Celebrating over 1 Million Downloads and 50,000 Free CEUs on the Sound Bites® Podcast | NEW: Get 1 years’ worth of CEUs with the new 15-CEU Podcast Course
Click here to earn 1.0 FREE CEU for listening to this podcast episode! GLP-1 Meds and Then What? Turning Weight Loss into Lifelong Wellness – Dr. Gitanjali Srivastava awards 1.0 CPEUs in accordance with the Commission on Dietetic Registration’s CPEU Prior Approval Program.
Disclosure: This episode is sponsored. Commercial support has been provided by Danone North America & OIKOS. Dr. Gitanjali Srivastava is a paid consultant to Danone North America. No brands are discussed or promoted.
Enhancing Success with GLP-1 Medications: Considerations & Strategies
This episode explores strategies for maintaining weight loss and overall wellness following the use of GLP-1 medications. Listeners will learn how behavioral, nutritional and clinical approaches can help patients sustain progress and build long-term healthy habits with shifts to their dosage or after discontinuing treatment.
When you lose weight, you lose percent body fat, but you’re also losing a certain muscle mass. And the people who are able to maintain exercise and healthy eating habits long-term are the ones that are able to preserve their weight maintenance longer.” – Dr. Gitanjali Srivastava
Tune into this episode to learn about:
the STEP and SURMOUNT 4 trial findings
the chronic pathological state of obesity
how GLP-1 meds curb food noise and disordered eating
how GLP-1 meds are intended to be used for weight loss
the crucial role of behavior change
statistics about how and why people plan to stay on or go off the meds
key behavior changes that GLP-1 users can adopt to maximize their success
the importance of structured exercise
how “clock genes” play a role in metabolic function
the power of fiber, protein and fluids in dietary habits
the three pillars: protein, portions and patterns
various reasons that people stop taking GLP-1s
what happens when people stop taking GLP-1s
stigma and bias with weight loss medications
the many challenges in maintaining weight loss
how dietitians are an essential part of the care team
the importance of communicating with patients about side effects
how to support patients who are pausing, cycling or microdosing their GLP-1s
resources for health professionals and the public
The role of muscle physiology and function – it feeds into the energy regulatory pathway. Once you are able to achieve the [weight loss] goal and structured exercise, whether it’s dancing, hobbies, or any type of activity, you’re going to maintain your weight longer.” – Dr. Gitanjali Srivastava
Gitanjali Srivastava, MD, FAAP, FACP
Dr. Gitanjali Srivastava is a Professor of Medicine at Vanderbilt University Medical Center, where she leads the Obesity Medicine program and founded the Obesity Medicine Fellowship. A board-certified internist, pediatrician, and obesity medicine specialist, she is a national leader in advancing obesity care and education. Her research explores obesity pharmacotherapy and includes work on the landmark SURMOUNT-3 clinical trial.
GLP-1 medications are resetting the energy regulatory pathways in the brain. There’s less food noise. The patient is going to be full longer. There’s going to be increased satiety. There’s going to be less disordered eating and snacking behaviors.” – Dr. Gitanjali Srivastava
Resources
Some links may be affiliate links. As an Amazon Associate, I earn from qualifying purchases.
One of the most important things is having access to dietary recommendations, services by a nutritionist or dietitian. Those are key resources and personnel in terms of the ‘journey’ – and being an accomplice along this journey is very crucial.” – Dr. Gitanjali Srivastava
Anderer S. Tirzepatide Outperforms Semaglutide in Head-to-Head Obesity Trial. JAMA. 2025;334(2):107–108. doi:10.1001/jama.2025.7798
Aronne LJ, Sattar N, Horn DB, et al. Continued Treatment With Tirzepatide for Maintenance of Weight Reduction in Adults With Obesity: The SURMOUNT-4 Randomized Clinical Trial. JAMA. 2024;331(1):38–48. doi:10.1001/jama.2023.24945
Haines MS, et al “Muscle loss with weight loss is modulated by age, sex, and protein intake and may affect glucose homeostasis in adults with obesity” ENDO 2025; OR09-08.
Mozaffarian D, Agarwal M, Aggarwal M, et al. Nutritional priorities to support GLP-1 therapy for obesity: a joint advisory from the American College of Lifestyle Medicine, the American Society for Nutrition, the Obesity Medicine Association, and The Obesity Society. Am J Clin Nutr. 2025;122(1):344-367. doi:10.1016/j.ajcnut.2025.04.023
Morgan-Bathke M, Baxter SD, Halliday TM, et al. Weight management interventions provided by a dietitian for adults with overweight or obesity: an Evidence Analysis Center systematic review and meta-analysis. Journal of the Academy of Nutrition and Dietetics. 2023;123(11):1621-1661.e25. doi:10.1016/j.jand.2022.03.014
Rubino, D., Abrahamsson, N., Davies, M., Hesse, D., Greenway, F. L., Jensen, C., Lingvay, I., Mosenzon, O., Rosenstock, J., Rubio, M. A., Rudofsky, G., Tadayon, S., Wadden, T. A., Dicker, D., & STEP 4 Investigators (2021). Effect of Continued Weekly Subcutaneous Semaglutide vs Placebo on Weight Loss Maintenance in Adults With Overweight or Obesity: The STEP 4 Randomized Clinical Trial. JAMA, 325(14), 1414–1425. https://doi.org/10.1001/jama.2021.3224
Spreckley, M., de Lange, J., Seidell, J., & Halberstadt, J. (2023). Primary care-led weight-management intervention: qualitative insights into patient experiences at two-year follow-up. International Journal of Qualitative Studies on Health and Well-Being, 18(1). https://doi.org/10.1080/17482631.2023.2276576
Trinh H, Donovan A, McAdam-Marx C. Real-world effectiveness of tirzepatide versus semaglutide for weight loss in overweight or obese patients in an ambulatory care setting. Diabetes Obes Metab. 2025; 27(6): 3523-3525. doi:10.1111/dom.16343
Speakers: Melissa Joy Dobbins & Dr. Gitanjali Srivastava
[Music Playing]
Voiceover (00:01):
Welcome to Sound Bites, hosted by registered dietitian nutritionist, Melissa Joy Dobbins. Let’s delve into the science, the psychology, and the strategies behind good food and nutrition.
Melissa Joy (00:22):
Hello, and welcome to the Sound Bites Podcast. I’m your host, Melissa Joy Dobbins, a registered dietitian nutritionist, and a certified diabetes care and education specialist.
We’re coming to you live from the expo hall floor at the 2025 Food and Nutrition Conference & Expo, the annual meeting of the Academy of Nutrition and Dietetics, and the world’s largest gathering of food and nutrition professionals.
This episode is part of a special four-part series from Danone North America. Today’s episode is brought to you by OIKOS.
Throughout the series, I’ll be sitting down with experts to explore the latest science and practical strategies that help people of all ages eat well and feel well. And because we’re recording live here at FNCE, we’ll also be taking questions from the audience. So, be sure to stick around until the end of each episode to hear these questions answered by our guests.
Also, this episode has been approved by the Commission on Dietetic Registration for one CPEU for registered dietitian nutritionists.
Today’s episode focuses on weight management in the era of GLP-1 medications. Many GLP-1 users plan to stop taking the medications once they reach their goal weight. But research shows that maintaining weight loss is not easy.
To explore the challenges of weight loss maintenance with the use of GLP-1 drugs, I’m joined by Dr. Gitanjali Srivastava, Professor of Medicine at Vanderbilt University Medical Center, where she also serves as the medical Director of Obesity Medicine, and Program Director of the Obesity Medicine Scholars Program, and founder of the Obesity Medicine Fellowship.
Dr. Srivastava is a board-certified internist, pediatrician, and obesity medicine specialist. She has helped shape national standards of care in obesity treatment and serves in leadership roles with the Obesity Medicine Fellowship Council and Tennessee’s Chronic Weight Management task force. Her research focuses on obesity pharmacotherapy, including clinical trials of anti-obesity medications. She was co-investigator on the landmark SURMOUNT-3 trial.
Dr. Srivastava and I are both paid consultants to Danone North America to share the science and support for yogurt’s role in a healthy eating pattern. Commercial support for this series has been provided by Danone North America.
Dr. Srivastava, welcome to the podcast.
Gitanjali Srivastava (02:54):
Thank you so much for having me today. It’s a pleasure.
