Celebrating over 1 Million Downloads and 50,000 Free CEUs on the Sound Bites® Podcast | NEW: Get 1 years’ worth of CEUs with the new 15-CEU Podcast Course
According to the CDC, among U.S. adults aged 18 years or older with diagnosed diabetes, 89.8% had overweight or obesity (2017-2020). Obesity is a disease that results from a mixture of behavioral, environmental and genetic factors, not just from lifestyle. We know that there is not one single treatment approach that works for every person with obesity, however there is one type of approach we can use when discussing weight with every person: trauma-informed care (TIC). TIC is an approach that recognizes the possibility that many people may have a history of trauma exposure, and how past or ongoing trauma such as abuse, neglect, food insecurity, discrimination or medical trauma can shape a person’s relationship with food, body and health behaviors. According to data from the Behavioral Risk Factor Surveillance System from 2011-2020, 64% of adults in the U.S. reported they had experienced at least one type of adverse childhood experience (ACE) before age 18 and nearly one in six (17.3%) adults reported they had experienced four or more types of ACEs. Compared to women with 0 ACEs, women with 4+ ACEs are 62% more likely to have obesity, 41% more likely to report a hypertension diagnosis, and 36% more likely to report a diabetes diagnosis.
ACEs may include: inadequate or risk to family income/economic hardship (poverty), living in a high-risk household (mental illness, risk of suicide, alcohol or substance abuse), parental loss or incarceration, physical, sexual or emotional abuse or neglect, witness to violence (domestic, community), and food insecurity.
Tune into this episode to learn about:
why TIC is so important
how TIC is different from motivational interviewing
benefits of TIC to patients and practitioners
the obesity-trauma connection
weight stigma and diabetes distress
adverse childhood experiences
shared decision making
resources for health professionals and the public
When patients are treated with a trauma informed care approach, they feel understood and heard, and are more likely to follow up. Trauma informed care is not a thing to do; it is a way of being and a way of starting with different assumptions about the patient sitting in front of you.” – Dr. Robyn Pashby
Robyn Pashby, PhD
Dr. Robyn Pashby is a licensed clinical health psychologist and a nationally recognized expert in the psychological and behavioral treatment of weight and weight-related chronic health conditions. As the founder of Health Psychology Partners, she leads a team specializing in the complex intersection of mental health, obesity, and chronic illness.
Weight bias is real and can result in long standing internalized trauma. Using trauma informed care when discussing weight in clinical practice can improve not only patient experiences but also health care provider experiences.” – Dr. Robyn Pashby
Resources
Some links may be affiliate links. As an Amazon Associate, I earn from qualifying purchases.
Welcome to Sound Bites, hosted by registered dietitian nutritionist, Melissa Joy Dobbins. Let’s delve into the science, the psychology and the strategies behind good food and nutrition.
Melissa Joy (00:23):
I’ve been getting a lot of questions from listeners about the continuing education credits that dietitians can get for some of my podcast episodes. So, I wanted to clarify that I do offer free CEUs for some episodes but not all the episodes. I have about three years’ worth of free continuing education credits, as well as some very low cost CEUs and a package on sale for one full year’s worth of CEUs.
If you want the convenience of taking just one quiz and getting one certificate for all 15 credits, this is a fun and easy way to get your credits, so be sure to check it out and you can get all the details on my website at soundbitesrd.com/freeceus.
Hello and welcome to the Sound Bites Podcast. Today’s episode is about trauma-informed care, specifically regarding weight bias and diabetes distress. This episode is not sponsored. My guest today is Dr. Robyn Pashby.
Dr. Pashby is a licensed clinical health psychologist and a nationally recognized expert in the psychological and behavioral treatment of weight and weight-related chronic health conditions. As the founder of Health Psychology Partners, she leads a team specializing in the complex intersection of mental health, obesity, and chronic illness.
Welcome to the show, Robyn.
Dr. Robyn Pashby (01:51):
Thank you so much for having me.
Melissa Joy (01:52):
I saw you present at the Diabetes DPG Virtual Symposium earlier this year, and I instantly thought you would be a great guest and this topic would be a great fit for my podcast. I learned so much, and I’m just so excited to talk with you and share this with my listeners.
Before we dive in, please share some more information about yourself, the work you do, maybe a little bit about your background so that people can get to know you a little bit.
Dr. Robyn Pashby (02:20):
Sure, sure. Well, thanks for having me and most importantly thank you for caring about this really important topic because it’s under spoken about and yet it affects so many people.
Melissa Joy (02:29):
Absolutely.
Dr. Robyn Pashby (02:30):
So, as you mentioned, I’m a clinical health psychologist, and basically what that means is I completed my PhD in a medical school and I did a dual program, a medical psychology program, and a clinical psychology program. And since that time for maybe almost the last 20 years, I’ve been working at the intersection of physical and mental health.
And that shows up a lot when we’re talking about issues related to weight to diabetes because there is such a psychological consequence to living with those struggles, but also causal factors from mental health conditions that can contribute to those conditions. And so, that bidirectional relationship is something that I’ve loved and explored for much of my career.
I’ve worked a lot with people living with different weight related concerns, many people living with diabetes, and I do a whole variety of different things in addition to my clinical practice.
So, probably most relevant to your audience is that I’m on the Clinical Practice Committee of the Obesity Society, I’m on the Weight Management and Obesity advisory board for the American Diabetes Association, and I’m also involved in various other things, including the board of directors for the Obesity Action Coalition among many other things.
So, I’m pretty all over the place in this field and in a good way, meaning my hands are in lots of different baskets, and I hope that we can cover some really important topics that in spite of so much expertise, is not often given the seat at the table that it deserves.
Melissa Joy (03:57):
Absolutely. And I know when we were discussing what do we want to cover in this conversation because there’s so much that we can get into and it’s a pretty heavy dense topic. You had shared that you have some sort of diabetes experience as far as from your education or your background, and I don’t recall what that is, so if you could share that, it’d be great.
Dr. Robyn Pashby (04:17):
Sure. So, the Diabetes Association as you know, offers a lot of really cool training programs and one of the things that they do is a lot of training in mental health care for people living with diabetes. And so, I’ve taken those advanced courses and will actually be moving into a train the trainer model for the ADA where I’m going to be teaching other community health workers about how to work with your communities and work with their communities on helping people deal with diabetes in a holistic way.
So, it’s something I’m really passionate about and see in my patients who I care so deeply about, but I see the heaviness, the weight of this work, and I know how important it is.
Melissa Joy (04:57):
Yes, absolutely. So, thank you so much for the important work you’re doing. Let’s start off with defining what is trauma-informed care and why is it so important? That might be obvious but I’m sure you can articulate more than just it’s important.
Dr. Robyn Pashby (05:14):
Yes. So, look, there’s lots of definitions of trauma-informed care, and I could give you the very specific ones and we’ll probably get to some of those specifics. But I always like to remind people that it’s just a mindset shift and that mindset shift moves from what’s wrong with the person in front of you to what’s happened to the person in front of you.
So, if you’re a healthcare professional of any kind, it’s so easy when we’re in a time pressured environment or working with a hundred people on their calendar in a week, it’s so easy to just sort of move into checkbox like, What’s wrong with this person? What’s wrong with that person? What do I need to fix?
And a trauma-informed care approach asks people to sit in different seat in their minds and really think, “Okay, what is this person’s experience and why is this person presenting to me the way they’re presenting to me?”
