a deeper dive today. And not only do I have an expert in the topic, but she’s the dietitian who is also a GLP-1 user, and she has a multi-channel platform where she talks all things GLP-1.
So, we’re going to talk about the questions and concerns about the medications, some of the scams and fake products that are out there right now, the microdosing trend (I have a ton of questions), and there’s GLP-1 foods, the role of the dietitian, which is of course, huge and so important and a lot of other things. This is also a video episode, so if you want to hop over to YouTube and check us out there, that would be great.
This episode is not sponsored and the best way you can support this podcast is to click the follow button wherever you’re watching or listening. That would be a great way to support the show and just help spread the word and get the word out there about new episodes.
My guest today is Ana Reisdorf. Ana is a Masters of Science and registered dietitian and founder of the GLP-1 Hub, a platform providing evidence-based nutrition guidance for people using GLP-1 medications. Through her podcast, YouTube channel, and educational resources, she helps individuals navigate weight loss, side effects, and long-term metabolic health with clarity and confidence.
So, welcome to the show, Ana.
Ana Reisdorf (02:34):
Thank you so much for having me, Melissa. I’m so excited to be here.
Melissa Joy (02:38):
I am so excited. Like I said, a lot of questions, a lot of … gosh, this is a topic that the more I learn about it, the more questions I have. So, buckle up everybody and here we go (laughs).
Before we jump into the topic though, I would love for you to share more about your background. You are a writer and you have quite a history of your career prior to this GLP-1 expertise and such a needed resource. So, please tell us more about yourself.
Ana Reisdorf (03:06):
Sure. So, I’ve been a dietitian for almost 20 years. It’ll be 20 years next year. And I did a lot of things in my dietitian career. I taught at the university, I worked in clinical, I helped people prepare for gastric bypass surgery, a lot of different types of things.
But about 10 years ago, I discovered writing. I had always kind of dreamt of being a writer, but I thought you had to write a novel, and that seems really overwhelming to try to write a novel. But with the internet and content writing and all of the SEO and all these things, that really exploded in terms of demand for health professionals to become writers.
And so, for 10 years, I was a full-time writer. I actually had a team of 10 dietitians that worked for me. And we would write content for brands, mostly supplement brands, but a lot of different things as well. We also did recipe development video, all of that.
But about two years ago, this little robot showed up, his name was ChatGPT, and that really started to decline. The demand for that started to decline. And at the same time, Google made some shifts to their SEO and how they were ranking things. And just a lot has changed in that industry, and so my work really declined.
But at that same time, I started using GLP-1 medication for weight management. I was an early adopter on it, and I started in 2022 right before it got approved for weight loss. So, about two, three months before that happened.
One day, I was in the shower and I was like, “I need to get a new direction.” My business was declining, what am I going to do? And at that point, I had already almost been on it for two years, on and off (we can talk about that), but I was like, “What if I started the hub for all things GLP-1?”
Because what I started seeing is the amount of misinformation and not a whole lot of RDs or even MDs talking about this in a reasonable way. And so, I took all of that knowledge that I had about writing and SEO and marketing and everything and switched gears and turned it into this.
So, I still do some writing because I still have some consistent clients that are hanging around. But this is my full-time thing now, is helping people be more successful in a more reasonable way while using GLP-1 medication.
Melissa Joy (05:35):
I love it: reasonable. And I have already learned so much from your podcast and I love your YouTube channel. So, yeah, this isn’t going to be a three-hour episode, but people, we’re just going to kind of scratch the surface. I mean, maybe take a deeper dive in some of the questions, but I feel so good that I can just tell people to just go to your channels and learn more.
And as we go through our conversation today, we definitely want to highlight the role of the dietitian is so important for both of us to really emphasize and clarify the opportunities and the responsibilities, and just the changing role of the dietitian so we can touch on that as we go through our conversation. And of course, any of your personal experiences that you want to share as we go through the different questions that I have, please do that.
And like I said, I have several episodes related to this, I’ll recap those at the end and give people episode numbers so they can scroll back and listen to those. But basically, I’ve talked about the basics, I have talked a little bit about if and when people come off for various reasons, what then — and actually, you have something new regarding that that we’re going to talk about as well too.
I just saw your newsletter, and we can share that about like okay, you’re going to really focus on this aspect because it’s such an important part of the puzzle. I should also say as a diabetes educator for over 25 years, I was familiar with GLP-1s with the use for diabetes. They work in all different ways, but if we could kind of just start with how do these medications work in the body and the different parts of different organs if you will.
Ana Reisdorf (07:15):
So, there’s two main medications on the market. It’s the semaglutide, which is Wegovy, Ozempic, and then the Tirzepatide, which is the Zepbound, Mounjaro. So, the Wegovy, Ozempic targets the GLP-1, which is a hormone that helps suppress appetite that pops in kind of like right after you eat, but it only lasts for a couple minutes, and it extends the life of that. It’s a peptide really, we should call it.
Melissa Joy (07:40):
It’s our natural hormone that gets released, and then the medication helps extend that.
Ana Reisdorf (07:44):
Exactly. So, it extends it to be high all the time, so you don’t really ever feel very hungry. The other medication targets another hormone as well called GIP. And so, it has a more powerful effect, seems that it causes more weight loss and more powerful effect overall. And there are more coming that target all sorts of other peptides.
And I’m not an expert in all of those because there are so many, but these medications are the ones that are currently on the market, and more and more are coming because we have a lot of different appetite hormones. So, that’s really one of the primary effects.
Another thing that it does is it helps control your blood sugar because as the food moves more slowly, you don’t have those spikes that cause hunger and the insulin and all of that kind of stuff. So, that’s why it was used for diabetes for such a long time because it does help control your blood sugar after meals.
But one effect that I think is most interesting is the effect that it has on your brain, and that it really impacts that dopamine reward system. And so, what people feel is much less food cravings, what we refer to as food noise, which is the constant obsessive thoughts about food and what to eat, and what you’re not eating and what you’re going to eat next.
And then also, it’s translating into addictions as well because that same pathway that talks about what we’re going to eat and what we’re craving and what we’re not, also applies to alcohol, smoking, gambling, all of these things. So, even that, people are seeing results in that area as well.
Melissa Joy (09:23):
Very cool. So, the food noise, you mentioned something in one of your videos, I think it was just released a few days ago that really expanded my understanding of food noise. And I’ve said this several times on the podcast before, I’m just so excited this wasn’t a term that we were using before. And now, it’s like people get it that this is a thing that some people just have a lot of this food noise, some people don’t, and it’s just more accepted and I think it’s really decreasing weight stigma.
But you said it was more than just the cravings and the sort of focusing on food and the hunger aspect. You call it mental load, I believe. So, let’s talk about that a little bit because I was sort of like, “Oh yeah, this is huge.”
Ana Reisdorf (10:12):
So, yes, I have food noise. I am always (even now, even now) thinking about what am I going to make for dinner? What am I going to eat? Where are we going to go eat on the weekends? I’m planning a trip to Japan this summer, I have a million restaurants tagged because all I care about is what are we going to eat? I might have to eat five meals a day while I’m there because I want to eat food. Like that is my thing, is part of why I’m a dietitian.
But at the same time, I spent a lot of my life thinking about is this the right food to eat? Is this the best food to eat? What else have I eaten? Will this food help me lose weight? What is the meal that could do that? What is the next diet I’m going to try? Am I going to track these calories, macros, da-da.
Like all of that dominated my entire life. It is the reason why I am a dietitian is because I wanted that secret thing, that secret tip that would finally allow me to lose the weight that I wanted to lose. And now, I don’t do any of that. And that is the most mentally freeing thing. I don’t sit there at night thinking, “Okay, should I try this diet? Should I do this?”
Melissa Joy (11:25):
What am I going to do tomorrow? Next meal? Try this, try that. All the mental gymnastics and the times suck that that is. I think that’s huge. So, that’s how I’m thinking about food noise now, is more of like the food noise/mental load because it’s huge. So, thank you for sharing that.
And you mentioned briefly about new medications and there’s something new every day. And we should clarify, like there are things in the pipeline that go have to go through trials and research before they’re approved and so on and so forth.
But the new big thing is the oral semaglutide, I think it is, the oral Wegovy. And you have, I think it’s a video, but it might be a podcast kind of like the pros and cons on that, and how some of the considerations with that. If you could just talk briefly about the orals and what you’re seeing there, that’d be great.
Ana Reisdorf (12:21):
Sure. So, there’s this oral semaglutide had actually been on the market for a while for diabetes under the name Rybelsus. And so, all they did was rebrand it for weight loss, and the dose is a little bit higher. So, it’s really the same. And it’s been on the market, and it came on the market in January and about 30% of GLP-1 users are brand new and are on the oral now already. I mean, it’s the end of February.
Melissa Joy (12:50):
30%?
Ana Reisdorf (12:52):
Yeah. So, it’s less expensive because it’s around $149 right now for the starter doses. So, that is less expensive than the branded of the injectables. And the main thing about it, which is the main con that I see is it has to be taken in a very specific way because of absorption. It doesn’t absorb very well when it has to go through the digestive system. When it’s injected, it doesn’t have to pass the digestive system, so there’s not those same issues.
So, the main issue is that is absorption and how it has to be taken first thing in the morning with exactly four ounces of water, 30 minutes before your first meal. And so, for me, personally, that wouldn’t work with my lifestyle just because I hit the ground running with children and things every day. But I know some people that are retired and don’t have that kind of schedule, and that’s perfect for them.