Melissa Joy (02:57):
I’m so excited to be here in Nashville, your city, if you will. Now, I’ve talked about weight management and specifically, weight loss medications several times on the Sound Bites Podcast. So, for our listeners, I encourage you to check out the show notes at soundbitesrd.com if you would like to revisit those episodes.
But we’re going to begin today by diving into some of the clinical research and Dr. Srivastava’s experience with patients taking these medications. And Dr. Srivastava, how would you like me to address you moving forward in the conversation?
Gitanjali Srivastava (03:31):
Sure Melissa, you can call me Gitanjali.
Melissa Joy (03:34):
Okay, great. Thank you.
Gitanjali Srivastava (03:36):
To begin with, I just wanted to reiterate that obesity is a chronic disease, and the etiology is complicated. We have genetic, biological, physiological, behavioral, nutritional, environmental factors that contribute to obesity.
In regards to your question about weight maintenance, I think it’s important to clarify with the listeners what exactly is weight maintenance, because I don’t think we truly know what exactly is maintenance, and what is the aftermath.
So, when we take a look at a lot of these medications and what’s expected, so for instance, when you actually have a chronic disease and you treat the disease, let’s take high blood pressure, for example.
Let’s say someone comes in with high blood pressure, you treat the high blood pressure, let’s say follow a DASH diet, maybe the blood pressure comes down, but the blood pressure continues to be elevated, and that patient comes back to the doctor’s office and the doctor says, “You need to start an antihypertensive medication,” then the patient comes back and the blood pressure is controlled.
Well, the blood pressure medication is continued indefinitely in the lifespan of the patient. And the patient knows as soon as you stop the medication, what happens? That the blood pressure goes back up to its natural state. And I think we always have to remember that obesity is a disease, and it’s the same concept.
So, for instance, if we have a disease state, our natural reversion is going to be that chronic pathological state. So, once you bring in a treatment, and that treatment could be lifestyle intervention, it could be dietary intervention, it could be behavioral modification that can be beneficial for some patients. And now, we are in a new era, there’s pharmacotherapy like the GLP-1 drugs.
So, you start that medication, but once you stop the medication, your body is going to want to go back to its natural pathological state, because it’s diseased and there is a systematic inflammation, meta inflammation. And this is different compared to someone who is lean. So, we’re talking about persons that are adversely affected with obesity in the disease process.
So, in terms of weight maintenance, I think that there’s different definitions for weight maintenance. We don’t know what treat to target is. So, let’s give certain scenarios.
For instance, let’s say that you have a patient who comes in and has achieved his or her weight loss goals, has come in from a body mass index from class three to class two obesity and is doing much, much better, and is controlled with lifestyle and nutrition and maybe the medication. Will that patient regain the weight if the drug is discontinued? The answer would be yes, because the disease state is still present, even though it’s better controlled. I mean, the disease state is still there. It’s always going to be there.
Now another scenario is what if a patient starts with a class three body mass index? You start a medication, and the patient does really, really well, and all of a sudden, the body mass index is less than 30 or less than 25. What do you do with that patient?
And I think we don’t know what the treatment to target is, but we do know that even if the patient has approached a body mass index of 24, if I were to ask you the question, does this patient still have obesity? The answer is yes. The patient still has obesity because the susceptibility is there, the disease process is there. Now, it could be controlled with medication, or it could be in remission without medications. So, I think those definitions are very variable.
Now, the patient who’s able to reach a lower body mass index less than 30, or let’s say less than 25, may be able to better control and maintain the weight, if he or she follows dietary recommendations or works really closely with a dietitian and has structured exercise, maybe the weight maintenance would be persisting longer compared to an individual who does not engage in those practices.
Melissa Joy (07:46):
Gitanjali, you mentioned pathological state. Could you explain that further for our listeners and myself (laughs).
Gitanjali Srivastava (07:52):
Yes. So, the pathological state of obesity refers to all of the food noise when we look at the brain gut axis. So, the brain has what we consider a settling point in the hypothalamus, in the arcuate nucleus, and it plays a yin yang relationship because there’s hunger neurons and there’s satiety neurons.
And so, when we have, let’s say food that goes down our GI tract and it hits, let’s say, the duodenum in the stomach, there’s all of these hormones that are released that go up and tell the brain how we should feel, whether we should feel hungry, or whether we should have cravings, or whether we should feel full and satiety.
So, with the GLP-1 drugs, what happens is that they curb down that food noise. It’s like decluttering that gut brain axis. And they’re slowing that digestion, they’re delaying the stomach emptying as we speak.
And so, they also disrupt sort of that dysregulation that happens. And so, they’re resetting the energy regulatory pathways in the brain, so there’s less food noise. The patient is going to be full longer. There’s going to be increased satiety. There’s going to be less disordered eating and snacking behaviors. We also know that there is a likely decreased inflammation that happens overall in the body, or reduction in meta inflammation in the body.
So, there’s all these benefits to the treatment of that pathobiology or what we consider that pathological state compared to someone who’s lean. Let’s say when you have someone who’s lean, who actually let’s say goes to a buffet for an example and they overeat, the next day, he or she’s able to reset the metabolism without even thinking about it. That patient may be less hungry, they may feel like more energy, they may be tempted to run outside and burn off those calories. There’s all of these innate mechanisms.
But the person who has obesity, let’s say if you go to a buffet comparatively speaking, that person doesn’t have those processes necessarily working efficiently in his or her favor. And that’s where the GLP-1 drugs come in and they can actually reduce that pathology and help treat the patient.
Melissa Joy (10:17):
And one of the things that I think is so fascinating about that is that now the world knows that people have that, and it’s not just in their head and it’s not a willpower issue, that it’s pathophysiology.
Okay, great. Thank you. Both the STEP and SURMOUNT-4 trials showed that even with nutrition counseling and activity, weight regain is common when people stop taking a GLP-1 medication for obesity treatment, which makes sense as you’ve described.
Can you share a bit about those trial findings and what they mean for people who are using GLP-1s now or in the future, and the clinicians who work with them.
Gitanjali Srivastava (11:01):
Sure. I think the STEP trials and the SURMOUNT trials, we can definitely talk about. The STEP trials were associated with semaglutide, and we see that very clearly in the STEP-4 clinical trial where the clinical trial participants actually were prescribed semaglutide 2.4 milligrams. But once you stop the semaglutide 2.4 milligrams, the patients have actually a rebound and they regained the weight back, compared to the patients that were continued on the semaglutide.
And the question is, when the trial came out, people were very intrigued by that. But as an obesity medicine specialist, we know that that’s what the body is going to do, is the physiological response in that scenario. And we see that also in the SURMOUNT-4 clinical trial where the patients were actually exposed to the tirzepatide, and then later on, characterized into the placebo versus continuing the medication.
So, the patients who continued the medications continued to lose weight, but the patients who were transitioned from the drug to the placebo arm continued to regain the weight back.
And the same thing in the SURMOUNT-3 clinical trial, which was a little bit different. The patients actually underwent intensive lifestyle modification first before starting the medication. And it shows that even with the lifestyle modifications and after adding on the GLP-1 drug, that patients continue to lose weight. So, there can be some either additive effect or in combination with lifestyle modification as well in those clinical trials.
Melissa Joy (12:34):
Okay, thank you. Yeah, the STEP and SURMOUNT trials support the effectiveness of semaglutide and tirzepatide in treating obesity. I’d like to learn a little bit more from you about how GLP-1 users can optimize that weight loss journey, especially if they aren’t staying on the medications long term. There’s a variety of reasons that people may not stay on the medication, which we can get into. And I have some consumer insights to share as well.
From a clinician standpoint, how are GLP-1 medications intended to be used for weight loss?
Gitanjali Srivastava (13:09):
Sure. That’s a great question. First of all, the medications are prescribed for any patient that has a BMI greater than 27 plus or minus a complication when we’re thinking about a weight related complication, and then a BMI greater than 30.
And so, when you think about it, that’s the majority of US adults and Americans that have the disease process. These medications are intended to be chronic long-term for weight management. So, that means that you should not be discontinuing the medication once you start the medication.
Now, we have a little bit of questions around the potency. Now, that we’re getting into a new era of obesity medicine where these medications are able to surpass more than 20% weight loss, some patients are now able to reach their goals and some patients are now having a BMI of less than 24.