And I think when you make that shift, whether you’re a patient or a healthcare provider, I mean, I work with patients every day and I ask them to do the same thing about their own experiences because boy, we can sit here and say all of the healthcare providers need to work on their mindset shift but the truth is as people accessing healthcare, we also need to work on our own mindsets.
Because so often we get into self-blame, “What’s wrong with me? Why can’t I do this? Why can’t I be better, do better, act better, fill in the blank, take care of myself better.” And if we can shift that to, “What’s happened to me? What’s happened in my life?” Then we approach it with such a different level of compassion and understanding, not enough fluffy, say three good things to yourself way, but in a real way that you connect to the real issues.
So, trauma-informed care is really that mindset shift and I think it’s really important because there’s some good data out there that suggests that standard care that’s not a trauma-informed approach could be named like trauma blind and I think when you call standard care trauma blind, it gets people’s attention.
Because of course, no healthcare provider wants to be thought of as trauma blind. But if we don’t take a trauma-informed care approach as a universal precaution, then we are essentially operating in a trauma blind mechanism or way of being.
Melissa Joy (07:37):
So much, yeah, there’s the healthcare professional who wants to fix things, we want to help people and it comes from a good place, but it doesn’t work, it’s not helpful and we’re going to kind of get into some of the nuances and the psychology behind all of that. But we know that blame and shame are huge barriers to helping people grow and improve their health and have a better quality of life and that’s what we’re talking about.
Dr. Robyn Pashby (08:07):
Exactly. And I mean, if you look at the statistics, the reason trauma-informed care is so important is because the prevalence of experience of trauma. The National Center for PTSD said six out of every 10 men and five out of every 10 women have experienced trauma, at least one trauma in their lifetime.
And I think if you have lived through some of the things that we have lived through in our generation, even most recently, the pandemic, I think it becomes sort of even more universal. So, if you think about all of the various ways that people have experienced traumatic stressors in their lives, we can’t ignore it.
Melissa Joy (08:44):
No, I’m glad you brought that up because for everybody listening, it’s like, “Why is this important to me, either as a person or a healthcare professional, how much more prevalent it is than we might think.”
So, I know in your presentation you kind of shared some examples of trauma. If you could share some of that, I think it might help us go, “Oh yeah, this is like almost everybody,” even more maybe than those statistics that you shared.
Dr. Robyn Pashby (09:10):
I think that’s a really important point because a lot of times when I’m talking about trauma with people, what they immediately go to are very serious and impactful things and I don’t mean to minimize those.
But people who have experienced combat, maybe people that have been in serious accidents or been attacked or various other … maybe experienced childhood abuse or have left so very serious situations. But I think that that is an underestimation of what I would call cumulative traumatic stress during the course of our lives and many different experiences of trauma.
So, let me give an example, sort of a modified example from one of my patients over many, many years ago. But this is a person that lived with obesity, so lived in a larger body and — gosh, I have so many of these, but I’ll pick this one. And she went to the gym in our neighborhood where my office was and was feeling so proud of herself.
She worked out with a trainer twice a week, she was as healthy as she had ever been feeling so strong and physical strength sort of lends itself to feeling emotionally strong and she was just feeling great and she hadn’t lost a lot of weight, but that was not our goal. Our goal was for her to improve her quality of life, to feel mentally better, to manage her blood sugar a little better, which she was doing.
She left the gym that day and was crossing the street at the light (and I live in a city, so crosswalk) and as a car drove by her, as she was crossing the street, they threw a bag of fast food trash, just a crumpled up paper bag out the window at her and yelled something like, “Why don’t you go in that gym behind you — and some very derogatory term.
And the client came into me at our next session visibly shaken by this experience, not only because it was abusive and horrible, but because it felt so violating to the experience, her emotional experience that she had just been in, it just pierced this sense of pride and accomplishment that she was enjoying after a long time of struggling with a variety of health conditions.
And of course, that person in the car didn’t know any of her history, didn’t care to know any of her history, made so many assumptions. But if I had not been working with that client, I don’t think she would’ve ever told a single person that story. Why? Because it’s humiliating.
And so, I think about that story, and maybe some of the listeners here, healthcare professionals or not, have experienced teasing or bullying or feeling excluded or being excluded, being unable to access promotion at a job because of something that feels outside of your control, how you look or your ADHD or whatever it is.
It doesn’t have to be weight related but it’s this idea of being singled out as you’re bad, you’re wrong, something’s wrong with you, it goes right back into where we started, which is the goal of trauma-informed care is to get out of what’s wrong with you and get into what’s happened to you.
So, that’s one example. I mean, we could do a whole episode just on me giving you examples of that. Those are examples to me of cumulative traumatic stress. There was no question in my mind that on top of everything else in her life was a cumulative trauma. So, I mean, that’s just like I said, one example.
Melissa Joy (12:46):
Yes. That’s a powerful story and it happens so often.
Dr. Robyn Pashby (12:51):
Maybe not as egregiously, but anyone who’s been in the supermarket, who’s lived with obesity or diabetes for that matter, maybe has a CGM on their arm or something and is in the supermarket and getting food and has had someone sort of look up and down at their cart.
Melissa Joy (13:07):
“Should you be eating that? Should that be in your cart?”
Dr. Robyn Pashby (13:09):
Exactly.
Melissa Joy (13:11):
Even if it’s just a look.
Dr. Robyn Pashby (13:12):
Right. And so, I like to use that example because it doesn’t have to be as egregious as the one I just shared to pierce.
Melissa Joy (13:20):
And take the wind out of her sails and she was on such a good trajectory and yeah and that’s part of the issue is these things are barriers to that person improving their health and quality of life and their mental health is a big part of that.
Dr. Robyn Pashby (13:35):
Yes.
Melissa Joy (13:36):
So, I’ve done some previous episodes on obesity as a disease and weight bias, weight stigma, even amongst healthcare professionals, bias in healthcare and I know you talk about these topics a lot. What else do we need to know about those to kind of talk about maybe the obesity and trauma obesity connection?
Dr. Robyn Pashby (13:57):
So, I just gave you some statistics about the numbers of people that we estimate have experienced a traumatic event in their lives, at least in the U.S. and numbers are higher in other parts of the world. But I think that if you look at the statistics of people living with more severe levels of obesity, the more severe disease state, what we see are exceedingly high numbers of people who have had what we call adverse childhood experiences.
And that can be exposure to child abuse or neglect, but also parental substance use or parental incarceration, parental suicide, or very serious mental health issues, the list goes on and on. But adverse childhood experiences are very common, people living with obesity in adulthood.
Melissa Joy (14:44):
And those even include poverty and food insecurity.
Dr. Robyn Pashby (14:47):
Oh, absolutely. Absolutely, include that. Even community violence, living in a community that is unsafe and experiencing various types of violence. I talk about that because I want people to think about it, but I’m also careful to not want to bias people more. So, you look at someone living with obesity and think, “Oh, okay, that person experienced trauma or abuse or something, because that’s not fair either.”
Because statistics don’t make the person and I also think that it doesn’t need to be an adverse childhood experience scaled checkbox to accumulate over time as chronic traumatic stress. So, there’s a very deep connection between trauma and obesity, but it’s not always what it seems like at first read and it’s very bidirectional.
So, adverse childhood experiences we know become predictive of obesity in adulthood. What I think I want to get across to people is that living with obesity, particularly in childhood becomes predictive of experiencing traumatic stress. Why? Because of bullying, teasing, bias, all of those things that are without a doubt traumatic.