And then other medications too, if some other medications you have to take that way, and so you got to work the schedule out. But I think it’s a great option for people that don’t like injections, that want a cheaper option, and the results seem to be fairly comparable as the injections.
Melissa Joy (14:13):
Great. And I saw a presentation recently that showed that the symptoms are fairly comparable as well. I mean there might be a little bit of difference. And then I also heard recently that there are medications coming out that include something that is supposed to help preserve muscle mass. Can you talk to us about that?
Ana Reisdorf (14:30):
The Retatrutide, they call it the Reta on YouTube. And yes, I also belief it has glucagon in it, and it helps preserve or targets glucagon. I’m not an expert in this, but it will help preserve muscle and it doesn’t have the same effects as the muscle wasting as some of the GLP-1s do.
And so, it seems to be much more powerful, and people are losing 30, 40% of their body weight on it. And a lot of people in the trial have had to quit because they lost too much. It’s like bariatric surgery level weight loss, and it’s in phase three trials right now.
Melissa Joy (15:13):
And it tends to preserve the lean muscle mass. And I mean, would you say in general that part of that muscle mass issue is when people lose weight? I mean, when we lose weight, we lose muscle and fat anyway, but the rate of weight loss, like if somebody’s losing it slower and they’re doing strength training, I mean that can help preserve the muscle mass as well, right?
Ana Reisdorf (15:33):
Yes. And I think that we’ve really lost the story here in that in our country (not on this podcast) that faster is not better, and that’s what I keep trying to communicate. My personal goal was half a pound a week because I am going into perimenopause and I cannot afford to lose that muscle. And when I retire, I plan on going all over, and I have to be able to carry my suitcases and do the things that I want to do.
And I knew that if I started losing 8 pounds a month, 16, 10 pounds a month, whatever the people are losing, that that would affect me long term. And so, yes, it is due to people losing way too fast, having very unrealistic expectations about how quickly they should lose, having a goal weight that is unrealistic or just too extreme.
Not eating the protein, not eating at all, and not really thinking, “Oh, well now I don’t need to exercise because I’m losing weight with doing nothing.” So, I don’t know, I feel like we’re going really extreme and I’m actually very concerned with this Retatrutide because it does preserve the muscle, give you a six pack, you don’t have to go anywhere, do anything.
Melissa Joy (16:56):
It’s interesting.
Ana Reisdorf (16:58):
But the long-term effects of that I think are going to be quite detrimental. So, that’s what I keep trying to emphasize to the people but it’s very sexy to lose 10 pounds in a month.
Melissa Joy (17:11):
So, one more question about the meds. So, the GLP-1s first, we were like, oh, no longer just diabetes, we’re going to focus on obesity, weight management; my question was, are these newer medications just stronger? Is this just a higher dose? Is it kind of a mixture of all of that? I still don’t quite understand how the differences with the diabetes meds versus obesity.
Ana Reisdorf (17:37):
I know for the Wegovy specifically, the dose is higher than Ozempic, but it is the same medication. Just the FDA rules require if you’re going to use it for a different purpose, you have to rename it and change the target because it’s like a marketing thing. So, the Mounjaro and the Zepbound bound are the same medication, they’re just branded differently and marketed to different people.
Melissa Joy (18:01):
Great. And then there was one more thing (I think I saw this again on your channel), there’s like a patch. Oh Jesus, tell me about the patch or maybe we shouldn’t talk about that.
Ana Reisdorf (18:13):
Let’s talk about the patch because this is a cash cow. Let’s be honest, like this is the thing in the world right now, and everybody wants a piece of this market. And so, people are afraid of injections. So, there are many companies coming out with a variety of formats and selling them as GLP-1 patches, lozenges, drops, you name the format.
GLP-1 patch really took over on TikTok, and it’s called GLP-1 patches. It’s a little patch that you put wherever you want to put it. It actually doesn’t even have GLP-1 in it. It’s berberine, chromium, like a bunch of different vitamins, none of which can actually be absorbed transdermally.
So, they’re basically making you pay for a sticker to wear on your body, but then they get all these people that don’t really know or understand to promote it and talk about how they’ve lost … “Oh, I lost weight on it.” But we know the placebo effect is very powerful. So, I’m thinking it could be something like that, but the number of scams in this space is shocking to me.
Melissa Joy (19:26):
Yeah, yeah, yeah. And then we’re going to talk also about the whole gamut of qualifying with your insurance and getting it from your primary care doctor versus your doctor’s not receptive to it, so you go to something online or whatever.
I mean, like you said, there’s a lot of players in this space. And speaking of which, then the whole compounded medications, I have questions about those because I think those really came about when there was the shortage issue.
And I should just say these meds are a game changer for weight management, for obesity, for healthcare. So, there’s so much good about this, but yeah, we do need to understand the science and the risks and the scams and the frauds and everything like that.
So, let’s talk about the compounded medications. I mean, I assume that there’s just pros and cons about them, do you get this from your primary care doctor? Do you go to a med spa? What do we need to know in general about compounded medications?
Ana Reisdorf (20:25):
Sure. So, I would always want somebody to start with their primary care doctor because that person has their medical history, has all the information they need, and can determine if it’s appropriate for you or not.
Many primary care doctors will put in like a referral to the insurance to make sure or it’s like a prior authorization to get it approved hopefully by your insurance. And that’s going to be the best route, safest route, cheapest route. Now, a lot of insurances aren’t covering this or dropped it, especially at the beginning of the year. A lot of people had their coverage dropped.
Melissa Joy (21:00):
Yeah, you have a podcast episode on that.
Ana Reisdorf (21:04):
And so, people are looking for alternatives, and you can buy the branded medication directly from Eli Lilly, Nova Nortis. You can buy Wegovy directly from them, you can buy Zepbound or Mounjaro directly from them.
The issue is that the price is pretty steep. So, the Zepbound is going to cost you 300 to $500 a month depending on the dose, and then like the Wegovy pill is 149 right now, but that’s just for the starter dose, and I think it goes up closer to 300.
Melissa Joy (21:38):
And that you can buy directly from them also. That’s pretty safe, I mean if you can afford it.
Ana Reisdorf (21:43):
Yeah, I think that that’s ideal. That’s the ideal way to go. Your doctor can send them a prescription, or they will even help you find a doctor that will prescribe it for you and actually review your information. So, that’s the safest, best bet, I would love for everybody to just do that.
But that cost is quite prohibitive for many people. And that’s where the compounding pharmacies come in, and I think that they play an important role but there is an enormous amount of litigation around that.
So, if somebody wants to choose a compounding option, you want to be sure that you’re choosing a pharmacy that’s a 503A or 503B pharmacy that’s making the compound medication. And the only medication that is effectively compounding is the injectable.
If a compounding pharmacy is selling a pill that is not effective, Him & Hers just got sued for doing that by the FDA because they were trying to sell a compounded pill for $49 a month, and the FDA said, “This pill doesn’t work. You are scamming people,” and shut them down, and now they’re in a lawsuit with Novo Nordisk as well (laughs).
So, the only one as it is, the injectable and they have to personalize it in order to get around the rules. So, what they do is they make the semaglutide or the tirzepatide, and then they add things to it. Like right now I’m on one that has NAD in it because it has to be personalized to me so they can get around the rules because they’re technically not supposed to just replicate the same exact medication.
So, they add B12 to it, they add glycine to it, they add NAD to it, they add a variety of things to it to make it personalized, saying the patient needs it personalized for side effect management, whatever the heck else, and that’s how they’re getting around the FDA rules. But 503A, 503B means that it’s not FDA approved, but the FDA has oversight over those pharmacies, and if there’s complaints, they’ll look into it, they do inspections, that kind of stuff.
Melissa Joy (23:56):
And you have an article on your site with that and a link to that, so I’ll link to that in my show notes. I did see that.
Ana Reisdorf (24:02):
And then also another thing you can look at is if a pharmacy is legit script certified, and that’s a third-party company that will make sure that what they’re providing is legit script (laughs).
Melissa Joy (24:18):
So, that’s really interesting. I mean, so I’ve heard from a lot of people that their doctor’s not receptive to this. And until probably about a week ago, my understanding was between the insurance company and a primary care doctor, if you didn’t have a certain BMI to qualify or a lower BMI with two comorbidities that you wouldn’t qualify.
But then people are telling me, “No, like, you can go get this stuff in all these other places.” I’m like, “Okay, I’m trying to wrap my brain around all this.” So, with this increased access, is that potentially going hand in hand with decreased care?
Ana Reisdorf (25:01):
A hundred percent. It’s honestly shocking to me what is happening and how people are treating this the same as getting your Botox. Like I’m going to go, I will tell you every woman in my neighborhood — I live in a high rent part outside of Nashville, every woman in my neighborhood is on this medication.
Compounded; they can get at any med spa, the lady that does our Botox parties in the neighborhood offers it widely to every single one of them — not one of them qualifies.
Melissa Joy (25:36):
And how many of them are telling their doctors?
Ana Reisdorf (25:39):
They know better than to talk to me about it.
Melissa Joy (25:43):
Well, yeah, and I mean there’s this … so another video that I watched of yours, you were talking about your story and how you lost quite a bit of weight. And maybe you could share just briefly, like you said you’ve been off and on and kind of where you started and where you ended up.