So, we have less research data and insights, although a lot of research papers are in development in clinical trials that are evaluating the weight maintenance phase. But it leads to very interesting questions around body composition, muscle mass structured exercise, the importance of protein and fiber, and just really healthy nutrition for the weight maintenance phase.
Melissa Joy (14:25):
Yes. So, according to some consumer research that I’ve seen, 26% of GLP-1 users do not intend to stop using it. And 46% say they plan to quit in less than 12 months, while 29% will quit if they experience a negative outcome or side effect. And 46% will stop when their health goal is achieved. What’s your take on all of these variety of reasons?
Gitanjali Srivastava (14:56):
Absolutely. This data is very consistent with what we are seeing in the real-world pragmatic clinical data setting, and that’s what we see. There’s a higher discontinuity among users of GLP-1s, and it’s for various reasons. Part of it is also insurance, cash pay options, and sustainability of the drug coverage and formulary changes that we’ve seen over the past year, especially back and forth on that. So, a lot of that has to do with the cost and affordability of the medication.
But if you move that aside, a certain portion of the medications can experience side effects and those side effects, if they tend to be lingering or persistent, tend to be more adversarial for the patients. And those patients may discontinue and consider other options. But a large majority of patients do not want to be on these medications long-term.
I mean, that’s the one question that I get often from my patients like, “Dr. S, how long do I need to be on these medications?” And my answer typically is, “You have to be on these medications long term. This is a chronic disease.” And it’s going back to again, reemphasizing and reiterating over and over again their chronicity of obesity as a disease process, very much like how we have high blood pressure and type 2 diabetes and even asthma. There can be flare ups and things like that.
So, I think it’s helping the patient understand their journey, that they’re in it for the long haul, and we have to help them with all the tools and the armature that we have necessary to proceed forward and be successful in this journey.
Melissa Joy (16:30):
Yes. The cost and accessibility factors, that’s the reality. But a big portion of it is people just going into this journey assuming that they don’t need to stay on forever. So, those are kind of two different things.
Gitanjali Srivastava (16:45):
Yeah, very two different things. And so, I think that’s where the education comes in too. So, cost considerations and barriers aside, I think from the statistics that you had quoted from the consumers that we are hearing, is that many people still believe that, okay, it’s a quick fix. It’s short-term or temporary that they’ll take it for maybe a year and just see how their body does.
And oftentimes, we’ll see those patients come back with significant amount of weight rebound and regain, and it’s the return of hunger and cravings and disordered eating that was previously treating the pathology that the patients are now experiencing off the GLP-1 drug.
Melissa Joy (17:27):
And I know we’re going to get into some of those nuances about preparing the patient, going in with the proper mindset of here’s the ideal situation, the medication works while you’re taking it, it stops working when you stop taking it. From your perspective, what are the key behavior changes that GLP-1 users should adopt to maximize their success on this medication?
Gitanjali Srivastava (17:51):
Sure. So, I think one of the most important things is having access to dietary recommendations or services close by nutritionist or dietitian or someone within the network because those are key resource and personnel in terms of the journey and being like an accomplice along this journey is very crucial.
Oftentimes a professional dietitian can actually zone in on meal planning and creative ideas. Sometimes we have patients that travel, and they didn’t think about, let’s say the baby food L section as a certain pouches that they can carry or throw in the travel bag, for example.
So, there’s a lot of creativity and ingenuity when it comes to customizing meal planning and recommendations. So, if a person has access to one and certainly there’s virtual, there’s online, they can get a referral from primary care physician.
The other thing to complement that is structured exercise, I cannot emphasize that enough. And a structured exercise is what you’re able to do in the capacity of your moment in your current time. I know that we are very busy professionals and working, sometimes there’s like 10-hour, 20-hour jobs that people are doing. Sometimes people are working two jobs to make ends meet. And that is really tough.
But as long as you can be active or keep up with your activity steps and let’s say 10,000 steps per day as a goal. And it’s not about going to the gym necessarily, but it’s about being structured and consistent and persistent. So, if all you can do is 10 minutes of walking in the morning and 10 minutes after work, that’s better than nothing, but you have to maintain that and be structured.
And this is becoming very important and much more crucial as we get into the weight maintenance phase. Because this is where when you lose weight, you lose percent body fat, but you’re also losing a certain muscle mass. And the people and the patients that are able to maintain exercise and healthy eating habits long-term are the ones that are able to preserve their weight maintenance longer, and be able to sustain and just be, I think, just be overall well compared to those who are not engaged in those practices.
Melissa Joy (20:01):
Yes, I’ve heard this a lot that, I mean, exercise is important for a variety of reasons, but with that weight loss maintenance phase, it’s really crucial.
Gitanjali Srivastava (20:11):
Yes, so crucial. So, another aspect of exercise that I wanted to add is the role of actually muscle physiology and function. So, why is it important to exercise?
Sometimes patients will come in and say, “Well, I don’t really care about the muscle mass, I care about the total weight that’s lost.” And so, the reason that that’s important to look at the complete picture is that if you have preserved muscle or you’re able to maintain a muscle, that means that muscle is going to burn.
We think about burning energy and energy expenditure, and that your resting metabolic rate is going to be higher and so your metabolism is going to be more efficient in burning off that extra weight. And that’s where weight maintenance comes into effect. And that’s why I’ve spoken at it several times of the importance.
It’s like putting your money in the savings bank. It comes in so much handy at a later time. But when you have reached your goals and let’s say you are very happy where you’re going, someone who has not exercised compared to someone who has exercised is going to actually regain the weight significantly faster compared to someone who is able to exercise. And there has been studies that have evaluated and looked at that.
So, coming into the role of muscle physiology and function, it feeds onto that energy regulatory pathways. Once you are able to achieve the goal and that structured and exercise, whether it’s some dancing or hobbies or any type of activity just to keep yourself active, you’re going to just maintain your weight longer.
Melissa Joy (21:54):
And when you say structured, is this like it’s on my calendar, I’ve blocked out the time, or is this more formal exercise?
Gitanjali Srivastava (22:01):
Either one. Any exercise is better than no exercise, but yes, it can be. And for persons that are very busy, I actually tell them, put it on your calendar because if it’s on your Outlook calendar or Apple calendar, it’s in your site because when it’s out of sight, it’s out of mind and it’s not going to happen. And your time is going to be easily consumed with other activities.
And I think in the United States, when we look at how productive and a capitalistic society we are, we are always like energizer bunnies, always on the go, go, go. And we never have time to take care of ourselves. And you really need to put thought and insight into self-care and nourishment. And that’s why if it goes on your calendar, it’s great.
I personally do it all the time. Call it whatever you want, a wellness meeting, a productivity meeting, a one-to-one, but you are going to be more energized coming to your meetings if it’s blocked out in your calendar. If you can only do it 15 minutes, 20 minutes, that’s great. If you can do 30 minutes that’s even great, but pencil it into your calendar and I think that will actually help maintain that consistency and structure.
Melissa Joy (23:05):
Yes, very good. When in the weight loss journey should people begin thinking about these behavior changes?
Gitanjali Srivastava (23:12):
It’s never too late and it’s never too early (laughs) as soon as possible. So, if you are listening to this and if you have patients that are not engaged in these types of behaviors, encourage them to do it now. It’s never too early and it’s never too late, as soon as possible, but the sooner the better.
Melissa Joy (23:31):
You talked a little bit about physical activity and that structured activity, and we can talk about dietary changes as well, but I understand you are very passionate about sleep and the role of sleep, so I’d love to hear your take on that.
Gitanjali Srivastava (23:46):
So, sleep is equally very important, as we’ve discovered over time that we have these clock genes and when you get disturbance in these clock genes, it can actually cause a lot of metabolic derangement and complications later on.
And we see this in night shift workers too. People, especially nurses that are working the night shifts, you see a lot more disordered eating and sometimes, it’s like you’re working four days on, two days off or seven days on, seven days off. And it really messes with the metabolism and how we perceive that.
Equally important too, is also assessment for that reason for sleep apnea. So, for instance, when we gain weight, it’s not just the waist circumference that is gaining weight over time, but there can be deposition of fat at the base of the tongue that can actually lead to obstructive sleep apnea and other complications.
