Celebrating over 1 Million Downloads and 50,000 Free CEUs on the Sound Bites® Podcast | NEW: Get 1 years’ worth of CEUs with the new 15-CEU Podcast Course
Injectable Weight Loss Medications & Long-Term Weight Loss Maintenance
Weight loss medications are nothing new – they’ve been around for decades. However, newer injectable medications originally intended for diabetes treatment have made their transition into the weight management space. As their popularity has surged, so have discussions about their safety, efficacy, side effects, and even their accessibility including costs and supply chain issues. These medications have also brought some attention to an important aspect of weight management that is often overlooked – weight loss maintenance, or in other words – keeping the weight off.
People can lose weight with the medications, but finding a lifestyle that allows you to keep the weight off is critically important. If you’ve lost weight, you feel good, you want to stay on the medication, great. However, if you don’t, for whatever reason – you can’t afford it, you’re having side effects, you miss food — we want to help give you a plan to keep the weight off. Without a plan, you’re almost guaranteed to gain the weight back.” – Dr. Jim Hill
Tune into this episode to learn about:
Different terms used and different medications available
Efficacy and safety considerations
Research on potential benefits beyond weight management
Issues regarding accessibility and affordability
Appetite suppression and decreasing “food noise”
Adverse events/side effects
Considerations for staying on the medication long term
If there is a “best diet” while on these medications
What the research is showing about decrease in muscle mass on these medications
The crucial aspects of lifestyle, exercise and mindset
If/what role they play in long-term weight loss maintenance
How long-term weight loss maintenance hasn’t received the attention it should
Resources for health professionals and the public
James Hill, PhD
Dr. James Hill is one of the world’s foremost experts in obesity and weight management. He is Professor of Nutrition Sciences and Director of the Nutrition Obesity Research Center (NORC) at the University of Alabama at Birmingham. Dr. Hill has published more than 700 scientific articles and book chapters. Many of these focus on the importance of healthy eating and physical activity in weight management and in preventing and managing chronic diseases. He has been continuously funded from NIH since 1981 and in 1998 received a prestigious MERIT Award from NIH. He is the recipient of several ASN awards, including the Centrum Center Science Award, the McCollum Award, and the David Kritchevsky Career Achievement Award in Nutrition. He has received the TOPS award and the George Bray Founder’s Award from The Obesity Society. He was the 2012 Atwater Lecturer for the US Department of Agriculture. Dr. Hill was elected to the National Academy of Medicine in 2014. Dr. Hill is a cofounder of the National Weight Control Registry, a registry of individuals who have been successful in maintenance of a reduced body weight. He recently launched the International Weight Control Registry to further investigate factors that contribute to successful weight loss management. He has a passion for translating research to address public health issues. He is co-founder of America on the Move, a national weight gain prevention initiative that aims to inspire Americans to make small changes to prevent weight gain. He is the author of the Step Diet Book, published in June 2004 and the State of Slim published in August 2013. He is co-host of a podcast entitled “Weight Loss and….”.
Resources
Some links may be affiliate links. As an Amazon Associate, I earn from qualifying purchases.
Welcome to Sound Bites, hosted by registered dietitian nutritionist, Melissa Dobbins. Let’s delve into the science, the psychology, and the strategies behind good food and nutrition.
Melissa (00:23):
Hello, and welcome to the Sound Bites Podcast. Today’s episode is about weight loss medications, specifically injectable weight loss medications, or GLP-1s, commonly referred to by their brand name such as Ozempic, Wegovy, Mounjaro, Saxenda, Zepbound (I think I covered all those brand names).
We’re going to discuss the different medications available, some of the side effects, benefits, pros and cons, but perhaps most importantly, considerations about keeping the weight off long term.
My guest today is Dr. Jim Hill. Dr. Hill is an internationally recognized expert in weight management. He has spent 40 years studying how people can achieve healthy weights. He’s professor of nutrition sciences, and Director of the Nutrition Obesity Research Center at the University of Alabama at Birmingham.
Dr. Hill has published more than 700 scientific articles and book chapters. Many of these focus on the importance of healthy eating and physical activity in weight management, and in preventing and managing chronic diseases.
He has been continuously funded from NIH since 1981, and in 1998, received a prestigious merit award from NIH, and he’s received many, many, many other awards as well. Welcome to the show, Dr. Hill.
Jim Hill (01:49):
Melissa, happy to be here.
Melissa (01:50):
I should say welcome back.
Jim Hill (01:52):
Yes.
Melissa (01:53):
You’ve been on the podcast twice before, way back in episode 24, and then in 79, and here we are in the 260s. Can you believe it?
Jim Hill (02:03):
Wow.
Melissa (02:04):
And you recently launched a podcast called Weight Loss And … So, I would love for you to share more about your background and the work that you do, and also, what your podcast is all about.
Jim Hill (02:18):
Yeah, I’ve been in this field for a long, long time. And when I first started back in the 1980s, no one cared about obesity, and I wasn’t an obesity researcher, I was studying body weight regulation. And then I think what we saw was during the 1980s that suddenly, obesity rates started creeping up.
Before 1980, less than 10% of Americans were obese. So, it wasn’t really anything people talked about or cared about or studied. And after 1980, being a smart guy, I said, “Ah, I’m an obesity researcher because this is something that’s getting more and more impact.” And look, today, everybody cares about this.
So, I started out actually very interested in the biology of weight management. Really, then learned, well, I didn’t see anything obviously wrong with the biology, maybe its behavior. And from there, well, maybe it’s the environment, and circling back to now, it’s all of those. It’s biology, its behavior, and it’s the environment.
So, I spent 26 years at the University of Colorado doing research in this area. I’ve been here at UAB for just over five years as Director of an NIH center, which supports nutrition research. So, we have over a hundred people studying obesity here in our center.
And recently, with my colleague, Holly Wyatt, we developed this podcast Weight Loss And … to really begin to share some of the things that we’ve learned, we interview a lot of other people from other nutrition obesity, research centers.
So, we talk to the top scientists, but the whole idea is we know a lot about how to manage weight, and sometimes, we’re not communicating that very clearly.
So, what we’re trying to do in the podcast is to give people some practical advice for managing your weight — for losing weight, but even more importantly, for finding a lifestyle that allows you to keep the weight you want permanently.
Melissa (04:19):
Excellent. Yes, you have long focused your work on the weight maintenance part, like you’ve lost the weight, how do you keep it off? In fact, one of the things I always tell people is that you co-founded the weight control registry.
And for the listeners who don’t know about that, I would love for you to explain what that is because it’s all about talking to people and doing the research, and looking at what the literature says, and just crowdsourcing everything to find out what works.
We know that losing-gaining, losing-gaining, yo-yo dieting, whatever, like there’s a ton of things you can do to lose the weight. Like keeping it off is that elusive goal, it seems.
Jim Hill (05:00):
The National Weight Control Registry was started in the early nineties with my colleague Dr. Rena Wing, who’s now at Brown University. We were having lunch and started talking about the fact that you saw so much in the media about how no one succeeds at managing their weight, at losing weight and keep it off.