Melissa Joy (16:00):
Absolutely. And just to put a finer point on it, you’re saying that people with more adverse childhood experiences, they’re more likely to have obesity and even high blood pressure.
Dr. Robyn Pashby (16:10):
As well as diabetes.
Melissa Joy (16:12):
So, as a diabetes care and education specialist myself, I know about the diabetes distress scale and diabetes distress in general. So, let’s talk about that a little bit because it’s kind of similar to what we’ve been addressing with obesity, and you’ve mentioned diabetes a couple of times. So, what is diabetes distress and how does it impact quality of life?
Dr. Robyn Pashby (16:34):
Look, diabetes distress, anybody that lives with diabetes knows what that means just inherently. It’s the stress related to the relentlessness of diabetes, the relentlessness of the self-management and the realization that there are even in the best conditions where the best monitoring and the best care there can be serious long-term complications.
And I think that feeling of helplessness and hopelessness is very serious for people and can lead to something bigger than diabetes distress to burnout and depression and other pretty significant mental health concerns.
But diabetes distress also, of course, is related to even just like dealing with other people’s unhelpful reactions. Oh, should you be eating that or what’s your blood sugar after you ate that piece of birthday cake with your six-year-old son? All these kinds of things.
It’s just exhausting and it is emotionally taxing and then let’s not even get into what it’s like to navigate insurance and financial things and dealing with, “Oh, my CGM broke and now the insurance company won’t let me get another,” whatever it is. I mean, it’s just like this sort of chipping away at people’s lives.
I just recently heard this new term called time toxicity and financial toxicity and it’s this idea that the burden of carrying major chronic medical conditions like diabetes becomes toxic to our time. It soaks up every spare minute. Financial toxicity for obvious reasons, it soaks up any spare penny you have and I think of course, if you’re living with those things going on in your life, you experience distress and they can lead to burnout.
Melissa Joy (18:17):
Yeah, absolutely. Just overwhelming just thinking about it.
Dr. Robyn Pashby (18:20):
Yes.
Melissa Joy (18:21):
You have a slide that talks about kind of where and how stigma comes into this equation, whether it’s personal or social or clinical. So, I’d like to talk about that a little bit more just to kind of connect some of those dots because this concept on the surface makes a lot of sense, but when we get into the specifics, there’s a lot of ahas going on.
Even for people who maybe are, I think we’re going to touch on how is this different from motivational interviewing, just again, healthcare providers, dietitians who … we’re there to help people and we’re coming at it from a good place, but then the more we learn it’s like, “Oh yeah, these shifts are really crucial.”
Dr. Robyn Pashby (19:05):
So, I think it is an impossible goal to assume that healthcare professionals or even patients ourselves will be free of bias. Instead, I think our job is to examine our biases, recognize when they come into play and work at shifting.
I never want to set people up to think, “Oh, I can’t undo that bias so I’m bad and therefore I’ll stop doing this or I just won’t even try, who cares or I’m bias free.” Actually, the people that pretend to be bias free are the people that worry me the most because it’s a little less examined.
And so, I think that the stigma piece is inherent in our nature as human beings because we are social creatures and so we’re constantly comparing sort of our social status. I don’t mean financial, are we acceptable as humans to everyone that’s around us? And that is still true if you’re a healthcare professional.
And I think when you add in something like obesity that has been so misunderstood for so long, or diabetes that is subject to the same misconceptions that obesity has been, which is essentially it is a matter of willpower and if you just behave better, you will do better, you will be healthier that of course, these stigmas come out in full force.
I mean, the stories I have heard from my patients and experienced myself by the way from healthcare providers, meaning, well, I know my friend Joe, who’s an amazing something, did the Atkins diet and lost 40 pounds, I think you should give it a try. It’s not because that person is trying to shame me, it’s because they’re actually trying to help me. It’s so lacking in an awareness, it’s a trauma blind approach.
So, if you were to think to yourself, what’s wrong with this person and what you see in front of you is a person that you deem eats too many carbohydrates and could benefit from weight loss then throwing the Atkins diet idea, and I don’t mean to pick on Atkins, you know-
Melissa Joy (21:14):
Fill in the blank.
Dr. Robyn Pashby (21:14):
Yes, fill in the blank diet. Some, very strict and specified plan that is universally applied. You throw that plan at this person and think, this will fix the problem.
If you think what has happened to this person in front of me during the course of their lives and think for even a minute, wait, okay, this is a person that has lived with weight and diabetes struggles for 25 years or more, and has tried every plan on the market, has been on three different medications for diabetes, has experienced serious health consequences from it, is totally ashamed about all the things they have to do to just survive the day and I’m going to suggest something that’s just like sort of a universal fit, that doesn’t even make any sense anymore.
But it makes sense to someone that approaches it from that, “What’s wrong with this person in front of me?” So, if that tiny example gives you an idea of, as a healthcare professional, why if you just switch that mindset, you actually help people so much more. It is so much healthier of an interaction.
And by the way, I didn’t say this earlier but there are some newer or maybe up and coming data that when healthcare providers use a trauma-informed approach, they report lower levels of physician related burnout.
Why? Because they’re actually helping people and that’s why they went into that job. So, imagine this scenario where we can help patients and we can help physicians or other healthcare providers for that matter, what a win-win.
Melissa Joy (22:56):
Yes, I’m just sitting here kind of, I don’t want to say smirking, but I have to share this. Even myself as a dietitian, one of the last times I went in for my physical, my doctor who I love, we were talking about my weight and menopause and she said, “Well, I just cut X, Y, Z out of my diet and I lost eight pounds.” And I was sitting there going, “Seriously?”
And then she’s like, “Well, have you met with a dietitian (laughs)?” And I’m like, “Actually I have. I hired a dietitian (laughs) and I wasn’t just treating myself.” Anyway, just a total side comment because it’s everywhere.
Dr. Robyn Pashby (23:30):
It’s everywhere. And you saying couple things, I love this doctor, obviously you have a relationship with her, she knows what you do and it’s just blurted out not because she’s trying to hurt you, she’s trying to help you.
Melissa Joy (23:43):
Yeah. For sure. And also, something else that came to mind when you were talking as a diabetes educator, we see such a huge difference in the mindset of people with type one versus type two. They’re both overwhelming diseases and there’s so many moving parts and so much going on.
But the type two people tend to deal with much more shame and blame weight aside. I mean, weight is a part of that but let’s take that piece out of it.
I was kind of surprised, but then it made sense when I started getting more involved in social media, I don’t know, 10, 15, it’s not 20 years ago, but like 15 years ago, realizing that the diabetes online community, which I don’t even know if we talk about the DOC anymore, but it was primarily type one people who were reaching out and they’re getting that online support and they’re sharing their stories and supporting each other, but the type two-ers like lurking because of all that stigma.
And he’s like blame and shame that they did something wrong and that’s why they have diabetes. So, that was just something that popped up in my mind when you were talking, because it’s such a glaring difference.
Dr. Robyn Pashby (25:05):
Yes. And the cause of that like you just identified, is that people feel responsible for their own condition and therefore feel responsible for their own treatment.
Melissa Joy (25:16):
Yes. And so many times like this is, if we think about these things logically, we know, okay, well maybe some people do say, “Oh, well I did this and that and that’s why I have diabetes,” still, it’s so emotional. Again, just sort of a personal, I think I shared this in a previous episode. I don’t normally share a lot of personal things, but-
Dr. Robyn Pashby (25:35):
I’m a psychologist.