But one of the things that you said was like, you’re like, “Nobody said anything about my weight loss,” and we’re in this culture now where you’re like, it’s not good to say anything about somebody’s weight. Like I always think if I see somebody, I’m like, “Oh, maybe they’re sick.”
Because I have a family member who was ill, and they lost a ton of weight. And another family member knew the reason, but they were still like, “Oh, you look great.” And I’m like, “Don’t know if that’s a good thing to say.”
Anyway, so there’s just a lot of considerations there. But the good thing is like do we have the right to just be like, “Oh, you’ve lost weight, you’ve gained weight.” Like there’s some generations a little older than us who will say, “Oh, you’re putting on some weight, you’re filling out or whatever.” But you were disappointed that nobody had noticed and you’re like, “I wish somebody had said something.”
So, talk to me a little bit more about your journey, your story, and some of this like should we comment on people’s weight or not or should we check in and say, “Hey, how are you?”
Ana Reisdorf (27:06):
I mean, I don’t think there’s a right answer, it’s just my experience. The only person who noticed was my mother-in-law, but she has a lot of things to say, so that was something. But I felt like I was finally-
Melissa Joy (27:20):
Your husband knew?
Ana Reisdorf (27:21):
Yes, I never hid it from anybody. I was always willing to talk about it, but I mean people don’t know, especially early on because I’ve been on it for three years, so then it wasn’t really common as it is now. So, I just was kind of like I’m finally accomplishing this goal that I’ve worked so hard to try to accomplish my whole life and nobody notices.
But as I think I became more open about it, especially once I started GLP-1 Hub, then people started really talking about it more and saying, “Oh, we notice this or whatever.”
Melissa Joy (27:52):
So, they noticed, but they just weren’t saying anything.
Ana Reisdorf (27:54):
Right. But it was just like at first, kind of, and I kept bringing it up. I’m like, “Look, my pants!”
[Laughter]
Melissa Joy (28:01):
So, your journey, your story.
Ana Reisdorf (28:02):
So, I started, it was on Mounjaro because the Zepbound wasn’t out yet because it hadn’t been approved for weight loss. I went through a telehealth company which ended up being purchased by Weight Watchers.
Melissa Joy (28:14):
Oh yeah, yeah. They’re doing a lot in that space now. I have a colleague who works with them.
Ana Reisdorf (28:19):
And at first, I had a coupon, so it was like around $500 a month for the medication because Eli Lilly was putting out this coupon. And so, I did it for four months and I lost about 20 pounds and I was like, “I’m alright here.” And the medication went up to $1,500 a month because the coupon ran out, and I was like, “My husband’s going to kill me if I spend 1,500. He’ll be like go to the gym more, get a trainer, it could be less than that.”
So, I stopped, and then I’ll be honest, I kind of had a good time summer that summer. I was at the lake, hey, get out, drinking beers, eating nachos, doing whatever things I was doing. And I didn’t really notice that my portions were slowly getting bigger and I wasn’t being super diligent about the habits that I probably needed to put in place.
So, I quit in March, by September that year, I gained it all back, and I was like, “Okay, I know what I did wrong, I’m going to try this again because I can’t just be hanging out, having a good time, being a party girl at 45-years-old.”
So, I went to a med spa, and I got on compounded semaglutide, which was cheaper. It was about $400 a month for that. And I lost it again through the holidays, and then because of the cost, I went off, and I was much more diligent that time. I didn’t gain all the weight back, I was really, really being cautious. But by September again, I had started seeing, like I had gained like five pounds, and I started seeing the writing on the wall.
So, I met with one of our colleagues who is a weight management expert, and she was like, “Look, you can exercise an hour and a half a day, eat all this protein every single day, worry about this for the rest of your life, or just get back on the medication.” And I was like, “You know, you’re right.”
And so, at that time, luckily my husband had switched jobs that summer and it was now covered by my insurance. And so, I was able to get on for $25 a month. I lost more, so now I’m at a 40-pound weight loss where I am right now, which put my BMI finally just right below that 25 mark which is where I wanted to be, and have been maintaining on one of the lowest doses.
And then my husband lost his job in November, so now I had to switch to a compound which I’m paying out of pocket for. But for me, it’s not the stress and the mental stuff that I have to think about, doesn’t seem worth it with all the other demands in my life. It’s just not something I want to do.
Melissa Joy (31:02):
Yes, thank you for sharing that. So, I have questions about the lowest dose and we’re getting into the microdosing. But I say this a lot on the podcast, and it’s one of the biggest frustrations I guess in my career, especially as a diabetes educator, is this anti-medication, this fear of medication and this just anti-medication sentiment.
People who go on blood pressure medication don’t typically say, “I got to get off of this, and if I don’t, I’ve failed and whatever.” It’s very common in the diabetes world and now we’re seeing this in the weight management world.
And I feel like that’s a weight stigma, that’s a, if I am on this medication, I wasn’t doing what I’m supposed to be doing, and I’m failing, and I would love to see that change. And for people with diabetes (and I’m transitioning into telling people with weight management about this), this medication is helping your body do something that your body was not able to do on its own.
And whether it’s the insulin resistance or all of the different, I think it’s like 11 or 12 different parts of the body that the diabetes medications, different medications can work on. And trying to get them to understand sometimes like, “Okay, you’re on three different medications because these three medications do different things and it’s a progressive disease, so your dose might continue to go up over time.”
And that’s different from the obesity or the weight, but that’s one of the things that I see with the GLP-1s. And of course, there’s the GLPs and stuff, we’re just calling them GLP-1s — is they’re really intended to be long term because they work while you’re on them, they stop working when you go off.
And like I said, I’ve done some episodes on there’s a variety of reasons people go off. You’ve talked about cost, there’s side effects. Some people just don’t tolerate them. There’s a variety of reasons, but a big reason some people go off is because they don’t want to be on them long term. We need to address the realities of okay, if people go off for whatever reason, how can we support them?
And I appreciate your honesty and sharing because you talk about this, these are the mistakes I made, this is what I learned, and this is why you’re helping people maybe avoid that step or be more informed going in. So, is there anything you wanted to say about that? I mean, you kind of came to it in your own way that this is going to be a long-term tool for you.
Ana Reisdorf (33:33):
And at the time I started, I didn’t understand that. I’ve been working as a content writer for 10 years; I am not a clinician, even now I’m not a clinician. And I didn’t understand how it worked. I thought it was like phentermine, I’d done phentermine like 10 years before. I did phentermine, it kind of wears off after a while, then I got off phentermine. So, that was my thought about it.
Melissa Joy (33:54):
I think a lot of people think that too. They don’t know that it’s a long term, right?
Ana Reisdorf (33:59):
Right. So, that was kind of how I was thinking about it. And then like $500 to $1,500 is an impossible jump for nearly anybody. So, it just wasn’t really an option, but I think that people are starting to understand more and more that obesity is a chronic disease that is going to need some degree of management.
And yes, just recently on my podcast, I interviewed Dr. Jim Hill and Dr. Holly Wyatt, and they are experts in weight maintenance. But I’ll be quite honest, I read their book and I was like, “I can’t do this.” I couldn’t possibly do what they’re recommending, and their book is about getting off the medication. But with my life and the demands of the things that I need to do, I wouldn’t be able to do what is required. And so, I take a lot of hate for it, but-
Melissa Joy (34:54):
A lot of hate for?
Ana Reisdorf (34:56):
For not wanting to do all of the things. Like just today somebody was like, “If you had changed your relationship with food, if you were willing to put in more effort, you would be able to do this, you’re just lazy.”
Melissa Joy (35:11):
Okay, like I want that stuff to go away. Somebody said something — well, because we’ve heard all like, “Oh, it’s a shortcut.” I’m like why shouldn’t weight loss be easier? Why should it not be easier to lose weight? I’m like I don’t understand. It should be easier to manage your blood sugar, it should be easier to manage your blood pressure, I don’t understand. Why does it need to be hard? That really makes me mad. That really makes me mad.
And I will say, I’ve had Jim Hill on the podcast a couple times, and I just met Holly at a conference and I know the name of their book is Losing the Weight Loss Meds, which as a writer, you know they did not come up with that title, it’s the publishing house. And she did tell me that the publishers wanted the pen, the injectable pen on the cover to be crushed and they were like, “No,” they fought against that.
You can put zero on there because they make it very clear if you can stay on the medication, do that. But if for whatever reason you’re coming off, this is what it looks like. And this is partly why we need to help people understand it shouldn’t be so hard. That’s the reality of it, it’s hard.
Early on in my career, I started off in clinical, but I was focused on weight management and eating disorders and I became an outpatient dietitian, and I got so burnt out, I’m like, “I cannot help these people, this is hard. This is really hard. I’m going to have to get a degree in counseling.” And then I found diabetes, and I was like, “Oh (laughs), I can help people. They can make a little change, and I can help them not be so fearful.”
And there’s just a whole other layer to that where it was just very much more empowering, and it’s just a whole different disease. But I also became a dietitian so that I could make sure that I would know how to manage my weight.
And we’re not alone, there’s a lot of dietitians who’ve done that. But it just makes me mad that people are like, “If you do this, if you do that …” Like these people, first of all, it’s none of their business; second of all, they don’t understand.
Ana Reisdorf (37:25):
No, they don’t. And it’s frustrating (and I shouldn’t listen to YouTube commenters) when they think, “Oh, you, you are just eating at McDonald’s all day.” Like “I’m not.” And even if I was, it’s my decision too. But there still is a definitely you should just try harder.