And we were sort of joking and maybe there are people, maybe we should find them. And then we realized that’s not a bad idea. So, we started the National Weight Control Registry to find those people who had been successful, not just at losing weight, but at keeping it off. And we’ve published, gosh, maybe 60, 70, 80 publications on the National Weight Control Registry.
We learned so many things from looking at those people that have succeeded. One of the big ones for me, and you sort of hit on it; losing weight is very different than keeping weight off. There are different processes, they require different strategies. Unfortunately, the way a lot of people approach weight loss is go on a diet, stay on that diet forever.
Well, we have decades of showing that doesn’t work very well. So, we see losing weight as a separate process from keeping it off. And that’s where the drugs come in. The new medications — men, they’re fabulous for losing weight, unclear their role in weight loss maintenance.
Melissa (06:20):
Yes, and I encourage our listeners to dial back to episodes 24 and 79 because I learned so much from you in those conversations that really shifted even my own understanding of those different processes.
And correct me if I say this wrong, but one of the big ahas for me was that dietary intake or calorie level is what really drives the weight loss process, is the driver in that car, if you will. But the exercise is the driver in the weight and maintenance process, but it’s way more complex than that.
Jim Hill (06:56):
It is, but you’re exactly right, there’s no question. You can lose weight with exercise, but you have to do an amount that’s just not feasible for most people. The way you lose weight is go and eat less. There’s nothing wrong with that.
And in fact, research shows that just about every diet that’s been developed works for weight loss. You eat less, it’s a way to eat less. That’s not a strategy for weight loss maintenance. And if you exercise during weight loss, you may lose a little bit more weight, but it’s not the major factor. That totally shifts when you’re keeping weight off.
Now, exercise becomes the driver, and we could do a whole episode so many ways. It’s way more than burning calories. Essentially, exercise fixes your broken metabolism, it helps you manage your appetite. It has mental health effects. It’s to the point where we tell people, if you’re not prepared to substantially engage in regular physical activity, you’re not likely going to be successful in keeping your weight off.
You can lose it, but you aren’t going to keep it off. Doesn’t mean diet isn’t important. If we could get the population to be a little bit more active, Melissa, then we could do amazing things with diet. The problem is diet is contributing to the obesity, and unless we get people’s energy expenditure up, they can’t eat enough to effectively maintain their weight.
Melissa (08:19):
Wow, okay. So, let’s jump into the topic of weight loss medications (and I should mention this episode is not sponsored).
So, I’ve been doing a little bit of research on this and was surprised and sort of not surprised to learn that the terminology we’re using is current but perhaps already outdated. So, of course, you hear the brand names in the ads, and at the water cooler, if we still have the water cooler (I don’t know, just from friends and family).
But amongst professionals, we kind of refer to those as the GLP-1s. And I’m a certified diabetes educator, and we could maybe touch briefly on these started off as diabetes medications, and then my understanding is we saw, oh hey, there’s a weight benefit. Maybe this could apply to people without diabetes.
And I should say GLP-1s, what that means is glucagon-like peptide-1 receptor agonist. There’s also GLP-1/GIP glucagon-like peptide-1 receptor agonist/glucose-dependent insulinotropic polypeptide dual receptor agonist. Yeah, that’s why I’m a diabetes educator.
Jim Hill (09:26):
Tongue twisters, aren’t they?
Melissa (09:27):
Anyway, so, oh let’s just call them anti-obesity medications, right? Wrong, that’s getting a lot of pushback, calling them anti-obesity medications. And I was like, well, aren’t they just like injectable diabetes/weight loss medications? But some of the newer terminology I’ve been hearing is incretin-based therapies or nutrient stimulated hormone-based therapies. Again, a mouthful.
So, I don’t know if you have heard any other terms or like what people are referring to those, but I just wanted to kind of put this out there for people listening that if you hear these terms, that’s all under this umbrella that we’re talking about.
Jim Hill (10:03):
The problem is there’s no consistency. People are using different words out there to describe them. We’ve had weight loss medications for a long, long period of time, the difference is we’ve never had ones that are as effective as these medications.
And the two you mentioned, one is based on GLP-1 and the second is GLP-1 plus GIP. What these medications do is to essentially greatly amplify your body’s natural signals of satiety. So, you’re making GLP-1 right now, I’m making GLP-1.
And what that does, it’s a signal from our GI system telling our brain that we’re full, we don’t need to eat. What these medications do is boy, amplify that hundreds or thousands of time so you get this huge signal that really tells your body that you’re full, you don’t need to eat. And consequently, it allows people to eat less without being hungry.
If you don’t take the medication, you eat less, you get hungry. What this does is to prevent that hunger that occurs when you eat less.
Melissa (11:14):
Right. Thank you. Yes. So, weight loss medications are not new at all, you know this. And when I was doing my research, I was reminded of some of the weight loss medications that I was using with patients. I didn’t prescribe them, but that my patients were on way back when I was an outpatient dietitian in the mid to late nineties.
So, there’s seven medications with FDA approval for weight loss. Four of them are oral and then these three GLP-1 injectables. So, thank you for explaining like in general how they work. And we know that appetite suppression or appetite control is a big factor in helping people lose weight.
And then we’re going to talk about food noise too because this is a kind of a new term that’s come up with this that I think is really important as well. But because these medications were originally used for diabetes, and oftentimes, the medication is indicated for one thing, but it has other effects, then are used, I don’t know, off label is the right term or whatever, but it’s discovered, “Oh hey this medication also does this.”
So, it’s kind of not surprising that we’ve seen sort of this aha with, “Oh, these could help with weight management.” But besides weight management, let’s just touch briefly on are there other benefits, and if so, what are those? I’ve seen some things in the news, but I’m curious as to what you are seeing.
Jim Hill (12:36):
Yeah, so to put it in perspective, most of the chronic diseases we’re dealing with: diabetes, heart disease, cancer, kidney disease are obesity-related. If you’re obese, it increases your risk of getting those. What we’re seeing with these medications is the weight loss is accompanied by an improvement in diabetes, kidney disease, heart disease, maybe even cancer.
What it shows to me, Melissa, is the value — if we could prevent or treat obesity, it would be more than the weight effects. It would really reduce all these chronic disease. So, in my mind, it’s the weight loss that’s driving these, and it shows the potential of weight loss to improve health in an individual and in a population.
Melissa (13:27):
Okay, thank you. Yes, and one of the things that we’ve known for a long time in the healthcare community, and I recall like really holding onto this as a diabetes educator is oftentimes, it’s not a huge amount of weight that you need to have in order to see a significant improvement in health markers and health outcomes.
And I think we’re going to touch on this because I know that there’s a study that you did where you were kind of talking about what people’s weight loss goals were, and I think it ties into that, where it’s like what people want to weigh and want to lose is maybe even more extreme than what’s needed to get some of these health benefits.