Melissa Joy (25:36):
You’re pulling this out of me; I feel safe with you. It was a blood pressure episode that was just a fascinating guest. And I said, I went on a hormone replacement patch and my doctor said, “Check your blood pressure within two weeks,” and I always had beautiful blood pressure. And I’m thinking, “Okay, yeah, whatever.”
I checked it and it was high. And so, I went through this, “Oh my God,” and (laughs), I don’t know if I shared this before, but a family member who is a physician was telling me, “You need to lose weight. You need to cut all the salt out of your diet. You need to stop drinking wine.” And I was like, “You need to leave my house right now (laughs). Now my blood pressure’s really high, thank you very much.”
But I did go through that like, “I’ve brought this on myself, what did I do?” And then I was like, “Wait a minute, my blood pressure was fine before I started on this patch. Let’s go off the patch and see what happens.” And sure enough, my blood pressure went back to being beautiful.
Even if we do know logically that we didn’t cause this or if we’re like, “Yeah, my lifestyle may have been a contributing factor, I can make some changes,” there’s just such an emotional component to it that kind of overrides our logic brain.
Dr. Robyn Pashby (26:47):
Yes, you just highlighted that our brains need to have cause and effect and the truth is diabetes and obesity are very complex conditions that do not have a single cause, they often get reduced to single measurements but they are not singularly caused.
Our brains really struggle with that ambiguity. So, it’s much easier to say, like for you, “Oh, the patch is the problem,” take the patch off, problem solved. With diabetes, “Oh, the blood sugar is the problem, stop doing X that causes my blood sugar to spike and fixed,” but of course we know it’s just not like that.
Melissa Joy (27:30):
Yes. And I oftentimes tell my patients, I work with a lot of people who are sort of in the pre-diabetes realm, and I have some colleagues who, they’re like, “Well, that person’s doing everything right, why do they have pre-diabetes?” And I’m like, “Because their body isn’t processing things as efficiently as somebody who is not at risk.”
And so, I try to kind of separate some of that for people. You’re doing such great work here. Your body is just struggling a little bit and somebody else could be exercising way less than you, eating way more than you and their blood sugar is fine because their body is different.
Dr. Robyn Pashby (28:12):
And of course, as a psychologist, I’ve been so aware of this sort of stigma in mental health forever also. Depression or anxiety, people feel to blame for their own mental health conditions as well so the overlap is so similar.
And I was saying to you just before we jumped on record, that with this idea of diabetes distress and diabetes burnout, I’ve thought for a long time that there’s obesity burnout and obesity distress because of the chronic nature of needing to manage it. And the same is true with people’s mental health, people get burned out on just managing their mental health too, because it’s hard.
Melissa Joy (28:49):
Yeah. It’s like you don’t get a vacation from that.
Dr. Robyn Pashby (28:52):
Exactly. Yeah.
Melissa Joy (28:53):
Unless you’re burnt out and then you take a vacation from there-
Dr. Robyn Pashby (28:55):
You take a vacation.
Melissa Joy (28:57):
And then that has consequences. So, in all of this we’re talking about is trying to remove these barriers or like you said, make this shift to help open up the conversation and that’s where you have a lot of great advice that I want to dig into. I don’t know if now’s a good time to start teasing out the difference.
Well, wouldn’t this just be motivational interviewing? Wouldn’t it just be asking open-ended questions being that partner or that coach instead of I’m the person who has all the power and knowledge and I’m imparting it onto you. Talk to me about some of those nuances.
Dr. Robyn Pashby (29:36):
As someone who uses motivational interviewing in my practice and is a firm believer, I can tell you that the name motivational interviewing gives me the heebie-jeebies.
Melissa Joy (29:46):
Yeah. I don’t like it either (laughs).
Dr. Robyn Pashby (29:48):
Okay. Because to me it is a biased from the get-go approach because what we’re doing when we sit in that seat as someone who does it but is assuming that motivation is the problem and if I just get this person more motivated, then they will behave better and then do things. So, it’s just to me, one step up level from this whole idea that you just need to behave better then you’ll be fine.
So, while the idea of asking open-ended questions is of course a great way of interacting with folks, I want people to be thoughtful about how they think about motivational interviewing and not get caught up in, “I need to raise this person’s level of motivation.” What we actually want to do is know this person, that’s the difference.
And so, trauma-informed care asks you to know the person, to understand your assumptions that this person has something wrong, I need to help fix, it may not be the assumption that is going to be the most helpful.
So, instead, changing your assumptions like, this person’s been around the block with this, this person’s been through the wringer and this person is exhausted, if you start with that assumption, guess what, there are a few people that will surprise you and say, “Oh, this is new to me. And I had never thought that reducing my carbohydrate load would help my blood sugar.”
There will be a few people like that but the majority of people will feel seen and will trust you in a way that allows them to think about what is real in their lives and applicable in their lives. Because the truth is, we don’t have all the answers, we don’t know what is going to work for what person.
So, it’s a changing your baseline assumption rather than saying, “I’m not going to have any assumptions of this patient, or I’m not going to have any biases of this patient.” Of course, you are. You’re a human being and you’re there to help so you’re going to have all kinds of biases and all kinds of assumptions. It’s about understanding maybe those are not the most helpful ones in front of me and maybe I need to find out.
So, in medical terms, there’s a lot of discussion of shared decision making and I think that’s another way of saying, asking open-ended questions, working together as a team and again, shared decision making to my mind, that’s an obvious one. But instead, we should be thinking about changing our baseline assumptions of the person in front of us.
And the other thing that’s really interesting is, I think the difference in a motivational interviewing versus a trauma-informed care approach is that someone who’s actively using a trauma-informed care approach spends a little bit of time thinking about their own trauma and how and what that does to the interaction with the person in front of you.
Because you just said you’re on the patch, you gained a little weight during that, your patients, you’re your clients, we all share similarities with some people in front of us. So, what you had experienced in your life is going to be relevant in the room with your person that you’re working with.
And I don’t mean you need to go into deep trauma therapy, but I do mean you need to sort of understand that this could have a role in how you react to the person. The reason your doctor said, “Hey, this worked for me,” is because she felt so relieved to see her weight change, she was wanting to give you that relief.
That’s something that had she thought about it for another second, she might have skipped, might have skipped saying to you. So, I think that shared decision making is great. It’s another way of talking about it, changing your baseline assumptions, being aware of your own trauma history and how that shows up in the room.
And instead of downplaying or disregarding people’s hurt, no matter how small or unrelated it may seem to you, just sitting with it for a second can help people feel seen. So, the woman that I talked about earlier with the horrible experience after leaving the gym, if she were talking to her physician about it, who had three minutes with her or something, she might’ve said, “Yeah, some jerk made fun of my weight,” that’s what she would’ve said.
And a doctor could’ve easily been like, “Whatever, don’t believe those people, move on.” And that is so downplaying what this person’s actual experience is, not blaming the physician in that they don’t have time to sit like I do, it’s a luxury of my job but what if the physician responded with, “Ugh, I bet that hurt.”
Melissa Joy (34:29):
That doesn’t take any more time.
Dr. Robyn Pashby (34:30):
And yet it helped the person feel seen instead of, “Oh, you no worries, who cares what that person thought?” And so, I think to me, those are big differences in a trauma-informed care approach versus a motivational interviewing which is kind of like I’m leading you to this water hole hoping that you’ll drink.