But at the same time, I feel like these medications are life changing, they’re helping people who have been struggling for so long finally get to a weight that’s better. But then they also are being abused by people who don’t really need them, and I think that that continues the stigma for the ones who do.
Just this week, a neighbor said to me, “Oh, I work so hard to look like this, why do all these women just get to use this medication” and they don’t. And I understand her point of view, but at the same time, like, “Why are all these women using this medication they don’t need to do something.” I don’t know. There’s no right answer here.
Melissa Joy (38:26):
This is definitely opening up a whole different dynamic and conversation. And I saw one of our colleagues had a YouTube video on this where I was like, “Oh, this is food for thought.” I interviewed a GLP doctor and it’s episode 300.
And one of the things that she said to me or just said on the podcast that really stuck with me was, if somebody is obese and they take the medications, even if they get into the normal BMI level, they still have obesity.
And it’s like, oh yeah, just like with diabetes. If you’re managing it and your blood sugars are within normal limits, you still have diabetes. I mean, people could say they’re reversing it, whatever. I mean, you still have the disease, it’s pathophysiology. I’m like that is so true.
So, another reason to stay on the medication if you can, but let’s say somebody is in the overweight BMI, they’re not quite too obese, they’ve been struggling, they can’t get to the normal weight. They still have something, they have overweight, there’s still some pathophysiology there.
So, do we wait until that person gains weight and gets into the obese category or has the comorbidities or whatever, or do we nip that in the bud and help them get to a healthier weight? I don’t know. What are your thoughts on that?
Ana Reisdorf (39:58):
That’s where I struggle as well because for perimenopause for example, I have a friend who suddenly gained 25 pounds overnight and it pops her just right into the beginning of that overweight category where she had always been. That was her normal weight and she used them to get back to what she considered her normal weight.
So, I don’t know if there’s a black and white sort of answer, but at the same time, I think people are taking it so extreme, and it’s fueled by financial gain. When I was looking for a new compounding pharmacy, I signed up for one of these very popular ones, one of the most popular ones to see what the price would be and if I could get it, and they told me to lose another 25 pounds on their intake form.
And my BMI is 24.8 and they show me this graph: “If you sign up with us, you could get to 130 pounds,” and they had this little thing with it by June or whatever that they were promising me. And so, that kind of stuff is fueling unrealistic expectations, but I don’t know the answer.
Melissa Joy (41:09):
I’m like, “What?” Oh, because then they make more money, sorry. I’m like, “What (laughs)?”
Ana Reisdorf (41:14):
So, should we wait until people get into the obese category to give them the medication? Should we help people that have a normal BMI and just not happy with themselves accept themselves more? I don’t have a black and white answer. It’s complicated.
Melissa Joy (41:31):
So, microdosing: what exactly is microdosing? I thought it was just small amounts or like cycling, but explain to me what this trend is and what it really means.
Ana Reisdorf (41:44):
Sure. So, it’s really just using small amounts typically below what even the starter dose is for some of these medications, and you can really only do it with a compound. And so, the medication has a lot of benefits outside of weight loss. It helps reduce inflammation. I have a patient or an audience member that’s using it for migraines. I just interviewed a doctor who uses it for a variety of pain management issues.
So, you can do these smaller doses for people who maybe don’t need to lose weight to get some of those additional benefits. Or maybe if somebody doesn’t need to lose that much weight or if they’re on maintenance or they don’t tolerate the medication and have a lot of side effects. So, it could be a lot of different things, but it does typically require compound medication because the dosages of the prescribed of the branded kind don’t come that low.
Melissa Joy (42:38):
Like in the pen. In the pen, it is what it is. That makes sense. So, I heard that based on the research, there’s a therapeutic dose. So, I know with diabetes, if somebody’s going to start on metformin, they start on 500 milligrams a day. And that’s not a therapeutic dose, the therapeutic dose is 500 milligrams BID or twice a day.
So, like you said, like a micro dose could be lower than the starting dose. I assume the starting dose isn’t even therapeutic. Could people benefit, like you said, benefit from a small amount? Like even though it was not the amount that was in a research trial? Like I don’t understand why people are talking about that.
Ana Reisdorf (43:22):
It seems that they can. Some physicians that are well-versed in this think that the doses, even the starter dose is too high for a lot of patients, and they’re wanting to be more flexible about the doses. This is not really evidence-based, there’s no protocol that says do one milligram of semaglutide for this. It’s more a lot of physicians are kind of taking that into their own hands because they can, and that’s what I’m kind of seeing in this space.
Melissa Joy (43:51):
They’re kind of testing it out and playing around with it. I attended a webinar, it was definitely over a year ago. It seems like now that they’re definitely ramping people up more slowly, they kind of learned like they used to start people at a higher dose.
Ana Reisdorf (44:09):
So, it’s supposed to be titrated every four weeks. And when I first started, that’s what happened to me. Like I would say, “Okay, well, I lost five pounds this month,” and they were like, “Up to the next dose, up to the next dose.” So, I got to a point where I could barely eat, and I was miserable because I like eating, and I hated it. So, that was another reason why I quit.
But I think that most physicians are understanding now that there’s no benefit to doing that. If the individual is seeing results from a lower dose and not having any side effects, there’s no reason to keep going up because once you get to the highest, there’s nowhere else to go.
Melissa Joy (44:45):
Right, right. And then I would think for like, let’s say like you reach your goal weight that you would probably cut back a bit, okay, that’s very logical, that makes sense.
So, we hear a lot about GLP-1 foods. So, what are these foods, do we even need to know, and what do we need to know about GLP-1 foods?
Ana Reisdorf (45:06):
Sure. So, there isn’t a specific definition. I actually interviewed somebody on my podcast who is working on categorizing different foods and making them GLP-1 friendly so that companies can use the specific definition for different food categories, so that is kind of coming down the pipeline. But it’s really not magic, it’s foods that are high in protein or high in fiber, nutrient dense, lowering calories. But right now, everybody’s looking for that.
So, I think that a lot of companies are trying to make that, and I’ve even seen at restaurants, chain restaurants. The other day I went to a California Pizza Kitchen, and they had a whole new high protein, low volume menu, 40 grams of protein for this burger salad thing. And even the Olive Garden had a whole section of all my favorites, smaller portions, 600 calories or less.
So, it is influencing everything, every food industry, every type of food. Every restaurant is thinking about, how can we make smaller portions higher in protein. It’s good for everybody, not just on GLP-1, but it is a marketing thing.
Melissa Joy (46:21):
But I’m so glad to hear that though because really, restaurants like the portions are usually ridiculous. Like oh my gosh. So, GLP-1 foods or GLP-1 friendly foods would be foods that … protein fiber, foods with nutrients that people really need because they aren’t eating as much, so they really need to pack in the nutrition.
Ana Reisdorf (46:43):
Exactly, and lower portion size.
Melissa Joy (46:46):
So, speaking of that, like we do encourage people to have more protein, have more fiber, and stay hydrated because these medications can dehydrate you.
Ana Reisdorf (46:54):
So, not dehydrate you, it can reduce your feeling of thirst.
Melissa Joy (46:59):
So, I mean, protein, fiber, and fluids are very filling. So, how do you balance that? What do you recommend for people who are like they’re trying to do that but they’re getting full, and it sounds like the portion is the key from what you just said.
Ana Reisdorf (47:14):
What I try to focus on is the nutrients that I know that I need and are most important. So, you want those meals to be as nutrient dense as possible. So, the way I think about it is what is my protein? And sometimes, it can be … especially the days after my shot, I don’t feel as hungry, sometimes it might just be a protein shake. There’s a lot on the market that provide quite a significant amount of protein, but at least it’s something.
Then when I feel like I can have a little more, I go to fruits and vegetables next because we know that that’s where a lot of our micronutrients live and our fiber. I recommend that people try to eat a minimum of three meals a day that might not give them quite enough. So, those couple of small meals or snacks throughout the day — to wait until you’re hungry is not going to work because you’re not going to ever get hungry, not in the same way that you were before.
And so, you have to time it. I never ever skip a meal. So, I eat my breakfast at 7:00 AM, I eat my lunch at noon, I eat my dinner with my family at five. Like you have to just eat whether I am hungry or not, because I can’t wait on that to decide if I need my nutrition.
And so, that was a mistake that I made at the beginning because I wasn’t hungry. So, I’d make me a nice iced coffee and it’d be two o’clock, and all of a sudden, I’d feel my blood sugar actively drop. Like I’d start to feel super jittery and shaky because all I had was iced coffee all day. I lost muscle. My kids were making fun of my jiggly arms. I started not feeling my best, my hair fell out.
Melissa Joy (48:47):
Well, that’s not good.
Ana Reisdorf (48:48):
That’s what I want to prevent other people from doing, is that we really need to focus on the nutrition as much as we can, and not just have iced coffee all day.
Melissa Joy (49:00):
For sure. And you have a video on how to get more protein, so I’ll link to that as well because I didn’t watch it yet, but I know that it’s got good stuff in there.
Oh, you mentioned micronutrients, talk to me about this a little bit because we don’t hear as much about this.
Ana Reisdorf (49:14):
We should. Because yes, I think that everybody got the protein message. I think everybody’s got the protein.
Melissa Joy (49:21):
There’s a war on protein (laughs).