Jim Hill (14:05):
You’re exactly right. I think we have some pretty good evidence that weight loss even as little as 5% can improve health. But we’ve had a mismatch between expectations. So, if I put someone through a weight loss program and they lose 5% and I see their lipids are improved and so forth, that person’s not likely to see it as success.
I might as a healthcare professional say, “Oh wow, that’s successful.” And they’re saying, “I only lost 5%, I wanted to lose 40% or 50%.” What we found is when we ask people who were entering a weight loss program, how much weight they wanted to lose, their goal weight was 20 to 25%.
Melissa (14:49):
Of their current body weight?
Jim Hill (14:50):
Of their starting body weight. Some of these early medications and lifestyles can maybe produce 7 to 10%. So, you can see the mismatch. Even though 7 to 10% is going to improve your health, it wasn’t what people were expecting. And so, you had people losing 10% who saw that as a failure.
Well, rightly or wrongly, these medications on average can produce 15 to 20% weight loss. So, for the first time in my career, I’m seeing a lot of people lose weight and actually hit their goals. Traditionally, we would help people lose weight and lose 10% and that’s great, but I want to lose more, I want to lose more.
So, people weren’t very interested in weight loss maintenance. This has always been the issue with … I’ve been interested in weight loss maintenance, but nobody ever is in weight loss maintenance. I’ll get there when I lose another 5 pounds or 10 pounds or 20 pounds.
Things are different because with these medications, people are actually meeting their goal weight loss. Now, we have to help them keep it off.
Melissa (15:53):
Yes, excellent. I do want to mention just briefly if people are interested, some of the recent studies that have come out to show some benefits beyond weight loss, but to Dr. Hill’s point, related to weight loss likely, is the select trial.
There was some cardiovascular benefits, we’ve seen improved glucose control, insulin resistance, and then there was a study that was just published in the New England Journal of Medicine that showed that Ozempic cuts the risk of chronic kidney disease complications. So, if you want to look into that, I’ll link those articles in the show notes at soundbitesrd.com.
Let’s talk before we talk more about the appetite suppression, the decreased food noise, some of the things that I’m personally concerned that I’m hearing about decreased appetite, and therefore, intake. But let’s address the fact that the medications can be difficult to access, they’re expensive. Like talk to me about what’s going on there.
Jim Hill (16:49):
Yeah, the problem is that they become way too popular. So, not everyone who wants them, and not everyone even who has a prescription for them can get the medications. Now, the pharmaceutical companies are obviously working to solve that. They’re trying to make more of it.
Melissa (17:07):
I would think.
Jim Hill (17:07):
Because if the demand exceeds supply, they’re trying to ramp up the supply. But two problems: one, it’s hard to get, and two, it’s expensive. And so, you’re actually finding places offering compounded versions of these medications.
A pharmacy can do that. If there’s a shortage of medication, they can do it. So, they’re essentially going out and making their own medication. This is very different from the drug companies’ medications that are tested, and FDA approved.
So, some of it’s probably okay, some of it may be a little suspect, but there’s so much demand that people are doing anything to try to get access to these medications.
Melissa (17:52):
Right, yes. My understanding is that the compounded medications are not recommended. I’m not an expert in that area, but I believe that that’s what I’ve heard. But I’ve also heard that some of the supply chain issues have to do with the needles, and the actual equipment.
Jim Hill (18:10):
So, these are injectable, but they package it in these things that are just so easy to be injected with a pen. So, don’t think of a big needle.
Melissa (18:19):
So, it’s not like a syringe, it’s in a pen.
Jim Hill (18:22):
Yeah, it’s a little pen and you just prick yourself, and people don’t find it very aversive at all. But again, that’s part of the packaging, the medication, and the injectors.
Melissa (18:33):
Okay. So, let’s focus on the appetite issue, and let’s talk about this food noise. We hear all the time, it’s like for some people, it just settles that food noise. And as a dietitian and just my own personal experience, I can appreciate how much that noise just interferes with people’s daily business.
I often would tell people like, “I’m a dietitian, I’m supposed to think about food all day. Like, oh my gosh, I wouldn’t want you to have to worry about what you’re going to eat, what you’re not going to eat like all day long. You have other things to think about.”
So, what are you seeing out there as far as the food noise and how beneficial it is to just kind of quiet that?
Jim Hill (19:17):
Actually, that’s a term I’d never heard until recently.
Melissa (19:22):
Yeah.
Jim Hill (19:23):
And I didn’t understand it at first, but after talking to people, I think it’s critical. So many people say, “What’s happened with these medications — I used to spend so much time thinking about food, my next meal, those chips in the cupboard, da, da, da … I don’t do that anymore. The noise is gone.” Wow, that is amazing.
And that’s different from the hunger being gone, because again, we eat because we’re hungry, but we eat because of all these external cues too, even if we’re not hungry. That’s the part that goes away with the hunger and it’s totally amazing. And people say for the first time, I don’t have to deal with all this noise about food in my daily life.
Melissa (20:08):
Yeah. I mean, how freeing is that? And to your point, they are two different things. Some people … I’ve said this on the podcast before, like I don’t get that hungry. I don’t have a big appetite. That’s not an issue for me. It doesn’t mean I don’t take in extra calories or empty calories.
But I’ve talked to so many patients and have known people who like that’s a huge issue for them. I had never heard that term food noise before either. But it makes so much sense.
Jim Hill (20:34):
It fits. The more I talk to people, the more I think it’s a good term, and I think it’s something that’s very important.
Melissa (20:40):
Yeah, and it’s interesting that like not only had you not heard that term, but at first, you didn’t quite understand because you work in this space. And I think it’s like maybe that’s something that at least other people can understand, “Oh, this is why it’s been so hard for you.”
Jim Hill (20:54):
One of the things that we’ve been talking about doing on our podcast, is we talk to a lot of these experts, Melissa, and they’re these people that have never had a weight problem. And they’re very smart, good people, but they’re just assuming that people can do these things.
And I think unless you’ve been there, you don’t understand the power of those environmental things and like food noise. If you’ve never experienced food noise, it’s hard to understand what it is. And I think we have to have a better appreciation of what people have been going through with that.
Melissa (21:32):
Amen, a hundred percent. I could not agree more. I think that that’s so important. My big concern is, and I’ll say I have a family member who I’ve been wanting to go on Wegovy or Ozempic or something for a long time, but the more I learned about it, the more I realized, “Oh my gosh, some of these people their appetite is so suppressed (we’re going to talk about some side effects: nausea, vomiting) that I’m afraid they’re malnourished” and I’m sure some of them are.
Like there’s a difference between quieting the food noise, suppressing the appetite, and then being so nauseous or like no appetite at all that you’re not getting adequate nutrition or hydration.
Jim Hill (22:14):
See, this is something I worry about too. I had one woman tell me she has to set her alarm clock to eat. I worry in that situation. I think it’s great you’re not overeating, but we have to worry about people being malnourished as well.
So, there’s a good side to that, and there’s a watch outside too. And I think we have to balance those.