Sometimes with the treatment of sleep apnea, I’ve seen patients lose 20 or 30 pounds just by treatment of it or by actually having consistency and structure in our sleep. And sleep hygiene is so important too, especially if you think about our bedtime routines, we are distracted by iPhone and devices and there’s that blue light that is going on into the back of the retina that is disturbing our deep sleep and our REM sleep.
Our deep sleep is the most important part of the restorative process in terms of our metabolism. That’s where the cells kind of repair their energy and all of those processes. And so, if you do not get into the deeper phases of sleep, you will start to feel fatigued and it’s a rise in insulin and resistance and cortisol levels. So, protecting your sleep and having really good sleep hygiene is equally critical to the process.
I think in order to lose weight, it’s not just the nutrition and exercise, you really have to persuade your mind that you are rested, you’re eating healthy, you’re in a good fit in terms of your metabolism and you’re not stressed out.
Melissa Joy (25:48):
Very good. Let’s touch on dietary changes before we move forward to my next question. I talk about diet a lot, obviously on the podcast with weight loss and weight loss maintenance. But what behavior changes with regard to diet would you like to share with us for these particular patients?
Gitanjali Srivastava (26:04):
I think choosing foods that support fullness like fiber and protein and fluids and minimizing nutrient poor and highly processed like sugars and high fat and fried foods, it’s important. You want to limit alcohol and sugar sweetened beverages.
I think the main takeaway from here is that the scientific evidence really points towards healthy unprocessed foods. So, the more that we can eat the fresh fruits and vegetables and natural foods, the better it is in terms of a health perspective.
Melissa Joy (26:37):
Yeah, and I know that can be very confusing topic for patients; processed foods, ultra processed foods, is it in a box, a can, whatever. So, I like to encourage people to look at how much nutrition are you getting from that product. And sometimes that can help clear up some of the confusion as well.
Yeah, so for patients who do have to come off the medication, let’s talk about some of the considerations that the patients themselves and the practitioners as well should prepare for. For example, if a patient is stopping a GLP-1, what kind of changes do they typically notice physiologically and behaviorally?
Gitanjali Srivastava (27:15):
So, I think one of the things is that return of hunger and cravings before when-
Melissa Joy (27:22):
The food noise.
Gitanjali Srivastava (27:23):
Yeah, the food noise, it’s that sort of that subtle food noise that’s cluttering up our processes and that’s what we frequently hear as well. Once you stop the GLP-1, there’s no longer that delayed gastric emptying.
So, that food was staying in the stomach longer and feeling of satiety, so that feeling of satiety is diminishing. So, the hunger patterns are going to be returned, the patient’s going to be more hungry. And then we also see return of snacking and disordered eating patterns and return of intensity behaviors. That return of food noise all the time.
I think that is very consistent. And so, when patients start to notice those things coming back again, they may not be equipped to fully address it. And this is where mindful eating and mindfulness and those practices while they were on the GLP-1 medication is very beneficial, and physiologically that makes sense too.
But patients often say, “I feel like I’m thinking about food all the time.” And it’s that obsession with the food that returns for majority of those patients.
Melissa Joy (28:30):
Yes, all good points. So, from your clinical perspective, we know that maintaining weight loss is difficult, but what do you think is most difficult to navigate, and how do you help patients stay motivated during that time?
Gitanjali Srivastava (28:45):
Sure. I think the most difficult aspect of the journey, and this is after coming off a GLP-1 drug, is the discouragement and the disappointment that the patients face, and the patients come back and feel like it’s their fault again.
And I want to emphasize that it’s never the patient’s fault that there’s a return of hunger and patterns. And I have to explain and constantly remind the patient, it’s the pathophysiology in the bodies, the disease process in the body that is leading the patient to feel that way.
And so, there’s other ways that we can do that. And if for some reason … I like to explore the reasons for discontinuing the GLP-1 drug, that’s equally important to investigate. If it was for insurance reasons or considerations, there are other generic alternatives that we can consider.
If it’s for side effects, there’s still other alternatives to consider that can actually help curve the appetite curve, curve the hunger that is returning back and we can actually guide the patient in that journey.
Melissa Joy (29:49):
And I assume that if you can manage some of those side effects, then maybe they won’t need to go off with the medication, right?
Gitanjali Srivastava (29:57):
Correct. You’re absolutely right. Sometimes depending on the side effects, and most of those side effects are GI related. We can use Tums, we can use Protonix over the counter, there’s anti-emetics to help with the nausea. There’s different ways of spacing out the injection from seven days to seven to 10 days and alternating the site of the injections that we can all do. And that takes care of 90% of the side effects that majority of the patients experience.
It’s important to note that dietitians are really important in helping with the timing, let’s say, of the food and the type of food. Sometimes patients can be having side effects. Let’s say for example, their blood glucose is much better controlled and they’re having nausea because they’re skipping out on meals or not eating. And that’s oftentimes picked up by a dietitian. And sometimes during the office visit for the provider, the patient may not reveal that he or she may be skipping meals. And that’s important.
Other side effects aspects is sometimes the nausea, and let’s say it’s the GI adverse profile, can be alleviated by the type of food. So, for instance, if patients come in with constipation, there are certain fiber rich foods that the patients can tolerate beyond let’s say green leafy vegetables that patients would really benefit from.
So, in terms of the timing and the type of food, the dietitians can really help mitigate the side effects that are associated with some of these GLP-1 drugs.
Melissa Joy (31:23):
Oh, that’s really good to hear. So, you mentioned the high blood pressure medication, or the hypertension medication and how people, they go on that they kind of don’t expect to go off of it. I see this a lot as a dietitian and a diabetes educator, I feel like there’s just more stigma associated with weight related medications. Even like with diabetes, I feel like maybe there’s shame or blame feelings like well, I need to get off of this medication because it’s my fault that I’m requiring it versus blood pressure. Have you seen that as well?
Gitanjali Srivastava (31:59):
Oh yes. I even see this as a social context too. One time I was in social gathering, and one of my close friends, another friend commented, “Oh, did you lose weight? Was it with a drug or did you do it by yourself?” So, it’s that stigma and it’s their bias, because when you think of other diseases like high blood pressure and diabetes, there’s no outward appearance that I could pick out.
For example, if you put 10 persons in front of me and asked me who has high blood pressure and type 2 diabetes, I could not possibly guess. Maybe I could pick out some cues like acanthosis or something like that on exam, but it would be really impossible to kind of point out who has. But if I were to pick out of those 10 persons like who has obesity, all of a sudden, it’s a different context.
So, I think that we have in current, in 2025, we have come a very long way from where we were in 2010 and 2013 to battling bias and stigma, but it’s still a fight that we do all the time and education all the time to patients telling them it’s not his or her fault, it’s a biology, it’s genetics and relaying that messages throughout.
And so, sometimes that message can come from me, it can come from dietitians, it can come from the behavioral health experts, but if all team members relay the same message, we’re working in it together to fight bias and stigma, which is so critical to the success and the transition of our patients.
Melissa Joy (33:29):
And that’s so important because again, like this whole conversation of like what to expect, how to manage these side effects to increase the success of the patient staying on and knowing that okay, this is a long-term solution and a long-term journey, so then they might have less disappointment or discouragement as they’re managing this whole process and having these conversations with dietitians and physicians and other healthcare providers.
Gitanjali Srivastava (33:57):
Absolutely. So, oftentimes our patients not only see me, but they work very closely with their dietitian because the dietitian they pick up on the fact that hey, this patient is having a little bit of nausea, can you call in an anti-emetic? Or it’s definitely a collaborative atmosphere that we have.
And so, we’re part of the team, and I think having a team effort approach is definitely the key to managing the adverse effects that the patients may experience. But majority of those adverse effects can be managed by symptomatic and supportive care.
Melissa Joy (34:28):
Wow, that’s really good to hear. And the role of the dietitian has shifted in this GLP-1 era. And a lot of dietitians don’t know, like that’s a crucial role that you might be the first person to have the conversation about the side effects and be the conduit to the solution.
Gitanjali Srivastava (34:46):
Yes, I hear that all the time because I sometimes don’t see my patients till like maybe a month, two or three months later, depending on the follow up, especially if we’re doing adjustments and doing well, but they actually may be seeing our dietitian more frequently.