Ana Reisdorf (49:23):
I don’t really understand the war on protein. I literally have protein chocolate sitting in my pantry right now. There is plenty of protein. But the micronutrients is really what I think is missing. There was a study that just came out that found that GLP-1 users are deficient and are not getting enough vitamin D, which is most of the population B12, iron, calcium.
So, there are a lot of potential micronutrient deficiencies, and I think that every GLP-1 user needs to take a multivitamin at a minimum. Not a multivitamin in lieu of eating, but a multivitamin just to try to cover some of those bases. I even saw in the New York post last week, people are getting scurvy. Now, you and I know how hard it is to get scurvy, you really got to try. And so, a multivitamin will take care of that very easily.
Melissa Joy (50:19):
Yes, okay, good. I was going to ask you about supplementation. Just a couple of other questions. I think we’ve covered everything. You have a video on like seven weird side effects. Do you want to just briefly address a couple of those?
Ana Reisdorf (50:34):
Yeah. So, something I kind of talked about was like the lack of or the decrease in feelings of addiction. So, people quit drinking, like quit smoking, they just have no real addictive desires because all of that kind of goes away. And I actually interviewed an addiction medicine doctor about how he’s using that in his practice, GLP-1 at low doses.
Another thing that I personally noticed, which I thought was real weird, was I used to get horrific bug bites all summer. My legs were covered. Not anymore. I thought maybe the bugs don’t like me anymore, but this doctor told me it has to do with the activation of the histamines and it’s affecting that whole system as well.
Melissa Joy (51:18):
It’s interesting.
Ana Reisdorf (51:19):
It is interesting. It’s just observational.
Melissa Joy (51:23):
And of one — well, your doctor said there’s a mechanism.
Ana Reisdorf (51:25):
There is and then feeling freezing cold all the time. I think that has to do with the body fat loss, but the cold is actively painful for me now. I have to move to Florida very shortly because I cannot continue with these winters here.
Melissa Joy (51:44):
Come to Chicago.
Ana Reisdorf (51:45):
Oh gosh, no, no, no.
[Laughter]
So, there’s just these interesting things that people are observing. One that I find particularly interesting is kind of a lack of interest in things, just like a meh feeling. And I think that has to do with the dopamine addiction kind of spiral, and that people are feeling not that motivated.
I found that last year, I was really struggling with that, but I don’t know if it was seasonal depression or really that. But I just kind of felt like I don’t want to do anything, hang out with anybody, do anything. But that seems to have improved, at least for me, but people do report that they just feel kind of flat.
Melissa Joy (52:24):
Yeah, I can see that. And also, just if they’re running high and they’re sort of come back to normal level, that can be a change as well. I had a patient — I do a little bit of work with a concierge program that sees people with prediabetes and diabetes. And they said they had started on the GLP-1 and they said they had trouble with exercise like the day or two after the weekly shot.
And I mean, obviously we know exercise is so important, especially for weight loss maintenance and for overall cardiovascular health, and our bones and our muscles. So, we don’t want these people like, “I’m losing weight, I don’t need to exercise.” We want them to have some healthy exercise. She said that she felt fine. Like if she wasn’t going to work out, she felt fine. And even in the low to moderate part of the exercise class, she felt fine.
But as soon as it moved up a bit, she just felt like, “Oh my gosh, I’m so out of shape, or I’m just feeling fatigued or not short of breath.” I’m like, “Were you short of breath? Is this dystonic exertion?” She says “No, but I just don’t have any stamina.” Have you heard this?
Ana Reisdorf (53:35):
I think it’s probably just lack of calories. Because those first couple of days really is when the most appetite suppression is happening. And I will say that I feel pretty gassed towards the end of my workout too, especially if I didn’t eat as much the day before, which makes total sense.
Melissa Joy (53:52):
Yeah, yeah, yeah. Your glycogen stores are depleted and everything. So, because we know these medications have been used for two decades with diabetes and they’re not different medications, maybe higher doses — I mean, we say, well, we don’t have any long-term data on the safety or efficacy (I mean, like long-term). What are your thoughts on that? Do you think we’re going to see anything down the road where, oh you know, anything above this dose or this duration could be of concern?
Ana Reisdorf (54:26):
I think that there’s a possibility of that because there are those lawsuits pending on the medication of people who’s had very severe side effects. And I don’t know how all that’s going to really shake out what is going to come from that.
And I mean, 20 years of data is pretty good. There’s plenty of other medications that we use and that don’t have that level of data. But what does it mean for somebody to be on this for 50 years? I interviewed a doctor who’s a pediatric obesity specialist using it in patients down to 12-years-old. So, what does that mean-
Melissa Joy (55:05):
Something I hadn’t thought of.
Ana Reisdorf (55:06):
For somebody who’s going to be 80 and still on this medication for that long? I don’t think we have all the information on that kind of thing.
Now, there is one study I believe that found that long-term use of this medication does make your body stop producing the GLP-1 on its own which is why maybe people report like really major hunger when they get off. But I think we need more research before we say can it come back? Is that a long-term thing? Does it happen in everybody?
Melissa Joy (55:40):
So, as we transition into this new thing that I want you to share with us, so when it comes to weight loss maintenance, like we said, like if you could stay on the medication, stay on the medication; if you do come off for whatever reason, do you have any … like you said, there are things that you are like I can’t do all of that. What would you say to somebody who has to come off for whatever reason?
Ana Reisdorf (56:02):
I think it’s about monitoring. That’s really what I got from Dr. Hill and Dr. Wyatt’s book, is it’s about really monitoring and closely watching what you’re doing. And then the exercise piece, especially they told me straight up on my podcast, “You need to move more and stop sitting at your desk (laughs).”
Melissa Joy (56:21):
You in particular?
Ana Reisdorf (56:22):
Yes, me in particular, yes. I was like, “You guys, I’m really good about going to the gym every day.” And they’re like, “Yeah, but you sit there all day, so you’re doing nothing.” And I’m like, “Thanks, guys.” But I think that that movement piece, that regular all-day movement is really a key point in weight maintenance, but that’s unfortunately not how we live.
Melissa Joy (56:43):
Right, right, yeah. And Dr. Hill and Holly Wyatt have spent their entire careers studying weight loss maintenance. They founded the Weight Control Registry where they monitor people who have kept the weight off and what has worked for them. And I remember one of the first things I ever learned from Dr. Hill was that diet drives weight loss, exercise drives weight loss maintenance. So, just putting that out there, yeah, such a big part.
Any other thoughts? Well, okay, so you have this new steady state newsletter: maintenance and mindset on GLP-1 because I think it was just the other day, I got your newsletter, and you’re like, okay, so this is like something we need to talk more about. And so, tell us how people can sign up for this newsletter, but what you’re going to be focusing on, the maintenance part.
Ana Reisdorf (57:36):
Sure. So, what I have realized is a lot of my audience has already been on the medication for six months, a year, maybe even longer. So, what they are really wanting is not how many grams of protein do I need? If they don’t know that by now (laughs), I don’t know what to say. But now they really want to understand what does this mean long term.
So, that’s what I’m trying to focus on is like how could you continue to work on those habits? How can you continue to make this something that’s going to increase your longevity long term? How can we focus on actual health?
Because I think that maybe they’ve reached their goals or close to their goals or whatever, but maybe they’re still not able to implement all of those things. So, that’s what I’ve kind of shifted to. At first, I was really providing like, here’s how you start, here’s what you do, but now I want us to talk about what it means to be on this long term.
Melissa Joy (58:30):
Great, excellent. I want to hear your kind of bottom-line takeaway for people, and knowing that my audience is a mix of the general public and dietitians and other healthcare professionals. And then I want you to share where people can find your multi-channel platform and all the places that you are.
Ana Reisdorf (58:45):
Sure. The bottom line is eat, please eat, please eat nutrient dense foods. So, try to get to some weight that is a random goal that you’ve chosen. Work with a dietitian to really focus on your health and what this means for you to be 80 going on that cruise that you want to go on, so you can carry your bags. That’s what I want everybody’s vision to really be.
Melissa Joy (59:10):
Yes. And let’s talk more about that role of the dietitian because I feel like we didn’t touch on that, and I know that was a big emphasis you really wanted to touch on in this conversation. And that role has changed. We don’t have to help people deal with cravings or willpower and portion control. Now, we have a different role. You want to talk about that?
Ana Reisdorf (59:32):
Right, yeah. So, a lot of prescribers or doctors, they give the person a prescription and they go, or they go to these telehealth and it’s a chat that they can talk to, but it’s not somebody really helping them. And people have a lot of questions. And the dietitian is the person to help these people not develop scurvy. The dietitian is the person to help them figure out how to exercise with their limitations, or eat correctly, or get off if they want to get off the medication.
Like dietitian, I think a lot of dietitians were hesitant at first or felt betrayed by this, or that it was going to take their work away. I think that the dietitian is the most important person, and I really wish that more would really start speaking out online about this because there’s people talking, and they don’t know what they’re saying, and the dietitians need to talk about this and talk to people about being more reasonable. Remembering your body needs food, remembering all of these lifestyle habits now this medication makes it easy to finally do them.
Melissa Joy (01:00:41):
You can focus on that, get all that mental load out of the way. Be like, oh, what would be nourishing to eat? What would be enjoyable to eat? How can I get more nutrition in and spread it out throughout the day so that I’m not too full, and yeah, all of those things.