Melissa (22:35):
And from the little that I’ve learned, my guess is that part of that is which medication you’re on because they each have different sort of personalities if you will. And also, the dosing. Of course, I’m going to give a huge shout out to the important role of dietitians in this process.
And it’s not really the scope of our conversation, but if we haven’t touched more on it as we go through, I will kind of give some more specifics as we wrap up because it is a different world, it’s a different approach.
Jim Hill (23:05):
Well, I think dietitians should welcome these tools. They’re not threatening at all. I mean, for me, boy, the fact that people reach their weight loss goals, now, I can go in and do what I do best. And I think that’s the same thing for dietitians. I think there’s such an opportunity for taking people that succeed on the medications now working with them on lifestyle.
Melissa (23:31):
Yes, absolutely. And I think a lot of people just assume, oh well, dietitians aren’t needed because of this, but it couldn’t be further from the truth. It is a different role. So, now, your counseling will focus not on how to decrease your appetite and your calories and to control that and to manage the food noise — it can actually be focused on how do you get adequate nutrition.
Jim Hill (23:53):
Absolutely.
Melissa (23:54):
How do you get adequate hydration? How do you preserve that lean body mass and protect your bones as you lose weight? I think it’s just an really exciting opportunity, but I think dietitians need to be at that table and need to make sure that people understand.
And a huge role for the dietitian is to communicate some of these side effects and say, you know what, the patient’s afraid to tell the doctor that they’re so nauseous because they don’t want them to take them off the medication. But the dietitian’s like, “I’m concerned they’re dehydrated, they’re not getting adequate nutrition, can we titrate the dose back a bit? Can we try a different medication?” It’s really important.
Jim Hill (24:29):
Couldn’t agree more. Huge role for dietitians.
Melissa (24:32):
Let’s talk a little bit about most people seem to do well losing the weight, but then what? Obviously, nobody wants to stay on medications any longer than they have to, which is a whole other can of worms that we could talk about because I think there’s a lot there to say.
But I’ve heard with other weight loss medications, as with most medications, if it’s going to work, you have to stay on it. What are you seeing as far as like long-term on these medications? People wanting to come off obviously.
Jim Hill (25:05):
So, the medication works because it alters your biology, but it doesn’t do that permanently. Doesn’t make a permanent change in your satiety signal. So, once the medication goes away, you’re no longer going to get that fullness. Perhaps, the food noise comes back, things happen, insulin sensitivity decreases. So, the medication only works if you take it.
So, the model, I think on which this was developed is these are chronic medications. We have other examples of that. People take medications for management of blood pressure, management of cholesterol. And they take these with the idea of they’re going to be taking them forever.
I think that’s the model on which a lot of the experts are thinking right now. But one of the things that we see is, for various reasons, we don’t have exact data, but it looks like most of the people that go on these medications don’t stay on them over the long term.
And there are a lot of reasons for that. You talked about side effects is one reason. We see people that say, “I lost the weight, but I have no energy, I don’t feel good.” They’re the people that miss food. If you were to take away your love of food — I don’t know, you’re probably like me. You enjoy food, sharing meals with friends. And if that’s no longer something that’s pleasurable, that can be a negative.
People worry about they affect some body composition, you might lose muscle mass. So, there are various reasons people might not do it.
But what we’re trying to also say; if you don’t, don’t regain the weight. Don’t just go off the meds. If you go off the meds without a plan, most likely, you’re going to regain the weight. So, there is an opportunity if for whatever reason you want to go off the meds after you’ve lost the weight.
This is where dietitians, other lifestyle people become really critical. It is possible to do that, but you have to have a plan. Without a plan, almost guarantee you’re going to gain the weight back.
Melissa (27:19):
And that’s if you can access the medication to stay on it.
Jim Hill (27:24):
That’s right. You have to get them in the first place. And again, they’re doing a lot of research with the meds on low doses, tapering, intermittent use. Maybe you go off the meds with lifestyle, but if you go through a rough patch, you come back on the meds for a while.
These are wonderful tools. What we have to figure out is how to use those tools. Yes, we know they work for weight loss, their role in weight loss maintenance, unclear. There probably is a role and I think we will learn how to use them more effectively interspersed with lifestyle.
Melissa (27:59):
Very interesting. So, we’re seeing more articles or chatter about the best diet on a GLP-1. Can you address that?
Jim Hill (28:09):
I’ve looked at those because to me, what everybody is putting out there is a healthy diet. They’re saying the same sort of advice they would give anyone, and maybe that’s it. But I think Melissa, we really don’t know. I don’t think we have sufficient research to know specifically about the best diet to match the drugs.
We can say eat a Mediterranean diet, or a DASH diet, or a healthy diet, or increased protein — fact of the matter is we don’t have a lot of research that would help us understand specific ways that we might modify diet to be synergistic with the medications.
Hopefully, we’ll get some of that research and we will learn more. But the best advice people are giving right now is just to eat a healthy diet.
Melissa (28:56):
Well, and it makes me think, well, what is the best diet overall anyway? I mean, obviously, the Mediterranean diet always wins, number one, DASH diet is up there, but it depends on the person. But I’m wondering with hearing more in the news lately about decrease in lean body mass, maybe the best diet is one that just really prioritizes the protein.
I’m not saying a high protein or whatever, but what are you hearing? I mean, obviously, we know anytime you lose weight, some of that is going to be muscle. And you try to mitigate that as much as possible. But what are you seeing with some of these reports about more lean body mass being lost? Is it maybe just the speed of weight loss?
Jim Hill (29:35):
We don’t have the answer there. It’s a concern, but we don’t have enough data to say yes or no. So, if you were going to go on a lifestyle program and lose weight, 20 to 40% of that weight loss will be from lean body mass, and 60 to 80 will be from fat.
The question is, if you lose weight on the medications, does that increase the loss of lean mass, decrease the loss of fat mass? We don’t know, and we need lots more research. What I suspect is there are going to be groups that may be concerning and others not.
For example (and I’m in that group), elderly people where muscle mass is so critical as you age. In fact, a huge predictor of longevity. So, I would be really concerned at people in their sixties, seventies, eighties, making sure that when they lose that weight, it’s not an inappropriately loss of muscle mass. We don’t know that.
So, right now, it’s a concern. We just don’t have enough data to know for sure. But it’s something I know the pharmaceutical companies are paying attention to it, and they’re trying to get some data. So, whether or not it’s going to turn out to be a problem, we don’t yet know, but we need more information.
Melissa (30:56):
Very good, very interesting. And to that point, I’m guessing, I mean we don’t really have long-term data on these medications for weight loss, but we have some long-term data because of medications for diabetes, right?
Jim Hill (31:10):
We’ve used them for diabetes, but for weight loss, two to three years of data is all we have. Now, whether they’re going to continue to be effective, I think most people are assuming they will. We see that with lipid medications and blood pressure medications. So, the idea is if you continue to take them, they’re going to be effective.
We don’t know that, and we need more information. It’s just going to take time to have people on those medications long enough to look for. And like anything, we’re always looking for potential negative effects.