And so, I get messages from our dietitians all the time that this patient is having these side effects, what do you think about this? Or this patient is having an increase in stacking behavior and cravings, is it okay if we increase the dose? I see that the dose hasn’t been up-titrated and it’s been over a month, and the patient may not be aware that they needed to reach out back to our nurses team to increase the dosage of the medication. So, it’s team effort.
Melissa Joy (35:24):
It all comes down to communication, doesn’t it?
Gitanjali Srivastava (35:26):
Yes (laughs).
Melissa Joy (35:27)
So, for patients who know they’re going to be coming off of the medication for whatever reason, what can they start doing ahead of time to prepare for this transition and be successful?
Gitanjali Srivastava (35:37):
I think that’s a great question. For the patients — and there’s two approaches to this. One of them is the patient who may have reached his or her weight loss goal, but maybe coming off the medication, maybe due to insurance consideration.
So, I think the first thing is having a very good report with the provider, having a follow-up and a transition plan, that if he or she’s going to be discontinuing the GLP-1 drug, what other alternatives can we do? And there are options like metformin, phentermine, topiramate, bupropion, all of these other alternatives that the physicians can discuss.
At the same time, he or she should also have a follow-up with the dietitian to look over the meal plan and recommendations for protein and fiber and for consistency across the board in case snacking behavior and issues arise.
And then also, we have a behavioral health professional who’s also in our team that can actually help with a lot of the behavioral modification as well. And then also a plan for exercise and continued exercise support. So, all of those are definitely important part and pieces of the puzzle to really maintain proactively the next steps in the journey.
Melissa Joy (36:45):
Great. So, we’ve talked a little bit about what patients can do to prepare if they have to stop the medication, or perhaps reducing a dose or the frequency with which they take it. But of course, they don’t have to do it alone. And we’ve already talked about the important role of the dietitian, but let’s talk about how dietitians can best guide and empower their patients during this stage.
So, we’ve got dietitians listening in here at FNCE and of course, just listening to the podcast in general. What are some top strategies for helping patients sustain progress either after reaching their weight loss goals or if they’re coming off the medication for a variety of other reasons?
Gitanjali Srivastava (37:23):
Sure. So, I think it goes back to a couple of things. One, I think the focus in terms of lifestyle modification is very critical. And in terms of lifestyle modification, focusing on nutrient dense foods that are high quality foods is so important. Coupling that with behavioral modification strategies like mindful eating versus mindless eating to control that disordered eating or snacking behavior is critical, adding some structural exercise. So, having a very robust plan for a lifestyle modification and sustainability, especially after discontinuation of GLP-1, is going to be important.
And then engaging in the conversation with a provider what next? If you come off a GLP-1 drug and there is expected weight regain that’s going to happen, what are the alternatives that the patient could trial for anti-obesity medications that is a non GLP-1 to continue the journey forward?
I think that will address the majority of the concerns that arise, especially with weight regain that we’re trying to combat. And the patient is constantly fighting against. Because the patient is constantly fighting the biology and genetics and we know we can’t do that. We can’t fight biology; we can’t fight genetics.
We can have control over what we can do. We have control over the types of food that we choose and types of foods that we can put in our mouth. We have control over maybe the amount of exercise, and those are factors that are within our microenvironment. But the macro environmental factors, we have less of a control over.
And so, just like biology and genetics, maybe if it’s really cold outside, we don’t have any control over that, but we have control over wearing a jacket and going outside. So, those are the things that we can focus on.
Melissa Joy (39:09):
Okay, great. You have an approach with three pillars: protein, portions, and patterns. And I would love for you to share that with our listeners.
Gitanjali Srivastava (39:19):
So, in terms of the three pillars that we have is, we have protein. So, we want to encourage patients to anchor meals and snacks around high quality protein sources like Greek yogurt and eggs and legumes, lean meat.
So, protein not only helps preserve lean mass, it also supports satiety, which especially important once the medication is stopped. And yogurt is an especially versatile option because it’s portable. I have non-fat Greek yogurt all the time with lunch. So, it pairs well with fiber rich foods like fruits and nuts and it can be used for both sweet and savory applications.
Then we have portions that work with patients on strategies to right size portions in a way that feels supportive rather than restrictive. So, this may include smaller plates, mindful eating techniques, even practicing pausing mid meal to check in with hunger cues.
And then we have patterns. You want to help patients find an overall healthy pattern they can stick with long term. So, ideally, they’ve started to develop these lifestyle changes like choosing nutrient-dense foods, engaging in physical activity like strength training or mixed training, increasing protein consumption and supportive interventions.
We talked about sleep, stress management, nurturing, positive social connections, all of those are really important when they started on the medication. So, we’re looking at protein, portions and patterns.
Melissa Joy (40:48):
I love that. I’m a fan of alliteration and triplets, so that just checks all the boxes. With so many physicians either getting questions about these medications or supporting patients who may already be taking them, how can we make sure that dietitians are a part of that equation?
Gitanjali Srivastava (41:05):
I think communication is really important and it’s key, and it’s definitely a multidisciplinary team-based approach. I do not think that I could do weight management without my team. It’s not me doing it alone and it’s not the patient doing it alone. It definitely takes a village.
So, I think the education is key and also spreading the word about in terms of the importance of a multidisciplinary approach. And patients can request it too. Sometimes patients are not aware that it’s even an option. Oftentimes, they’ll come to their primary care physician talking about weight management strategies, but if the primary care or the generalist doesn’t bring it up, the patient doesn’t know.
So, communication and education are key aspects of disseminating that information of that multidisciplinary and multifaceted approach, the treatment and management of weight.
Melissa Joy (41:55):
Yeah, I think you’re so right. So many patients just aren’t aware and if the physician doesn’t bring it up, it doesn’t come up. But I do want people to know (I mean, I know a lot of the dietitians listening know, but just in case) that the academy does have a resource called Find A Nutrition Expert on their website at eatright.org, and patients can use that, doctors can use that, dietitians can even use that.
I’ve had people approach me about seeing them one-on-one, and if it’s not my particular expertise, I use that to help them find somebody with the right expertise or in their area who offers virtual counseling. And I believe there’s also stuff in there about insurance. So, I definitely encourage people to check that out.
Gitanjali Srivastava (42:41):
That’s a wonderful resource. And I do use it for our patients and they love it, but I think a large majority of patients may not be aware. And I think spreading the word out to practices that this is available resource would be fantastic.
Melissa Joy (42:54):
Yes, and ideally facilitating the conversation between the dietitian and the primary care provider as well too, because that’s important to close the loop on all of that. So, we’ve covered a lot today, but I would like to take a few questions from our live audience listeners.
The first one is: as dietitians, we often see patients who want to pause their GLP-1 therapy because of the side effects or the cost, but then they hope to restart it later. So, from your perspective as a physician, what should we know about the safety or effectiveness of cycling on and off of these medications?
Gitanjali Srivastava (43:31):
I think this is a very valid and a great question because patients do this all the time. So, it’s known as cycling or microdosing. And so, first of all, the medications are intended to be taken as per label, so there are a once weekly formulation. We are getting into these issues of cycling and microdosing just because there has been confusion in the layman and the medical community. And then there’s the insurance barriers and the cost considerations. And sometimes, patients are having side effects.
I think that we talked a little bit previously about if the patient is having side effects, then spacing out the injection from every 7 days to 7 to 10 days is actually acceptable and recommended and alternating the site of the injection. The question comes into weight maintenance, and I have several patients who are in the weight maintenance space, and we don’t have a lot of research in terms of guidance. So, our example is a patient who now has a BMI of 23.
So, back to that question, does she still have obesity? Yes, she still has obesity, but her obesity is controlled with medications, and she’s on tirzepatide. So, what are we doing for this patient? Well, when we discontinued the tirzepatide and she wanted to try it, she had return of hunger and cravings and anxiety, so she needs something.
So, we tried an alternative but she didn’t have the same response. So, but now she’s back on the tirzepatide, but she’s not requiring the higher doses, the 15 milligrams. She’s on a very low dose, 2.5 to 5 milligrams, that she takes actually every 14 days to maintain her weight and she feels good. She doesn’t have adverse effects.
I think that when we get into the weight maintenance phase, I think this is something that you should do with consultation with your physician, with your provider, and really discuss like the safety and the off-label use and how we should be using some of these medications, especially when you are treated to target and you’re reaching the weight maintenance phase.