Melissa Joy (34:51):
The word that comes to mind when you’re talking is compassion. So, it’s sort of a compassionate way of communicating and just connecting that also comes to mind.
Dr. Robyn Pashby (35:02):
I think it’s connecting. And I will say that is an exhausting process, but it becomes so much more rewarding in the long run and also expands trajectory of that person’s treatment experience so much.
It enables them to trust you when you start making referrals to support people, to a trainer or to a psychologist or to an endo, a new endocrinologist or something like that. They begin to trust you because they recognize that you’ve actually seen them.
I mean, one of the things I’ve spent years doing in my practice is just developing a long list of who I consider trauma-informed care providers in every discipline. I mean, I’ve got podiatrists and hairstylists, you name it, everything that I’ve just learned from my patients.
They will tell me a story like, boy, I was talking to my podiatrist and because I have diabetes, she was helping me manage some of my foot issues and she listened or a dermatologist who didn’t make me feel ashamed when she had to lift up skinfolds to check for this mole that I had versus someone else who touches you with a stick from far away.
These are real things. So, I think if you act as a trauma-informed practitioner, it also makes your support network in treating this patient easier as the patient then trusts you to refer them out.
Melissa Joy (36:27):
And real progress can be made, meaningful.
Dr. Robyn Pashby (36:30):
Absolutely.
Melissa Joy (36:31):
So, the shift in mindset is key, but you also said this can be exhausting. How do we, well as healthcare professionals, practitioners, and then also maybe in thinking about ourselves as patients, on the other side of that relationship and those are two different things. How do we start practicing these skills and improving these skills? Where do we begin? And it’s just like one step at a time and just keep trying to improve those skills.
Dr. Robyn Pashby (37:08):
I mean, I think there are trainings that people can do on trauma-informed care, so it’s not just a, “Oh, you should listen to this podcast and now know how to do it.”
And what I hope happens is that healthcare professionals listen to something like this and think, “You know what, the next continuing medical education I need or the next continuing education or a various other thing I need, I’m going to go look for that. I’m going to go see if I can find a training in trauma-informed care and really learn the ins and outs and start to implement it.”
Or maybe they read a book about it or maybe they talk with other colleagues and professionals in their field and get support around like, “Guys, I’ve really been thinking about this and I want to use some of these skills because I get it. I get that people need it.” That’s sort of on the patient side.
Related to that, just quick thing, I was reading some studies recently and there was a survey of physicians, about 200 of them who said that they were informed in trauma, like trauma-informed care, at least partially yet only 16% of them during this survey estimated that 50% of their patients had experienced trauma.
Statistically, we know for sure that 50% of their patients had experienced trauma just because that’s the numbers and only 16% of them acknowledged that. So, I think that part of it is just it’s hard for us as healthcare professionals to sit with the idea that this many of our people are hurting. It’s a heavy load. So, that’s why we need a lot of support from our networks and our people that we travel the world with for conferences and other things, we need those people.
And that’s why a lot of the people that we end up working with are not just patients, but we work with a lot of healthcare providers to not give them skills and trauma-informed care, but to help them manage their own burnout and their own trauma. Because once you start to see how much pain is out there and the people we’re working with, it’s hard but I think it’s there no matter what.
So, it’s not like, “Oh, well I won’t go get that MRI because I don’t want to know what that lump is.” The lump is there no matter what and the same is true with trauma. It’s there no matter what, whether we choose to see it or not, whether we choose to address it or not, both in ourselves and in the patients that we work with.
Melissa Joy (39:25):
I mean, when I was early in my career, I did a lot of eating disorders and weight management work and I got so burnt out on it and I remember just feeling like I need a degree in psychology to really help these people. And now it’s kind of come full circle that you can be a dietitian and work in different areas but learn more about these types of approaches that you don’t need a degree in psychology, you just can learn more about how to do this.
Dr. Robyn Pashby (39:50):
You really can because it’s not trauma treatment, it’s trauma informed care. Trauma treatment, leave that to us. But trauma informed care is very different and like I said earlier, it actually results in lower levels of burnout, healthcare professional burnout.
Once you start feeling competent in handling the pain that’s in your office, not treating it, but just seeing it and understanding it and then getting people where they need to go, great, you feel better. You’re helping people, it feels good to do that.
So, yeah, I mean, I think you said the mindset shift. I think, if I would ask anyone listening to do one thing, it would be to really do an honest assessment of, “What is my mindset when I sit down with a new patient living with obesity and diabetes, what am I really thinking? What am I thinking if they come in dressed in a suit versus they come in in sweatpants? What am I thinking if their hair’s fixed or not fixed?”
These are all real things that affect our perceptions. We don’t have to be ashamed to have perceptions, we have to recognize them. And so, once you start to do that, then I firmly believe that healthcare professionals want to be helpful.
And anyone listening to this cares enough to have listened to this whole thing, so they want to do this, but you can’t change what you don’t know so start there. Start with really looking at your assumptions honestly and not being ashamed if you have them.
Melissa Joy (41:21):
Right. Thank you. A couple things that come to mind, I do want you to share a few of the tangible things that you covered in your presentation. We don’t have time to get into all of those, that was a webinar and visuals and all of that.
But I do want to leave our listeners with some of those and we’ll put some resources in the show notes as well at soundbitesrd.com. But the other thing that has occurred to me as you’re talking is, well, what about those people who don’t have trauma, this still works with them, right?
Dr. Robyn Pashby (41:54):
So, it’s a universal precaution. The thing that I said, I think maybe in that webinar that you watched is think about it like handwashing. You don’t handwash only when you know you’ve contacted some infected surface and not all the surfaces that we touch are infected with bacteria, well they are, but you know what I mean. Something really scary-
Melissa Joy (42:13):
Let’s not go there.
Dr. Robyn Pashby (42:15):
But instead, what we do is we wash our hands as a universal percussion because it protects us and because it protects other people. And so, there’s plenty of people you’ll see in the practice that you’re in that don’t have trauma experience. Probably almost everyone has trauma exposure, but not everybody experiences it the same way and that’s fine but it’s still fine to talk to people in a trauma informed way.
To answer the first part of your question, which is some tangible things, especially around weight in particular, the first thing I think I said, and I just always say is ask consent period, full stop.
So, if your doctor had said to you, “Would you like me to give you some suggestions on how you can manage your weight?” You probably would’ve come back with something much more like, “Well, I’m a dietitian and I already have engaged with another dietitian colleague of mine and I have some ideas.” And she would’ve been much less likely to then flippantly throw out, “Oh, well I did this and this.”
Well, you start by asking consent to talk about this topic, which is deeply personal, weight and diabetes management are deeply personal even if they have come to you for that issue. The truth is, someone who made the appointment with you two weeks ago is not the same person who is sitting in your office or on your screen.
Because moods about weight change depending on what the scale said that day, depending on how your pants fit that day, depending on what you ate last night, depending on where you are on your menstrual cycle, depending on how your spouse talked to you or treated you, depending on whether some bully shouted something at you or someone looked in your grocery cart 30 minutes ago, so the person that reached out to you is not always the same.
So, they could say, “Yes, I want to talk to you about my weight.” And then they walk in your office feeling in a dark shame spiral and you might have to say, “You know what, let’s just get to know each other today. We’ll start talking about other stuff next time.” And that’s okay. And you have to actually respect it when people want to not do that, so you may not agree.