Ana Reisdorf (01:00:58):
So, I think that the dietitians … and I see a change in our profession. I see them coming just so you know.
Melissa Joy (01:01:06):
Definitely.
Ana Reisdorf (01:01:07):
They like to know everything first, and I think that they need to just jump it.
Melissa Joy (01:01:12):
Oh, and it would be nice if the doctors would refer to us, or if people just knew dietitians are not the food police, we’re more like coaches than referees, please work with us. We’re reasonable people, we can help you (chuckles).
So, you’ve got your website, your podcast, tell us all the places you are, Instagram.
Ana Reisdorf (01:01:33):
So, it’s all GLP-1 Hub, the website is GLP-1 Hub, and you can find the podcast there. It’s called GLP-1 Hub Podcast, YouTube channel, Instagram, everything under that. And I do two podcast episodes a week and two YouTube videos a week, and have the Instagram and the newsletter.
And so, I’m doing a lot of things because I feel very strongly about helping people be healthier on this medication, live the life that they want, and really carry their bags at 80.
Melissa Joy (01:02:05):
Yeah, absolutely: quality of life. And I think I forgot to mention at the beginning, we may be submitting this to CDR for one free continuing education credit and maybe 1.25 if it’s long enough. So, if you’re a dietitian and that is of interest to you, stay tuned for that. And there are other free CEUs on my website at soundbitesrd.com.
Not every episode is submitted for CEUs though, I can’t possibly do that. I’m a one woman show in addition to my fabulous editor, and a couple other support people.
Thank you everybody for listening. Ana, thank you so much for coming on and thank you for doing all this important work that you do. I have learned so much from you, and I hope that people follow you and continue to learn from you and recommend your platforms to their friends and family and clients, patients, everybody.
So, I mentioned a few related episodes. I’ll have those links in the show notes as well as well as all of Ana’s links. So, thanks again, Ana.
Ana Reisdorf (01:03:07):
Thank you.
Melissa Joy (01:03:08):
And for everybody listening, as always, enjoy your food with health in mind. Until next time.
[Music Playing]
Voiceover (01:03:14):
For more information, visit soundbitesrd.com. This podcast does not provide medical advice, it is for informational purposes only. Please see a registered dietitian for individualized advice.
Music by Dave Birk, produced by JAG in Detroit Podcasts. Copyright, Sound Bites, Inc. All rights reserved.
LISTEN, LEARN AND EARN
Listen to select Sound Bites Podcasts and earn free CEU credits approved by the Commission on Dietetic Registration (CDR) for registered dietitian nutritionists and dietetic technicians, registered. Get started!
Get Melissa’s Sound Science Toolkit here!
Partnerships:
Sound Bites is partnering with the Association of Diabetes Care and Education Specialists (formerly the American Association of Diabetes Educators)! Stay tuned for updates on the podcast, blog and newsletter!
Sound Bites is partnering with the International Food Information Council! Stay tuned for updates on the podcast, blog and newsletter!
Sign up for my monthly newsletter and episode eblasts so you never miss an update!
Listen on Stitcher (Android)
Install the Stitcher App
1. Search for “sound bites with melissa joy dobbins” 2. Choose Play Current Episode or Add to Playlist
Choose “Play Episode”
Subscribe & Review on iPhone
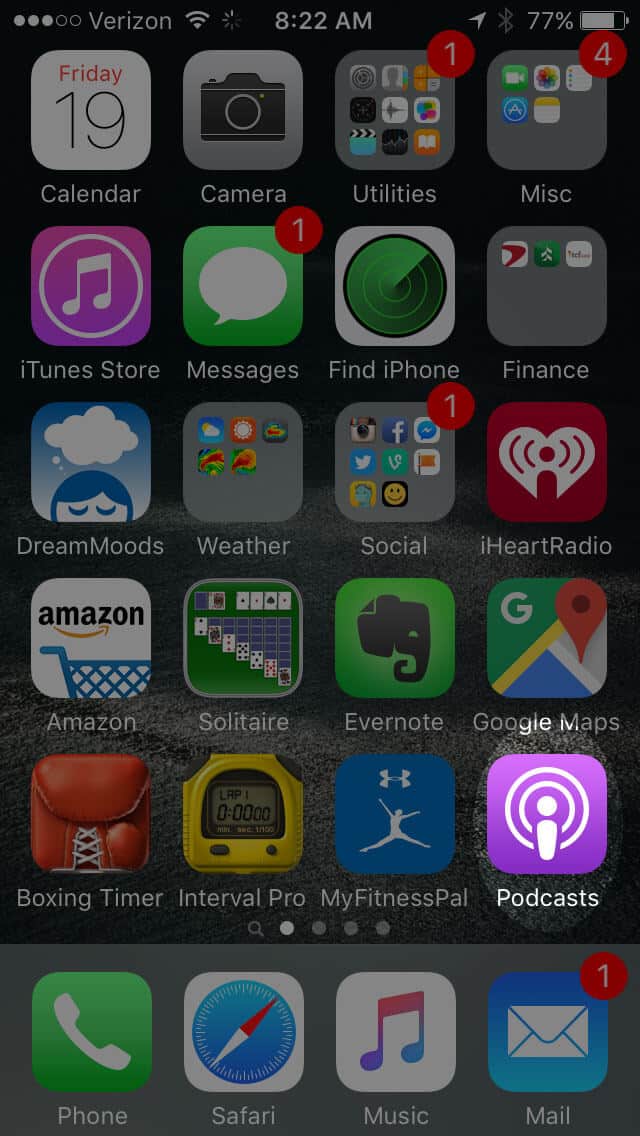
Open the “Podcast” app on your iPhone
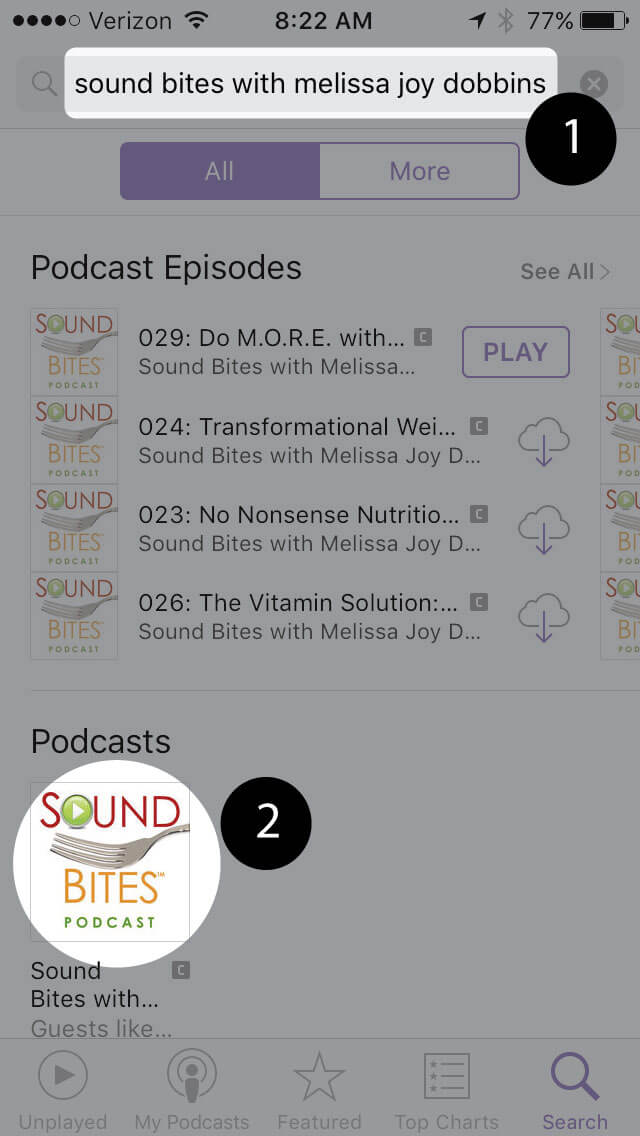
Search for “Sound bites with melissa joy dobbins”
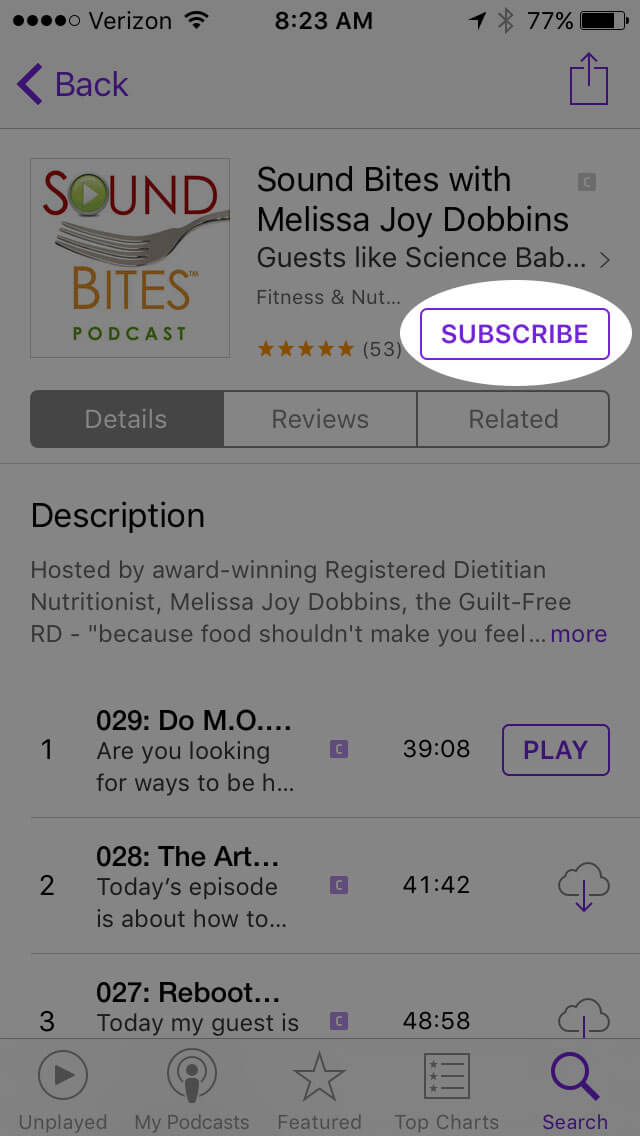
Open the podcast and click “Subscribe” and your done!