But more importantly, this patient is able to maintain a BMI of 23. She started with a BMI greater than 40 of note, but she’s able to maintain that. It’s because she is very vigilant about monitoring her food intake and this is healthy nutrition. We talked about the three Ps. She’s following that and she’s engaging in active structured exercise four to five days per week to maintain that, but she feels happy and healthy doing that.
So, I think that this is where we get into a very shady area of what to do. What’s the next step? And then some patients for another scenario is, let’s say a patient who’s had a great response from the GLP-1 drug has reached from a BMI of let’s say above class three obesity, and now is in class one obesity, but cannot afford the medication due to insurance.
So, these patients are opting to do the cash pay through the manufacturer, but they can be kind of spreading out the medication or taking a microdose of that medication, which is really discouraged, but that’s the only medication that is actually effective that they can do within the costs considerations and the constraints of that patient. So, kind of two extreme examples, but we are seeing that in the real-world setting.
Melissa Joy (46:41):
Okay, great, thank you. The other question is: looking ahead, there’s a lot of buzz about combination therapies and next generation obesity drugs. From your vantage point as a physician and researcher, what should dietitians be aware of as this landscape evolves?
Gitanjali Srivastava (46:58):
Great question. We now have dual agonists like tirzepatide, which we talked about, which is a GIP-1, GIP already approved. And there’s even triple agonists that are now in the late stage of a development such as retatrutide which really target multiple pathways beyond the GLP-1. There’s also other mechanisms of actions that are looking at activin and my statin inhibitors that actually preserve muscle mass in terms … and then combination of those agents with the GLP-1 agonist as well.
So, early data does suggest that these therapies may achieve even more significant reductions in body weight compared to semaglutide alone or tirzepatide alone. And that’s really exciting, but it also means that the after story will remain just as important. No matter how effective the drug is, patients will eventually face transitions.
And so, I think that’s why in this current era, we have more research that is exploring into muscle preservation and role of muscle mass and weight maintenance, and what is the best way to approach weight maintenance because we don’t know, but we are in a new era and that’s what we’re facing now.
Melissa Joy (48:08):
Interesting. Thank you. Well, Gitanjali, thank you so much for joining us today and sharing your expertise. We have covered a lot of ground, and you have helped us see this after story isn’t the end of the journey. It’s really just this next phase.