But so far, I mean, these medications, yes, they’ve had some of the problems we’ve talked about, but they’ve been pretty darn effective with certainly for most people, manageable side effects.
Melissa (31:57):
Well, maybe the best diet for these medications is resistance training.
Jim Hill (32:02):
Well, don’t laugh because-
Melissa (32:04):
I know, but I’m saying the diet.
Jim Hill (32:06):
Absolutely. I would say without any data, if you’re concerned about lean body mass, a little more protein, a little more exercise are the two things that logically make sense. We don’t know if that works or not, but logically, it makes sense.
Melissa (32:21):
Well, yes, and to your point, there’s an article, an excellent article written by Hope Warshaw that I’ll link in the show notes as well. It was either in her article or in some of the three-part webinar series that the academy has, which I’ll also link in the show notes.
And it’s like we don’t exactly know what the “best diet” is, for this, but we do know that a healthy diet, a nutritious diet and regular exercise is important and it’s good for health. So, we’ve got to fall back on that. And by suppressing the appetite and decreasing this food noise, maybe people can actually focus on that, and build some healthy habits.
Jim Hill (33:01):
And I think you’re going to need that regardless of whether you stay on the drugs or not. Even if you stay on the medications, I can’t believe that these things are going to most effectively work alone if you’re sitting on the couch all day eating a crappy diet. So, I think lifestyle is going to turn out to be critically important either way.
Melissa (33:23):
And lifestyle will finally get its day in the sun. There was one other thing you wanted to talk about: mindset, and of course, if there’s anything else you wanted to say about exercise.
Jim Hill (33:35):
Exercise, yeah. We have looked at this over and over and over, and put simply, it’s almost impossible for most people to maintain a significant weight loss without exercise. Now, the medications, in some way, it’s ironic they’re kind of playing the role that the exercise plays.
Because what exercise does, if you lose weight, your energy expenditure goes down because you have a smaller body. It means you have to eat less forever, and that’s been the difficulty with weight loss.
Now, one of the ways that we found that works is if you get people to exercise, they can now increase their food intake without gaining weight. Medications work the opposite way. They allow people to continue to eat less to match their low energy expenditure.
I’ve always believed that it’s important — I think the way our bodies work best is when we’re expending a lot of energy and we’re eating a lot of energy. We never developed biological systems for food restriction. We developed biological systems to eat.
And the only way then that you can manage a healthy way with that kind of biology is to have a high level of energy expenditure, except if you bring medications in to alter the intake side. So, you can see there are two different approaches.
Without the medications, I would say you have to exercise to keep weight off. And I think even with the medications, exercise is going to give you that little extra ability to do more on the food intake side without regaining your weight.
Melissa (35:16):
Yes, and hold on to some of that muscle mass.
Jim Hill (35:19):
Yeah. It also preserves your muscle mass, you’re right.
Melissa (35:22):
And what did you want to say about mindset?
Jim Hill (35:24):
One of the things we’ve learned is the brain is a key organ in weight management. And people sort of put weight loss aside: “I’m going to do over here on this journey of weight loss and then we’ll get back to the rest of my life.” And what we’ve learned is the two are related. If you want to change your weight permanently, you change your life permanently.
I mean, literally, we haven’t talked about the environment you’re in, the social network you’re in, it’s hard to go and see weight loss as one thing you do and then you come back to normal life. We found the people that are really successful at losing weight and keeping it off, change every aspect of their life.
Now, what they tell you, it’s positive. So, again, but just saying, I’m going to do my diet and exercise and not worry about anything else, I don’t think it works. I think you’ve got to think about, we talk about your identity, who do you see yourself as? Do you see yourself as a formerly obese person or do you see yourself as an adventurer or an athlete? The mind is so important in all this.
Melissa (36:32):
No, that’s huge.
Jim Hill (36:34):
We could do a whole episode on mindset.
Melissa (36:36):
We’ll have you come back and do that, I’d love to talk about those things. But now, I want to hear about this new book that you’re working on because I think it’d be very timely for people who are like, “I’ve done these medications, I’ve lost weight, now what?”
Jim Hill (36:49):
My colleague, Holly Wyatt and I, are doing a book on how
What we’re trying to do is to say, if you don’t, for whatever reason, you can’t, you can’t afford it, you’re having side effects, you miss food — whatever those reasons, we want to help give you a plan to keep the weight off.
And Holly and I have studied weight loss maintenance for years and years and years. And in fact, we laugh because it’s the perfect timing for us. Nobody cared about this before because everybody wanted to lose weight. They didn’t want to be in maintenance.
Now, it’s like, holy cow, this is our time. We can take everything we’ve learned from the Weight Control Registry, from our own research, and we can give people options, and the whole idea is we’re going to give people different options. There’s no one size that works for everybody.
We’re going to give people a lot of different strategies, and we’re going to hopefully, have them try out different things, try out different dietary approaches, try out different exercise approaches, and we hit heavily the mindset part. How do you get in the mindset that’s going to help you keep the weight off?
So, we’re very excited about writing this because it’s the work we’ve been doing, and we’ve been wanting to do this. It’s just that until now, no one cared about this topic. And now, people do. So, it’s very exciting for us.
Melissa (38:34):
Very exciting, yes. And it’s exciting for everybody because it’s the most important piece of that puzzle. And I mean, they’re all important pieces, but-
Jim Hill (38:45):
I used to say that weight loss maintenance is hard, and Holly, every time I would do that, she would just, “No, no, no, no.” And she finally convinced me, if you approach it as, “Oh, this is something to do that’s hard …” And through her work and through our conversations, it can be an interesting journey. It doesn’t have to be hard, you can learn so much about yourself.
So, I say don’t see it as hard, see it as interesting. And one thing we know, at the end, everybody we study who succeeds almost to a person says life is better after this than before. So, it’s an interesting journey that helps you learn more about yourself and it takes you to a place that you’re going to be happier.
Melissa (39:34):
Well, you know that makes me think of one of the previous episodes we did about transformational weight loss. Transformational, life-changing-
Jim Hill (39:43):
And it does, it requires a transformation. In a way, going on a weight loss journey is really a chance to reinvent yourself. You really can’t. So, don’t think of it as just going and doing diet and exercise. Think about who you want to be as a person, and how you can use this journey to do more than change your weight, to change your attitude, to change your identity, to change how you interact with people. And that’s why I quit saying it’s hard, I’m saying, “Wow, it’s an interesting adventure.”
Melissa (40:14):
No, that’s huge. And yeah, the identity piece, it’s so true. And I think for people to hear that and to try that on mentally and that mindset, I think is really important. So, thank you.
Jim Hill (40:28):
A few years ago, Holly and I were involved in a reality TV show, Extreme Weight Loss. And these are people … it’s not The Biggest Loser, it’s very different. These are people that went through a yearlong transformational program, and we always talked with them at the end.