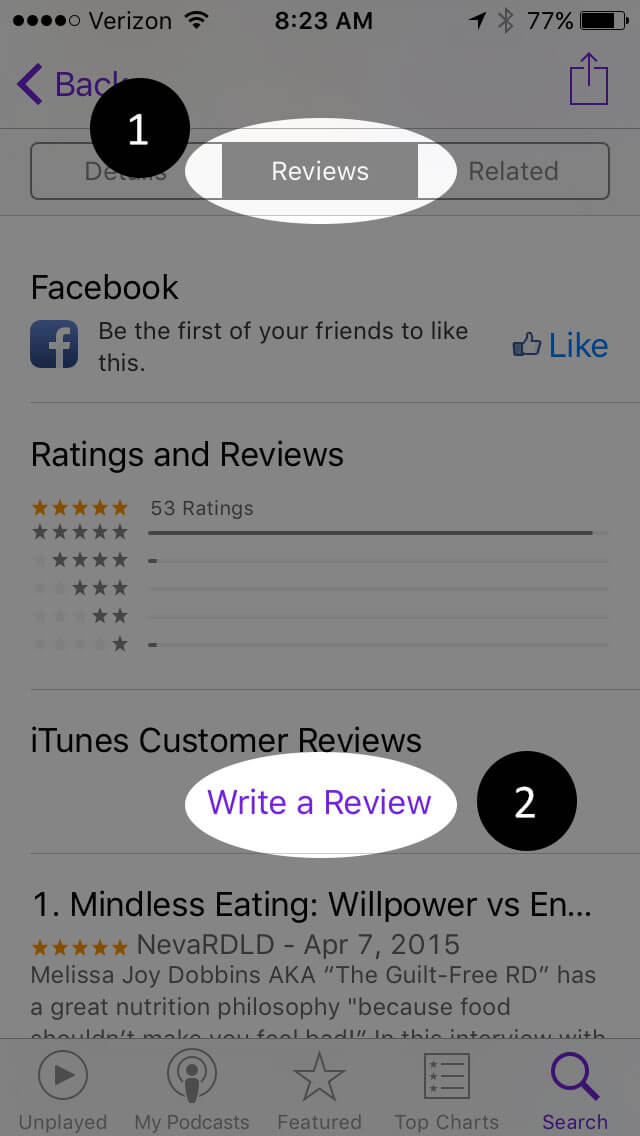
Write a Review
Click “Reviews”, then “Write a Review”.
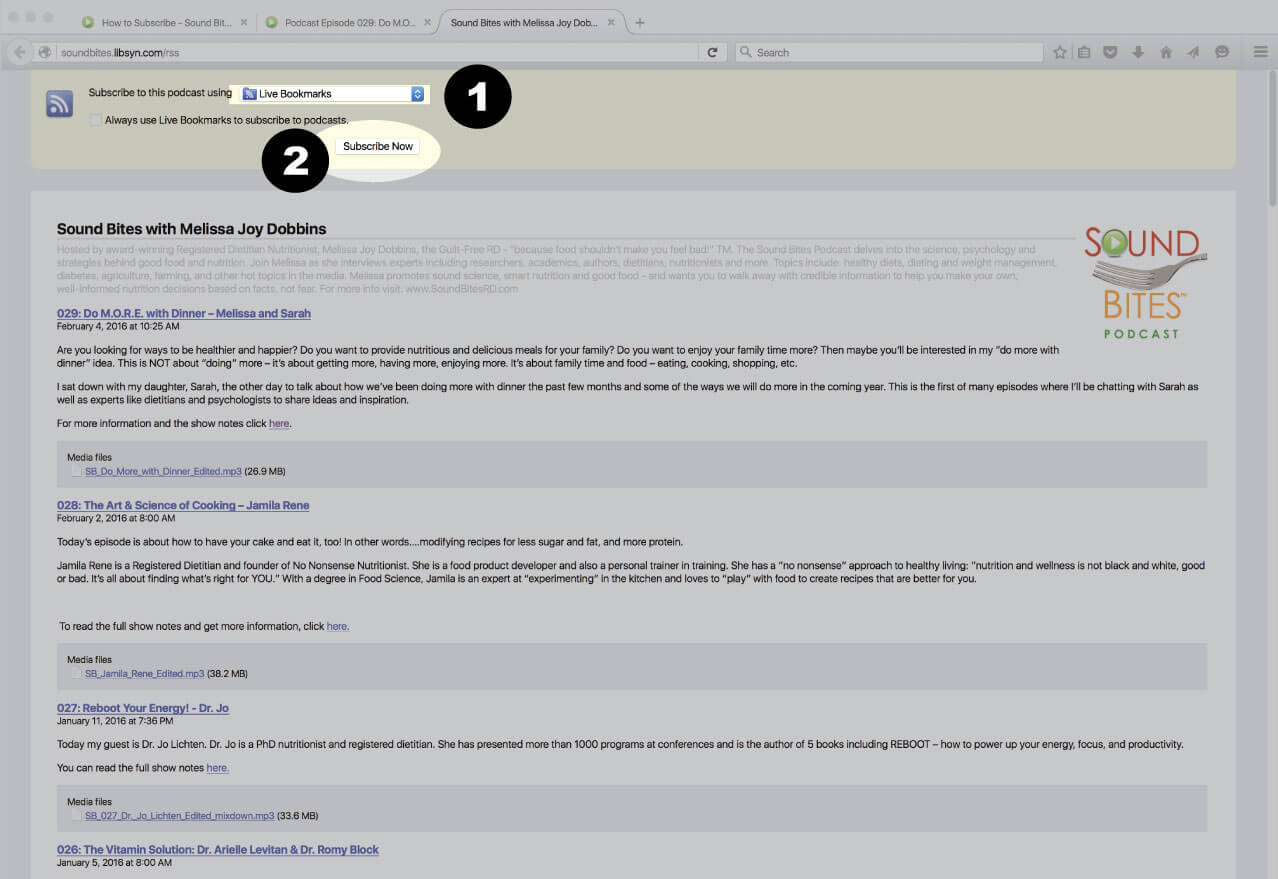
Subscribe via RSS Feed
Navigate to any podcast player . Click on the RSS feed icon.
Click on the RSS feed icon.
Click on RSS Feed
Choose which application you would like to use to receive the RSS feed
Click “Subscribe Now”
Confirm settings and subscribe.