And one of the biggest takeaways I think, is that medications can be powerful tools to initiate weight loss, but sustaining progress depends on habits, on support and confidence, and that’s where dietitians can really make a difference.
Gitanjali Srivastava (48:42):
Absolutely. So, GLP-1s and other anti-obesity medications are really changing the landscape of weight management, but they’re not a standalone solution. GLP-1 therapy is just one chapter in this lifelong journey.
The real success really happens when patients have a plan for what comes after, and that’s what helps them maintain their health and thrive beyond the medication. And dietitians are absolutely central in guiding and empowering patients through that transition.
Melissa Joy (49:13):
Thank you so much, and thank you to our live audience here at FNCE for being part of this important conversation. This episode is part of a special four-part series brought to you by Danone North America. Be sure to check out the other episodes where we explore child nutrition, gut health, and diabetes risk reduction, each one bringing you new science and practical strategies you can use in your practice.
Thanks again for tuning in and as always, enjoy your food with health in mind. Until next time, I’m Melissa Joy Dobbins and this is the Sound Bites Podcast.
[Music Playing]
Voiceover (49:48):
For more information, visit soundbitesrd.com. This podcast does not provide medical advice. It is for informational purposes only. Please see a registered dietitian for individualized advice.
Music by Dave Birk, produced by JAG in Detroit Podcasts. Copyright, Sound Bites, Inc. All rights reserved.
LISTEN, LEARN AND EARN
Listen to select Sound Bites Podcasts and earn free CEU credits approved by the Commission on Dietetic Registration (CDR) for registered dietitian nutritionists and dietetic technicians, registered. Get started!
Get Melissa’s Sound Science Toolkit here!
Partnerships:
Sound Bites is partnering with the Association of Diabetes Care and Education Specialists (formerly the American Association of Diabetes Educators)! Stay tuned for updates on the podcast, blog and newsletter!
Sound Bites is partnering with the International Food Information Council! Stay tuned for updates on the podcast, blog and newsletter!
Sign up for my monthly newsletter and episode eblasts so you never miss an update!
Listen on Stitcher (Android)
Install the Stitcher App
1. Search for “sound bites with melissa joy dobbins” 2. Choose Play Current Episode or Add to Playlist
Choose “Play Episode”
Subscribe & Review on iPhone
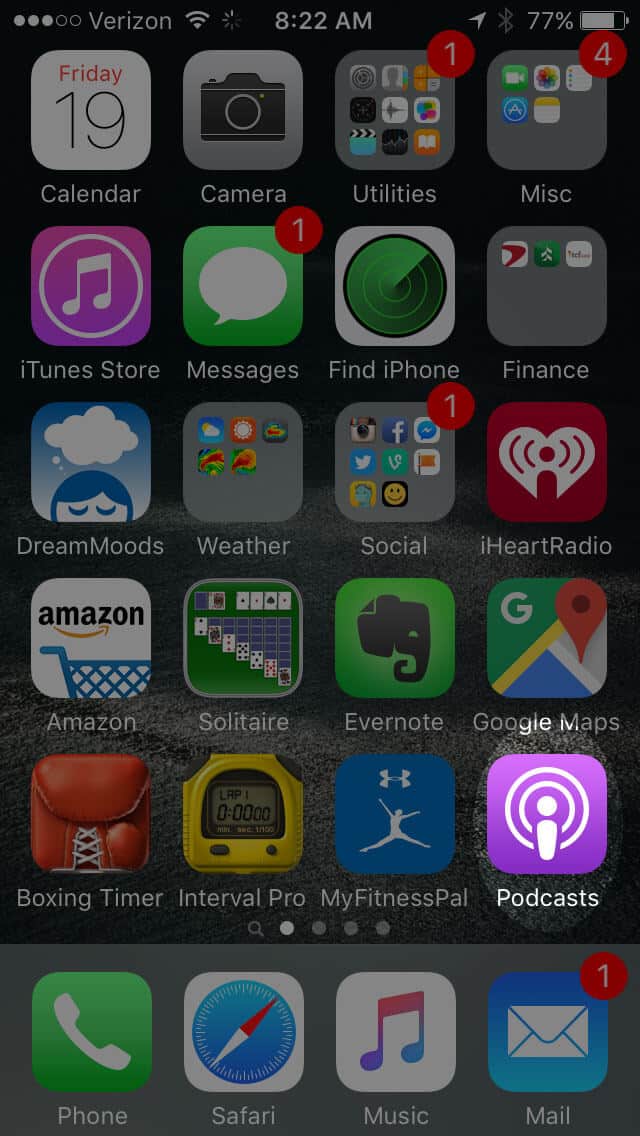
Open the “Podcast” app on your iPhone
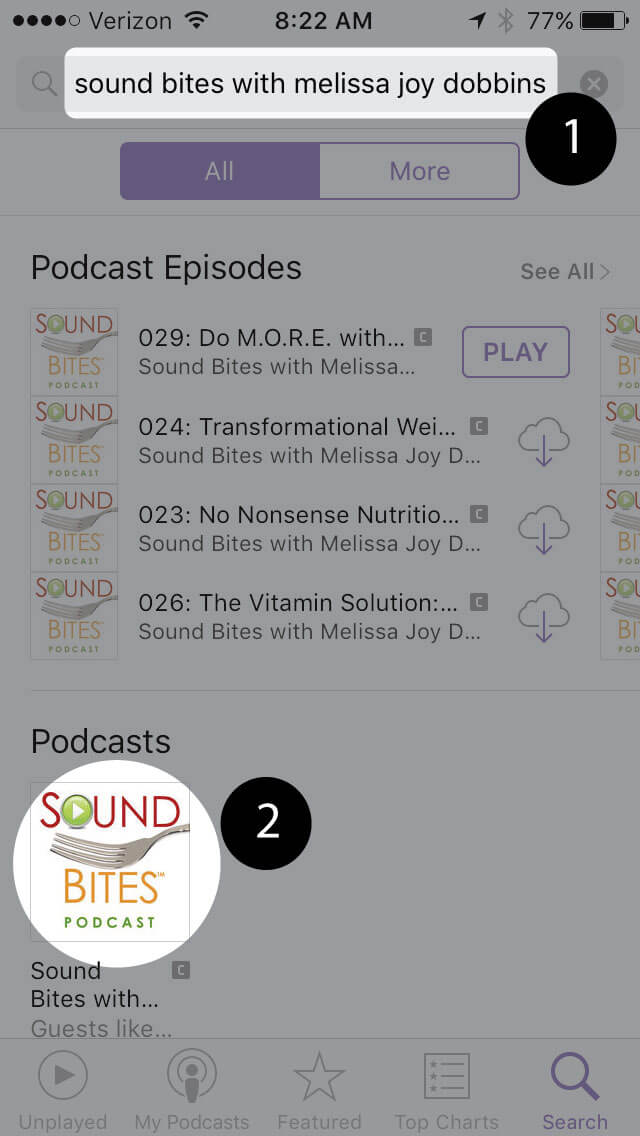
Search for “Sound bites with melissa joy dobbins”
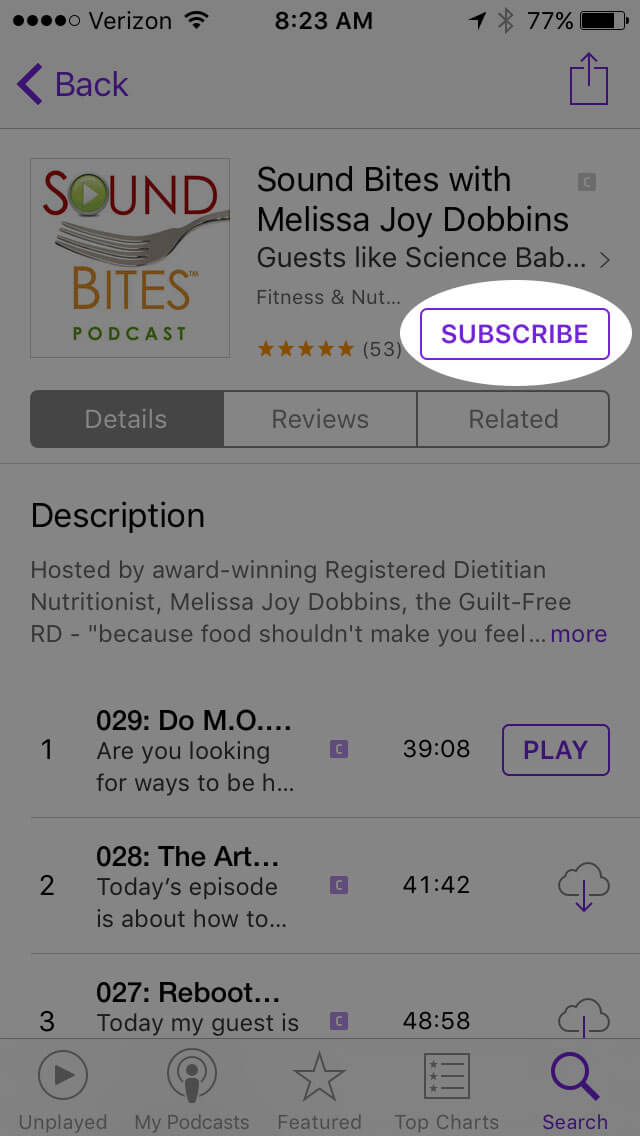
Open the podcast and click “Subscribe” and your done!
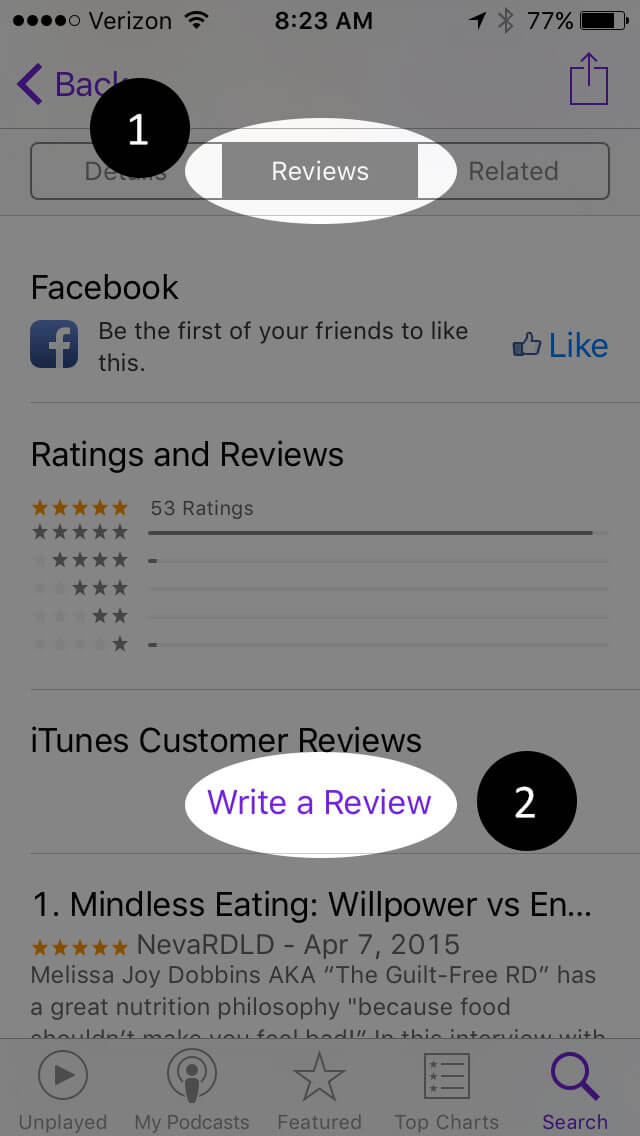
Write a Review
Click “Reviews”, then “Write a Review”.
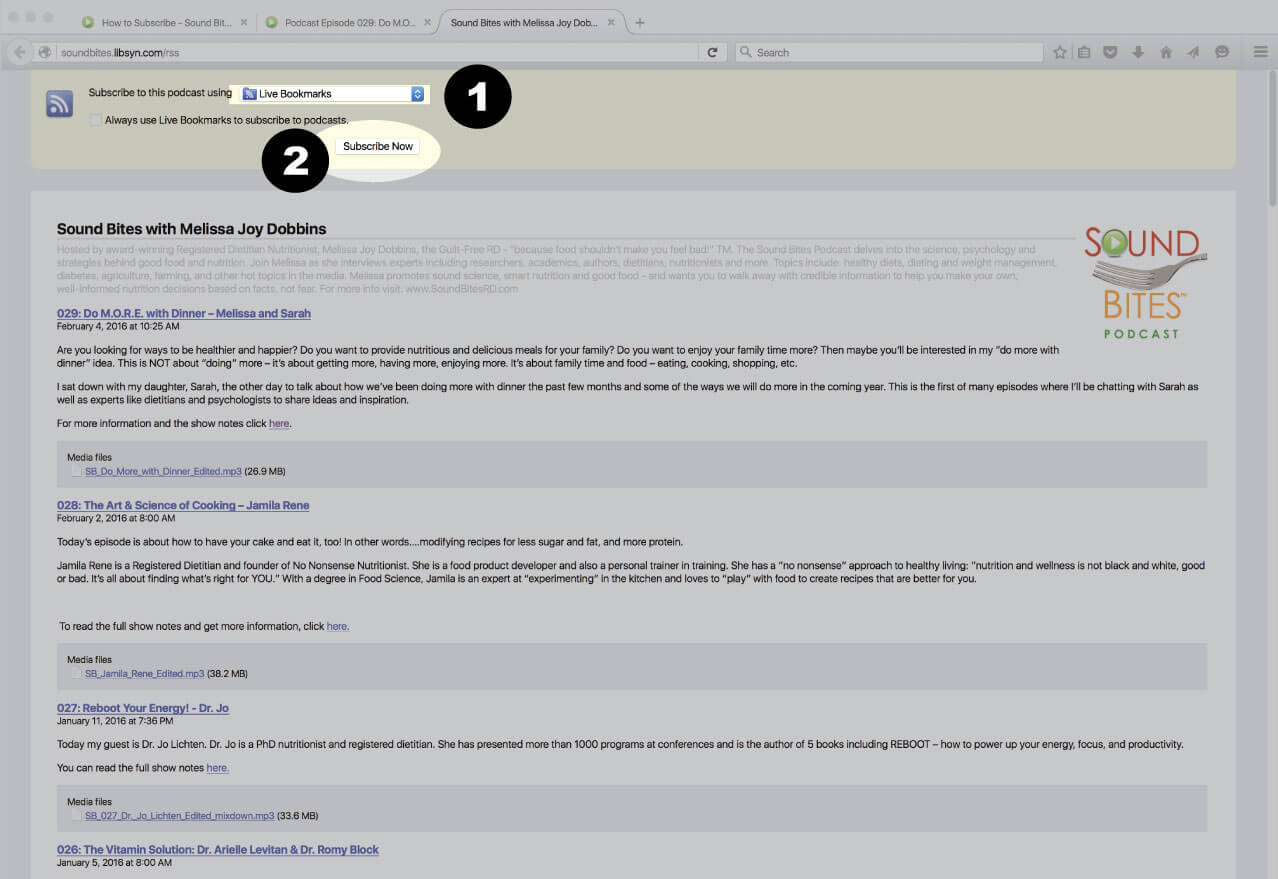
Subscribe via RSS Feed
Navigate to any podcast player . Click on the RSS feed icon.