And on average, these people lost half their body weight. They weighed half as much at the end/in the beginning. And when you ask them what was valuable, they always mentioned weight loss, but it was never in the top two or three or four answers: “I am a better person, I interact more with my friends, I’m happier. Oh, by the way, I lost 150 pounds.”
So, it’s in there, but we’re talking in our book about redefining success. It’s not just the scale. If you’re defining success as the scale, you’re missing a big opportunity to reinvent yourself.
Melissa (41:23):
Oh, wonderful. That’s a wonderful way to wrap this up. Where can people find your podcast and connect with you, and keep updated on the book?
Jim Hill (41:34):
So, the podcast, you can get it at weightlossand.com, it has all the episodes. We release one every Wednesday, so it keeps us rolling. I’m in awe of your numbers. We’re in the double digits and you’re in the triple digits, so I’m impressed with that.
But yeah, take a listen. We try to translate the science into practical application, so weightlossand.com. We’re in the process of writing the book, in the best of circumstances, it’ll be out sometime this year, but stay tuned.
Melissa (42:06):
Okay, excellent. And I know you’re on Apple, I’m sure you’re probably on Spotify, like the big places where people listen to podcasts. But definitely, want people to go to the website weightlossand.com because that’s the central hub for everything.
And as I mentioned, I’ll link to the three webinars from the academy, that’s eatrightpro.org, and this article that Hope Warshaw wrote, and anything else like the research studies, anything else I can gather, I’ll put those in the show notes at soundbitesrd.com.
Well, thank you so much Dr. Hill for coming on the show. It is always a pleasure to talk with you and I enjoyed seeing you and your lovely wife Trish back in Alabama when I was there in March for my conference, and we had the idea to do this podcast.
Jim Hill (42:54):
Well, it’s always nice talking to you, and thanks for everything you do. You just have a wonderful ability to get important messages out to people. And people can do this weight loss thing. I know people have failed over and over and over. Don’t give up, we see so many people transform their lives. It is possible.
Melissa (43:15):
Oh, thank you for being so inspirational. And for everybody listening, as always, if you liked this episode, share it with a friend, tell a coworker, tell them about the podcast, listen to another episode. And as always, enjoy your food with health in mind. Until next time.
[Music Playing]
Voiceover (43:31):
For more information, visit soundbitesrd.com. This podcast does not provide medical advice. It is for informational purposes only. Please see a registered dietitian for individualized advice.
Music by Dave Birk, produced by JAG In Detroit Podcasts, copyright Sound Bites, Inc. All rights reserved.
LISTEN, LEARN AND EARN
Listen to select Sound Bites Podcasts and earn free CEU credits approved by the Commission on Dietetic Registration (CDR) for registered dietitian nutritionists and dietetic technicians, registered. Get started!
Get Melissa’s Sound Science Toolkit here!
Partnerships:
Sound Bites is partnering with the Association of Diabetes Care and Education Specialists (formerly the American Association of Diabetes Educators)! Stay tuned for updates on the podcast, blog and newsletter!
Sound Bites is partnering with the International Food Information Council! Stay tuned for updates on the podcast, blog and newsletter!
Sign up for my monthly newsletter and episode eblasts so you never miss an update!
Listen on Stitcher (Android)
Install the Stitcher App
1. Search for “sound bites with melissa joy dobbins” 2. Choose Play Current Episode or Add to Playlist
Choose “Play Episode”
Subscribe & Review on iPhone
Open the “Podcast” app on your iPhone
Search for “Sound bites with melissa joy dobbins”
Open the podcast and click “Subscribe” and your done!
Write a Review
Click “Reviews”, then “Write a Review”.
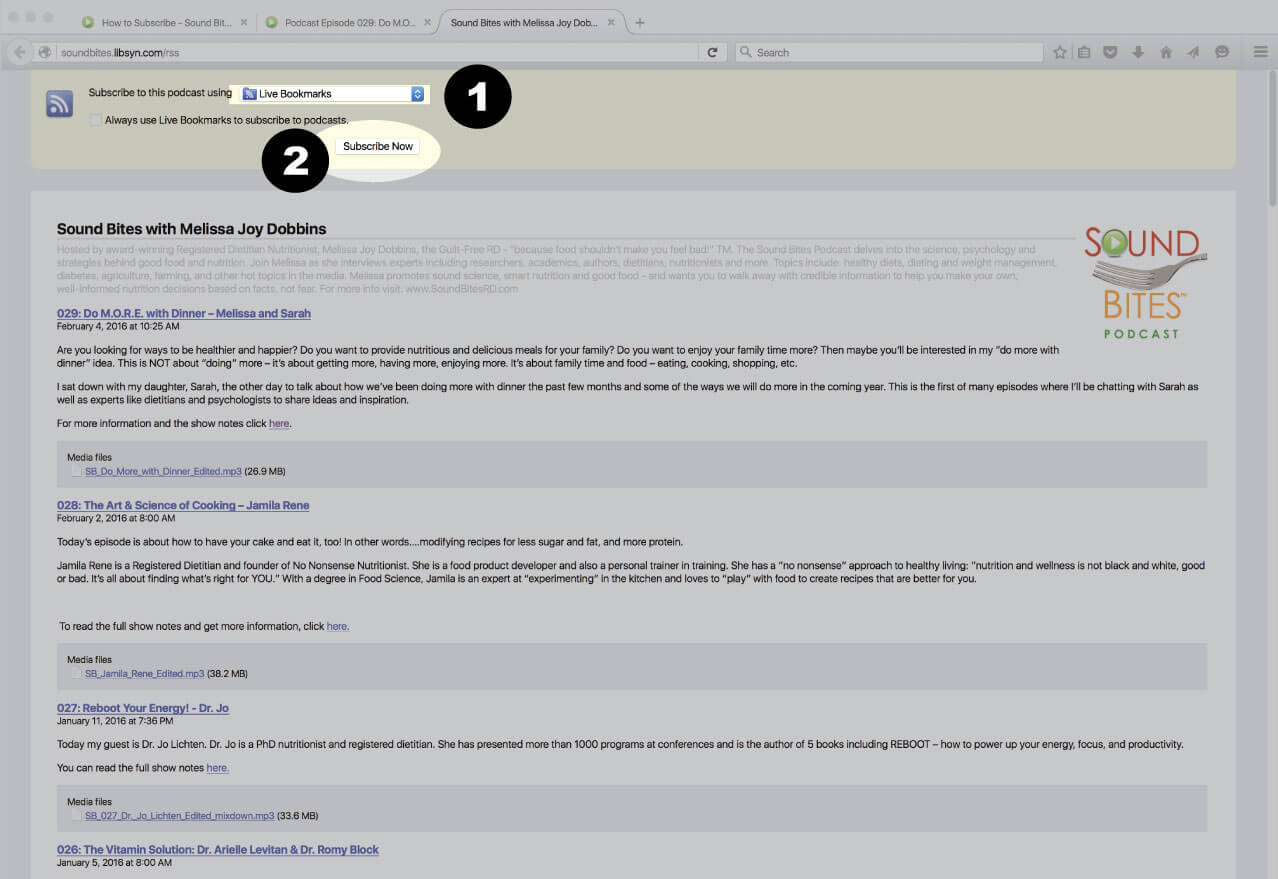
Subscribe via RSS Feed
Navigate to any podcast player . Click on the RSS feed icon.