And then the next thing is really respecting patient autonomy. So, they have a right to have a say in how they want their care to go and whether that’s faster or slower than your preferences or using different treatment methods, you can give your professional opinion, but patient autonomy needs to be at the top of the list.
And then transparency. So, I think using transparent communication, if you’re a healthcare provider who’s going to touch someone before you give them an injection or before you do a thyroid exam or something like that. Even just saying, “I’m going to put my hand on your shoulders so that I can touch your neck and feel your thyroid, is that okay?”
Even if they’re there for a thyroid exam, using that sort of permission asking thing gives people a sense of, “I have a choice in this matter.” So, much less triggering for people. “So, is it okay if we talk about your blood sugar numbers today?” Even if they’re there for that, it still gives them the choice.
Those are just some very tangible things and then there’s so many others like having size, accommodating equipment if you’re seeing patients in person, certainly having food safe environments. So, not having your front desk team having ordered some smelly takeout food or something which you’d be surprised how many things happen.
Just being sensitive to all of those factors, having blood pressure cuffs that fit appropriately, having exam rooms that are size accommodating, these sorts of things, gowns, all of those types of things are very obvious and there’s plenty of places we’ll link to that you can learn more about those.
Melissa Joy (45:49):
Great, thank you. And one other thing that I thought of, I did an episode on disordered eating and that’s not the term that … the guest was Jessica Setnick, and she was talking about how she trains dietitians to improve their skills in working with people with eating disordered and disordered eating behaviors, I think this is what she calls it.
Because similar to what we’re talking about, I might be a dietitian who doesn’t specialize in eating disorders or disordered eating, but I might be seeing patients diabetes, whatever, that have some disordered eating. Chances are I’m going to, so I don’t need to specialize in that, but it would behoove me to be aware and have some skills.
And one of the things that Jessica said, a lot of dietitians are fearful about is I’m going to make this person’s eating disorder worse because I’m not an eating disorders specialist. And you talked something about re-traumatization and I don’t know if that’s the same thing, but if we’re worried about we’re going to say the wrong thing or do the wrong thing, or not have the skills in order to handle certain situations, can you speak to that?
Dr. Robyn Pashby (47:06):
Well, I mean, no dietitian should have the skills to treat trauma because that’s not your job in the same way that I should not have the skills to treat someone with managing kidney failure nutritionally, that’s not my skillset and that’s okay, but that doesn’t mean that I don’t talk about it with patients and talk about all of the associated feelings they have about doing that.
And so, the highest risk you have of re-traumatizing a patient is when you don’t know your own assumptions, that is the number one highest risk. So, if you do that step that I’ve implored people to do, which is to examine your own biases and assumptions, your chance of retraumatizing that person in your office drops precipitously because you understand that a flippant comment of this or a joke of that or something is suddenly not in the wheelhouse.
And by the way, I use humor all the time in my practice, so I’m not saying be boring and be in a box-
Melissa Joy (48:02):
Serious and yeah.
Dr. Robyn Pashby (48:04):
So, less education is never the answer defense. Always it is, look around the corner that you can’t see.
Melissa Joy (48:12):
Well, thank you so much, Robyn. This has been like I said at the beginning, it was going to be kind of heavy but very important, so important. I know you’re working on a book and I would love for you to tell us a little bit about that and any takeaways that you want to share with our listeners.
Dr. Robyn Pashby (48:28):
So, my book actually comes out in July of 2025 which is very exciting. We’re in the very final, it’s being printed as we speak. So, it’s called The New Food Fight. I’m a co-author with a couple of my long-term mentors and colleagues.
And what we do is we examine the sort of the bite, I guess you could call it between the eating disorder world and the weight management world and looking at how we can come together, essentially using a trauma-informed approach to work down the middle and to see that there’s much overlap in those two worlds and that people need to be treated as whole people and not their diagnoses. So, please look for that, it’s available for pre-order already, which is very exciting.
Melissa Joy (49:09):
Excellent.
Dr. Robyn Pashby (49:10):
And then I’ll also just plug, we’re health psychologists and my team, we’re actually licensed for virtual treatment in more than 40 states around the U.S. So, we work with patients in a lot of different places doing this sort of work.
So, we can treat trauma anxiety and anyone dealing with weight related struggles, diabetes related struggle, that’s our jam. We know all about the meds and all about the everything so that’s our thing.
So, I guess if I were kind of leaving a takeaway, it would be that I ask my healthcare provider colleagues to think about themselves, the way I ask my patients to think about themselves, which is what’s my own story and how does my own story affect my health interactions? And when we do that, and we do that for the people in front of us, so what’s that person’s story and how does that affect their health and their treatment plan?
We completely change the dynamic of that relationship in such a positive and enduring way and at the end of the day, we care about helping each other, all of us, patients care about helping you too. They want to perform. Patients want to “get better or do a good job for you”.
And so, if you’re aware of your biases and you don’t set up that dynamic, and you can actively say, “Hey, look, this is real life, you’re not going to be perfect, that’s okay.” Then suddenly the relationship gets so much closer, people get so much more actual help so it’s like a psychologically minded approach without being psychological treatment.
Melissa Joy (50:41):
Thank you so much. I will also connect with you afterwards and also pull together whatever resources, you’ve got your website, healthpsychologypartners.com, and you’re on LinkedIn and Instagram as well and then any other resources that you want to share with our listeners. So, thank you so much, this has been wonderful.
Dr. Robyn Pashby (51:01):
Thank you so, so much and I look forward to talking again in the future.
Melissa Joy (51:05):
Yes. Congratulations on the book.
Dr. Robyn Pashby (51:07):
Thank you. This labor of love, woo.
Melissa Joy (51:09):
Yes. Yes. Labor of love for sure. And for everybody listening, as always, enjoy your food with health in mind, until next time.
[Music Playing]
Voiceover (51:20):
For more information, visit soundbitesrd.com. This podcast does not provide medical advice, it is for informational purposes only, please see a registered dietitian for individualized advice. Music by Dave Birk, produced by JAG in Detroit Podcasts, copyright Sound Bites Inc, all rights reserved.
LISTEN, LEARN AND EARN
Listen to select Sound Bites Podcasts and earn free CEU credits approved by the Commission on Dietetic Registration (CDR) for registered dietitian nutritionists and dietetic technicians, registered. Get started!
Get Melissa’s Sound Science Toolkit here!
Partnerships:
Sound Bites is partnering with the Association of Diabetes Care and Education Specialists (formerly the American Association of Diabetes Educators)! Stay tuned for updates on the podcast, blog and newsletter!
Sound Bites is partnering with the International Food Information Council! Stay tuned for updates on the podcast, blog and newsletter!
Sign up for my monthly newsletter and episode eblasts so you never miss an update!
Listen on Stitcher (Android)
Install the Stitcher App
1. Search for “sound bites with melissa joy dobbins” 2. Choose Play Current Episode or Add to Playlist
Choose “Play Episode”
Subscribe & Review on iPhone
Open the “Podcast” app on your iPhone
Search for “Sound bites with melissa joy dobbins”
Open the podcast and click “Subscribe” and your done!
Write a Review
Click “Reviews”, then “Write a Review”.