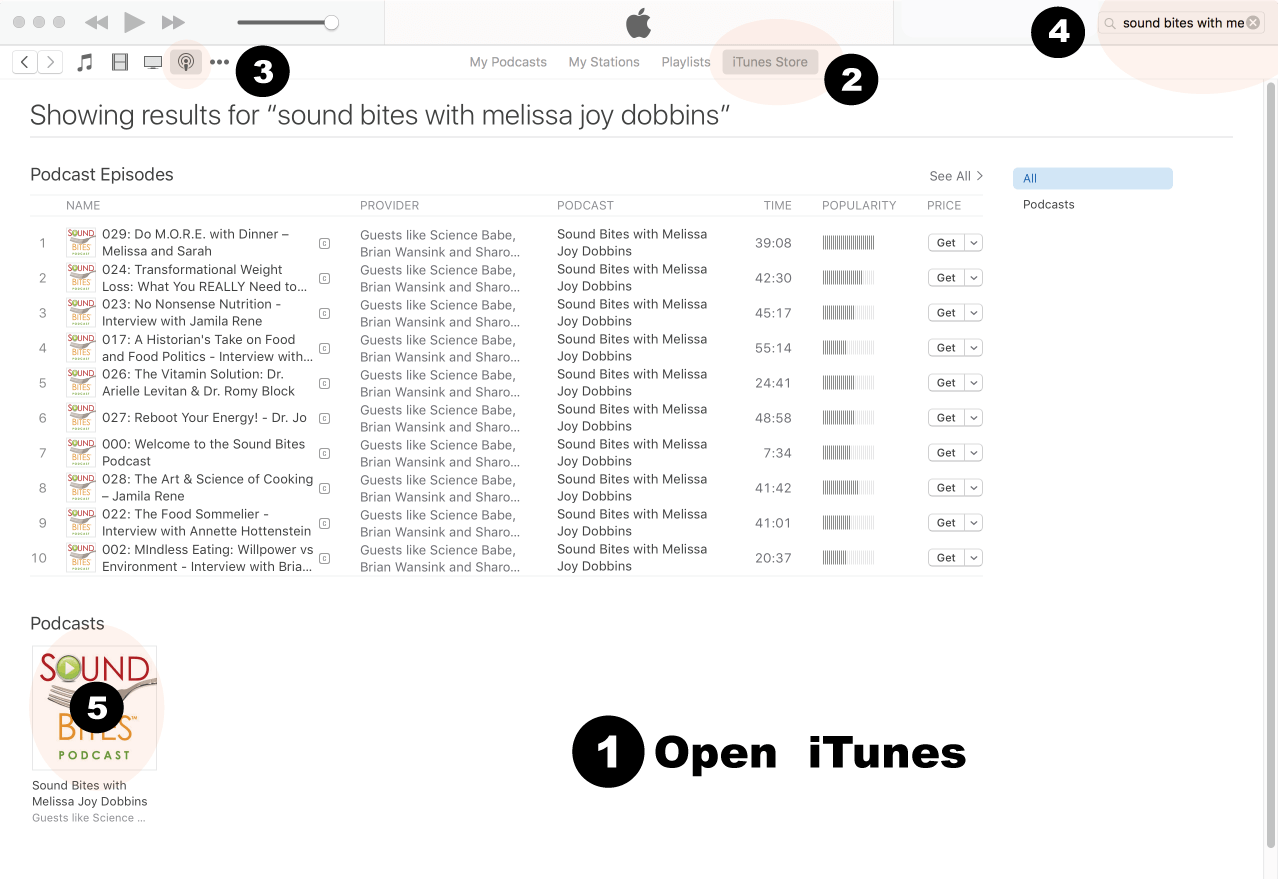
How to Review in iTunes
Open iTunes desktop application
Click iTunes Store
Click on Podcasts
Search for “Sound bites with Melissa Joy Dobbins”
Click on podcast image
Search for Sound Bites podcast in iTunes
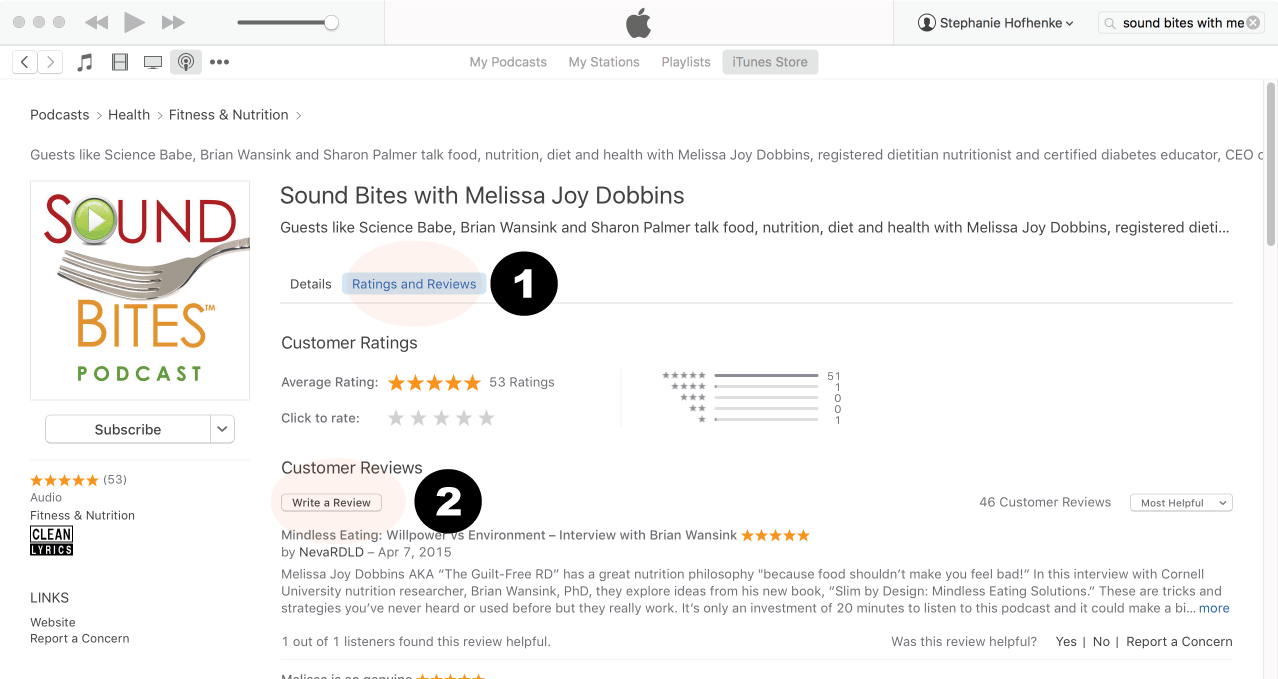
Click Ratings & Reivews
Click Write a Review
View reviews and write your own review.
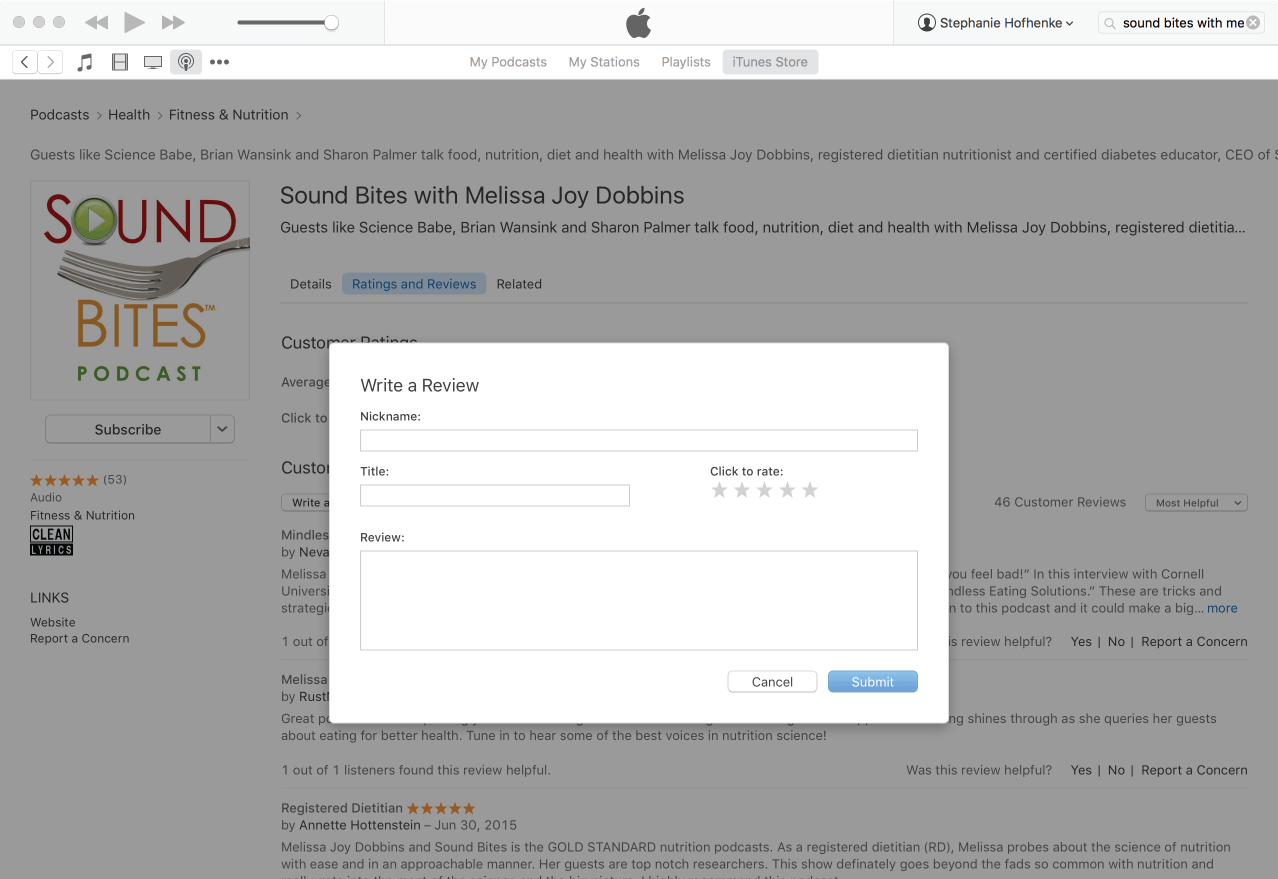
Write your review…. Thank you!
Write your review!
How to subscribe via iTunes
Click here to view the Sound Bites Podcastin iTunes, then click the blue “View in iTunes” button. This will open your iTunes application directly to Sound Bites Podcast. Click the “Subscribe” button, and your done!
 Ana Reisdorf is a registered dietitian, entrepreneur, and content strategist who has built her career at the intersection of nutrition, media, and online business. Before launching GLP-1 Hub, Ana ran a successful content agency staffed by a team of 10 dietitians, where she helped health and wellness brands create evidence-based, consumer-friendly content at scale. Through that work, she developed deep expertise in translating complex nutrition and health information into content that is both credible and engaging.
Ana Reisdorf is a registered dietitian, entrepreneur, and content strategist who has built her career at the intersection of nutrition, media, and online business. Before launching GLP-1 Hub, Ana ran a successful content agency staffed by a team of 10 dietitians, where she helped health and wellness brands create evidence-based, consumer-friendly content at scale. Through that work, she developed deep expertise in translating complex nutrition and health information into content that is both credible and engaging.