Click on the RSS feed icon.
Click on RSS Feed
Choose which application you would like to use to receive the RSS feed
Click “Subscribe Now”
Confirm settings and subscribe.
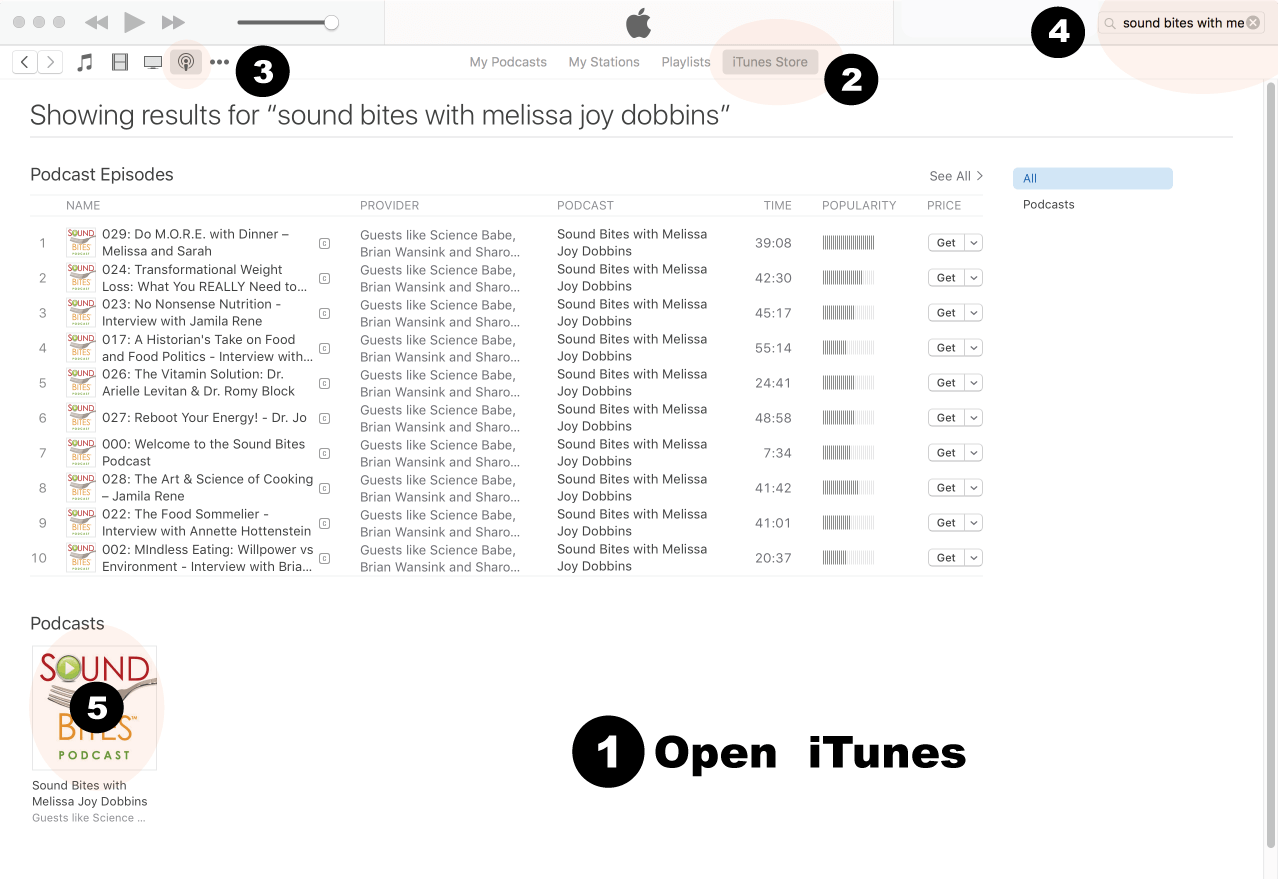
How to Review in iTunes
Open iTunes desktop application
Click iTunes Store
Click on Podcasts
Search for “Sound bites with Melissa Joy Dobbins”
Click on podcast image
Search for Sound Bites podcast in iTunes
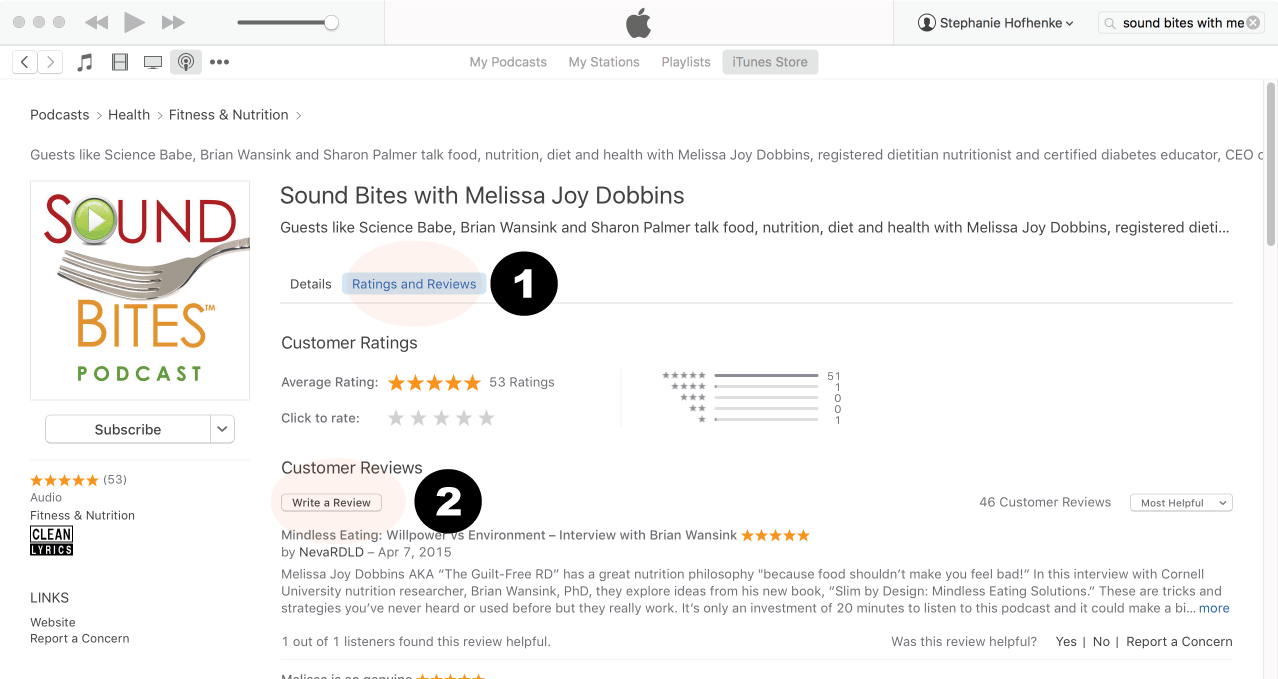
Click Ratings & Reivews
Click Write a Review
View reviews and write your own review.