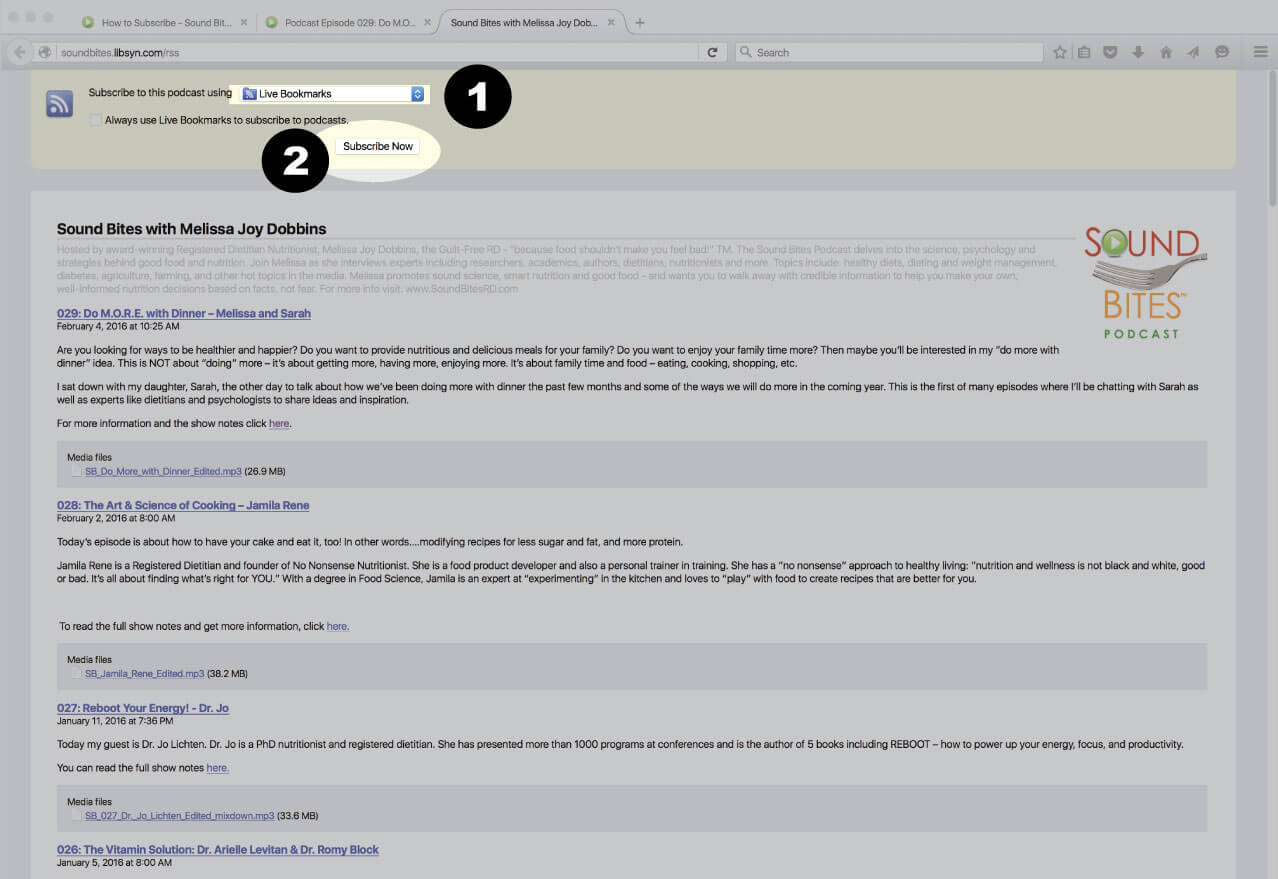
Subscribe via RSS Feed
Navigate to any podcast player . Click on the RSS feed icon.
Click on the RSS feed icon.
Click on RSS Feed
Choose which application you would like to use to receive the RSS feed
Click “Subscribe Now”
Confirm settings and subscribe.
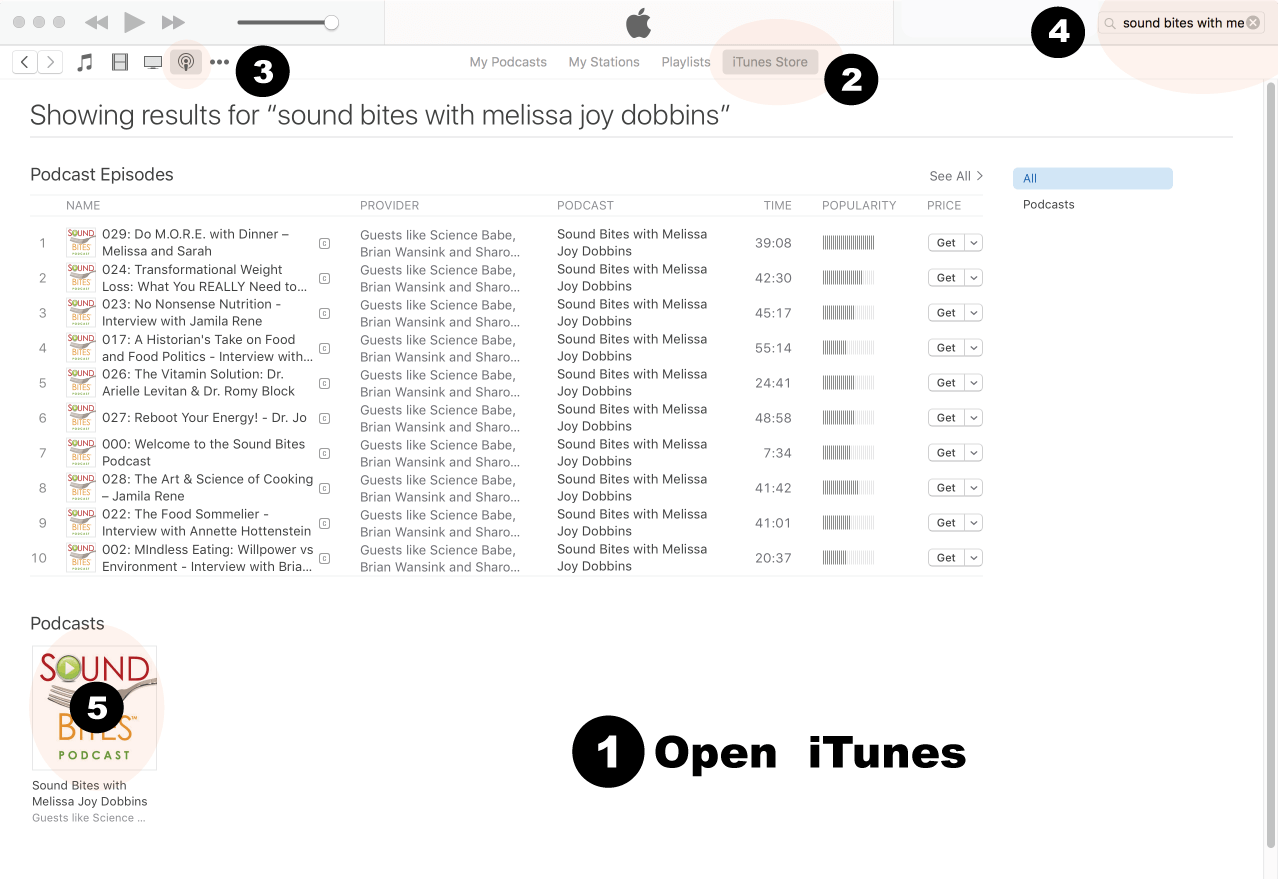
How to Review in iTunes
Open iTunes desktop application
Click iTunes Store
Click on Podcasts
Search for “Sound bites with Melissa Joy Dobbins”
Click on podcast image
Search for Sound Bites podcast in iTunes
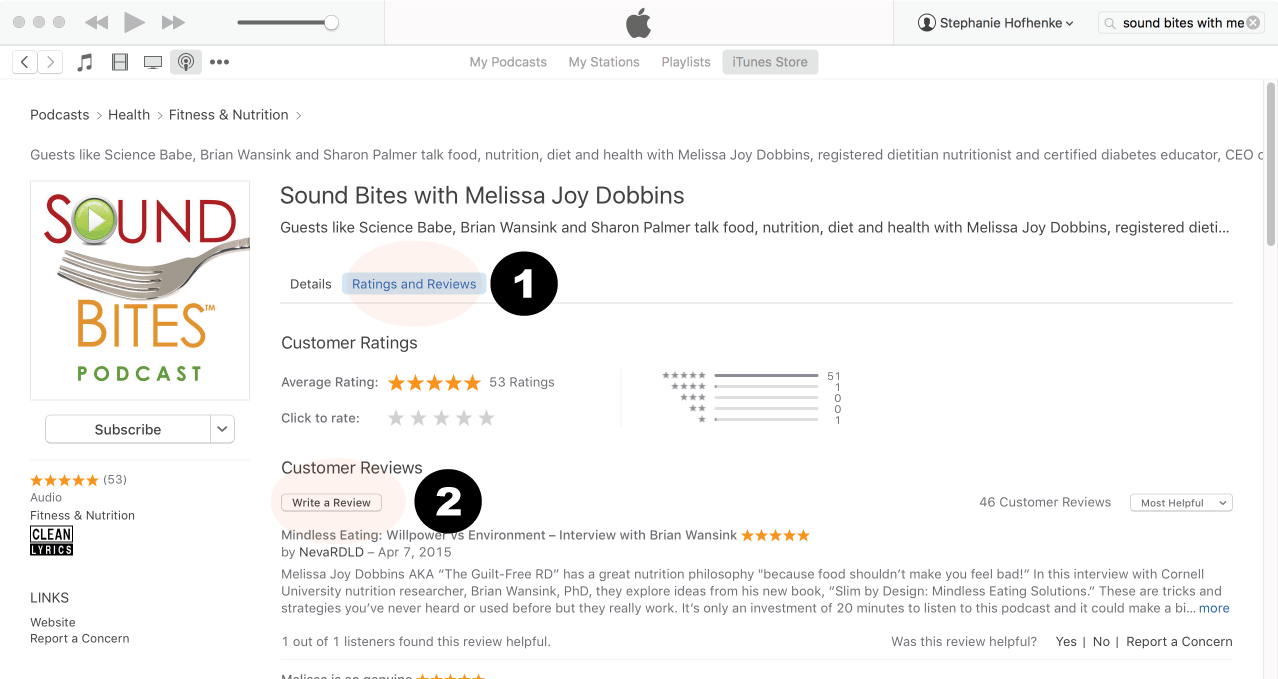
Click Ratings & Reivews
Click Write a Review
View reviews and write your own review.
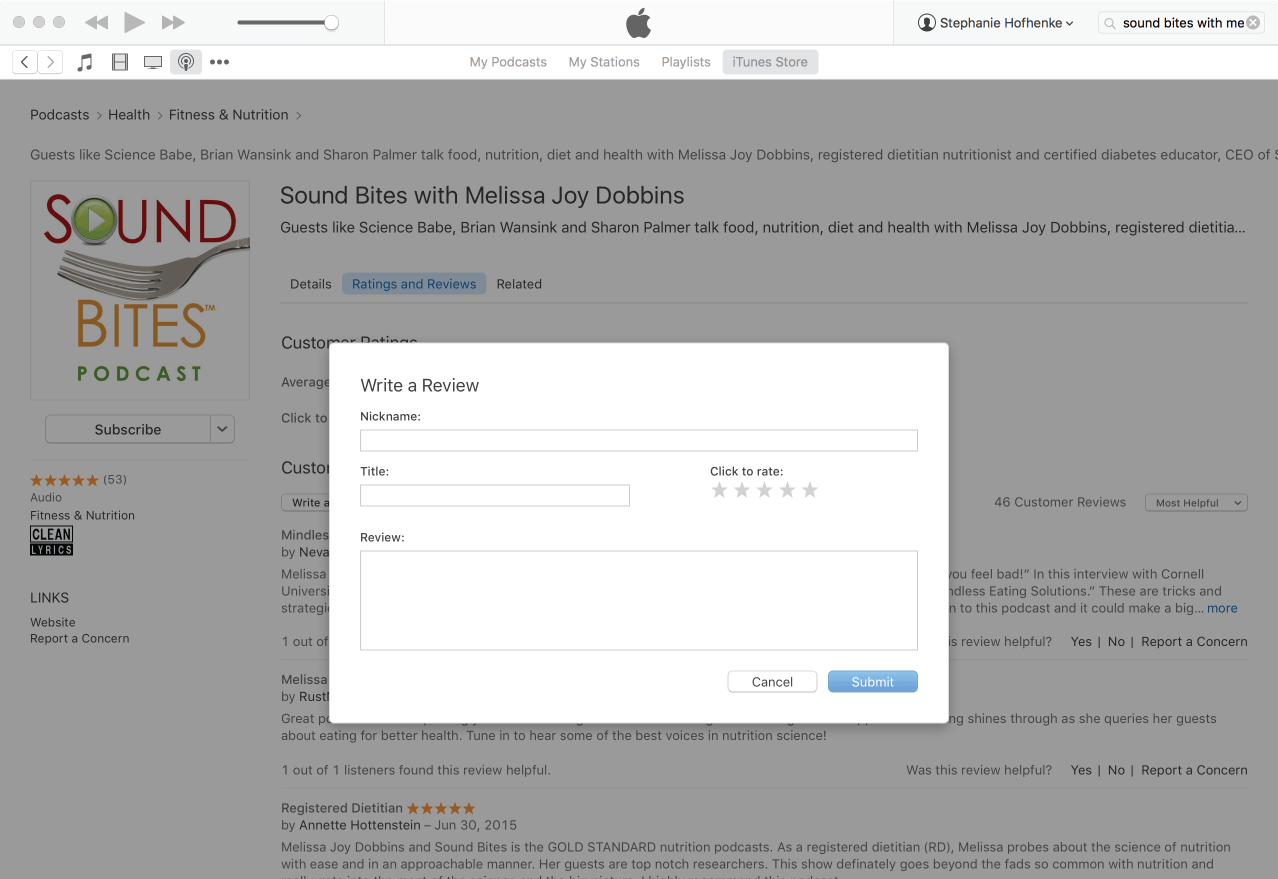
Write your review…. Thank you!
Write your review!
How to subscribe via iTunes
Click here to view the Sound Bites Podcastin iTunes, then click the blue “View in iTunes” button. This will open your iTunes application directly to Sound Bites Podcast. Click the “Subscribe” button, and your done!
 Dr. Robyn Pashby is a licensed clinical health psychologist and a nationally recognized expert in the psychological and behavioral treatment of weight and weight-related chronic health conditions. As the founder of Health Psychology Partners, she leads a team specializing in the complex intersection of mental health, obesity, and chronic illness.
Dr. Robyn Pashby is a licensed clinical health psychologist and a nationally recognized expert in the psychological and behavioral treatment of weight and weight-related chronic health conditions. As the founder of Health Psychology Partners, she leads a team specializing in the complex intersection of mental health, obesity, and chronic illness.