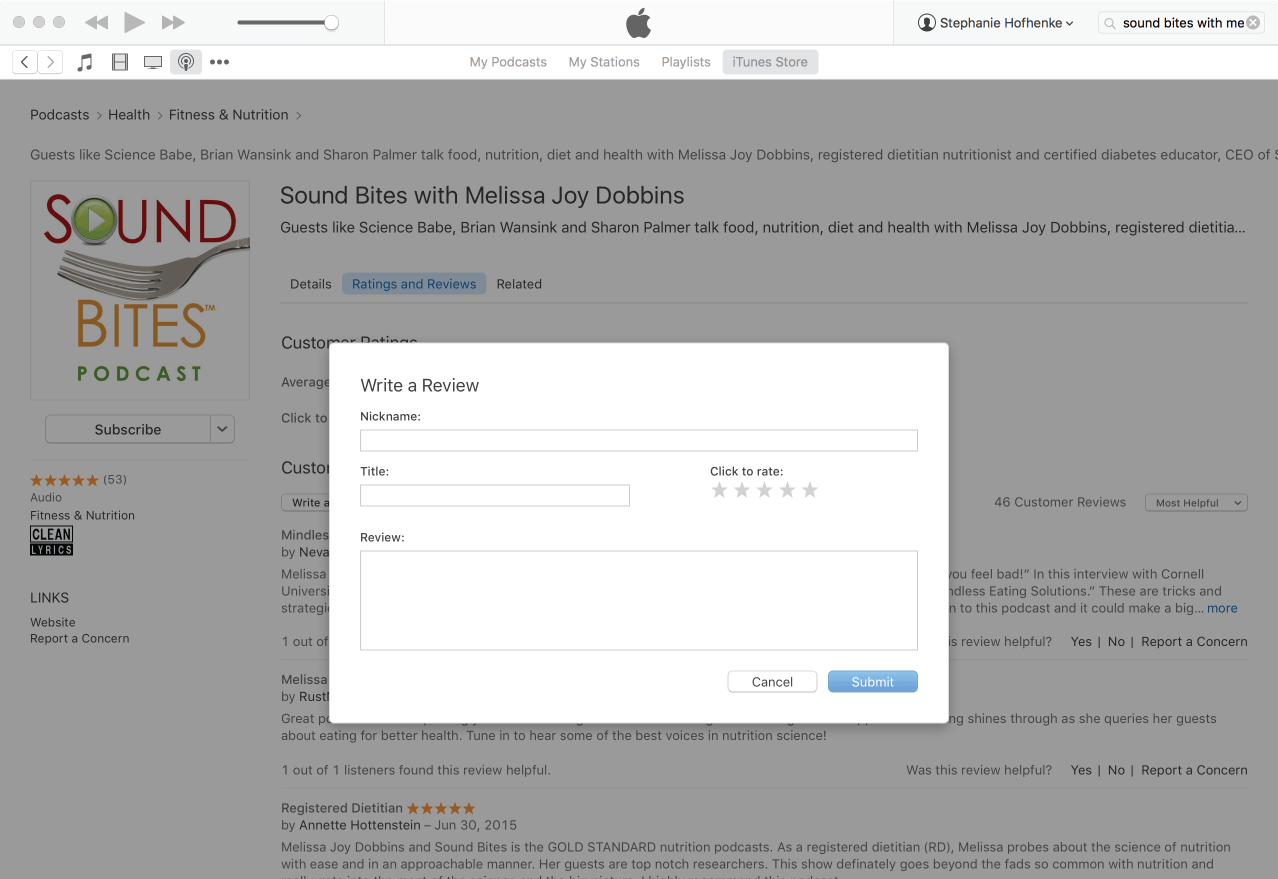
Write your review…. Thank you!
Write your review!
How to subscribe via iTunes
Click here to view the Sound Bites Podcastin iTunes, then click the blue “View in iTunes” button. This will open your iTunes application directly to Sound Bites Podcast. Click the “Subscribe” button, and your done!
 Dr. James Hill is one of the world’s foremost experts in obesity and weight management. He is Professor of Nutrition Sciences and Director of the Nutrition Obesity Research Center (NORC) at the University of Alabama at Birmingham. Dr. Hill has published more than 700 scientific articles and book chapters. Many of these focus on the importance of healthy eating and physical activity in weight management and in preventing and managing chronic diseases. He has been continuously funded from NIH since 1981 and in 1998 received a prestigious MERIT Award from NIH. He is the recipient of several ASN awards, including the Centrum Center Science Award, the McCollum Award, and the David Kritchevsky Career Achievement Award in Nutrition. He has received the TOPS award and the George Bray Founder’s Award from The Obesity Society. He was the 2012 Atwater Lecturer for the US Department of Agriculture. Dr. Hill was elected to the National Academy of Medicine in 2014. Dr. Hill is a cofounder of the National Weight Control Registry, a registry of individuals who have been successful in maintenance of a reduced body weight. He recently launched the International Weight Control Registry to further investigate factors that contribute to successful weight loss management. He has a passion for translating research to address public health issues. He is co-founder of America on the Move, a national weight gain prevention initiative that aims to inspire Americans to make small changes to prevent weight gain. He is the author of the Step Diet Book, published in June 2004 and the State of Slim published in August 2013. He is co-host of a podcast entitled “Weight Loss and….”.
Dr. James Hill is one of the world’s foremost experts in obesity and weight management. He is Professor of Nutrition Sciences and Director of the Nutrition Obesity Research Center (NORC) at the University of Alabama at Birmingham. Dr. Hill has published more than 700 scientific articles and book chapters. Many of these focus on the importance of healthy eating and physical activity in weight management and in preventing and managing chronic diseases. He has been continuously funded from NIH since 1981 and in 1998 received a prestigious MERIT Award from NIH. He is the recipient of several ASN awards, including the Centrum Center Science Award, the McCollum Award, and the David Kritchevsky Career Achievement Award in Nutrition. He has received the TOPS award and the George Bray Founder’s Award from The Obesity Society. He was the 2012 Atwater Lecturer for the US Department of Agriculture. Dr. Hill was elected to the National Academy of Medicine in 2014. Dr. Hill is a cofounder of the National Weight Control Registry, a registry of individuals who have been successful in maintenance of a reduced body weight. He recently launched the International Weight Control Registry to further investigate factors that contribute to successful weight loss management. He has a passion for translating research to address public health issues. He is co-founder of America on the Move, a national weight gain prevention initiative that aims to inspire Americans to make small changes to prevent weight gain. He is the author of the Step Diet Book, published in June 2004 and the State of Slim published in August 2013. He is co-host of a podcast entitled “Weight Loss and….”.