Click on the RSS feed icon.
Click on RSS Feed
Choose which application you would like to use to receive the RSS feed
Click “Subscribe Now”
Confirm settings and subscribe.
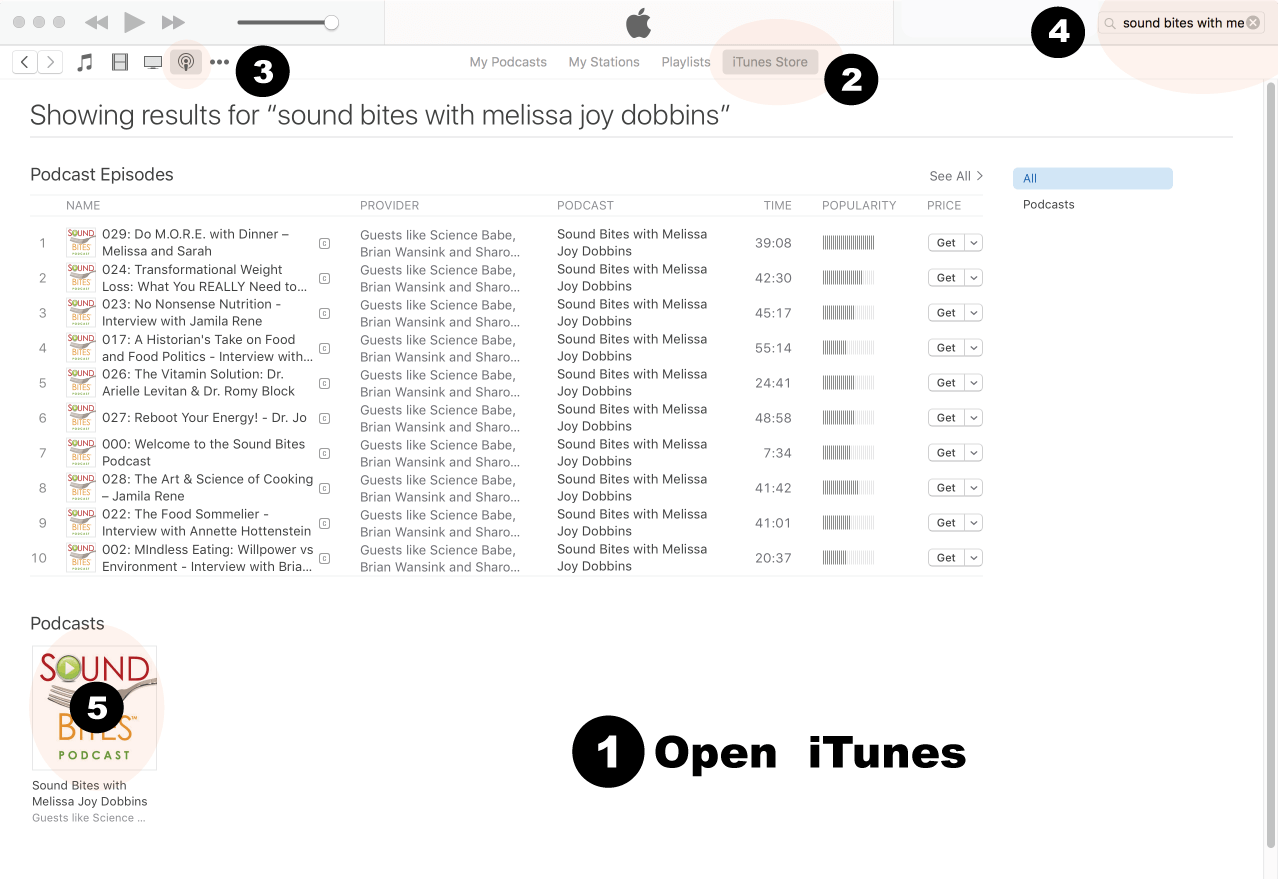
How to Review in iTunes
Open iTunes desktop application
Click iTunes Store
Click on Podcasts
Search for “Sound bites with Melissa Joy Dobbins”
Click on podcast image
Search for Sound Bites podcast in iTunes
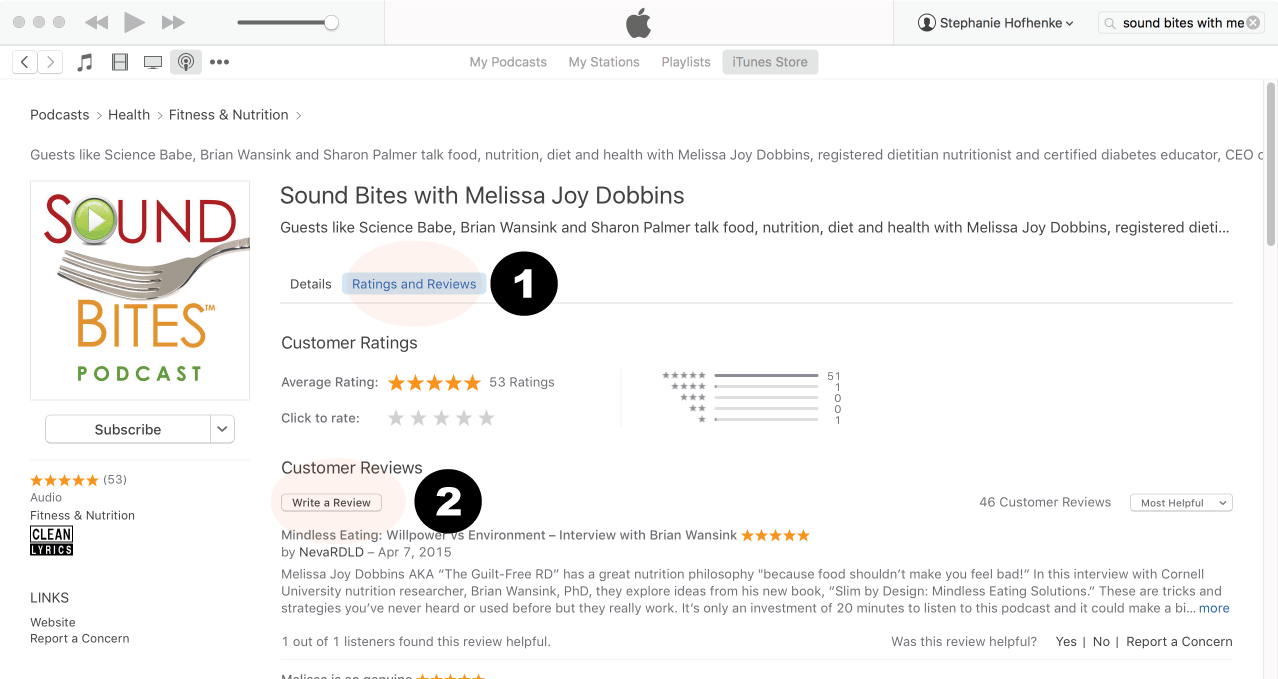
Click Ratings & Reivews
Click Write a Review
View reviews and write your own review.
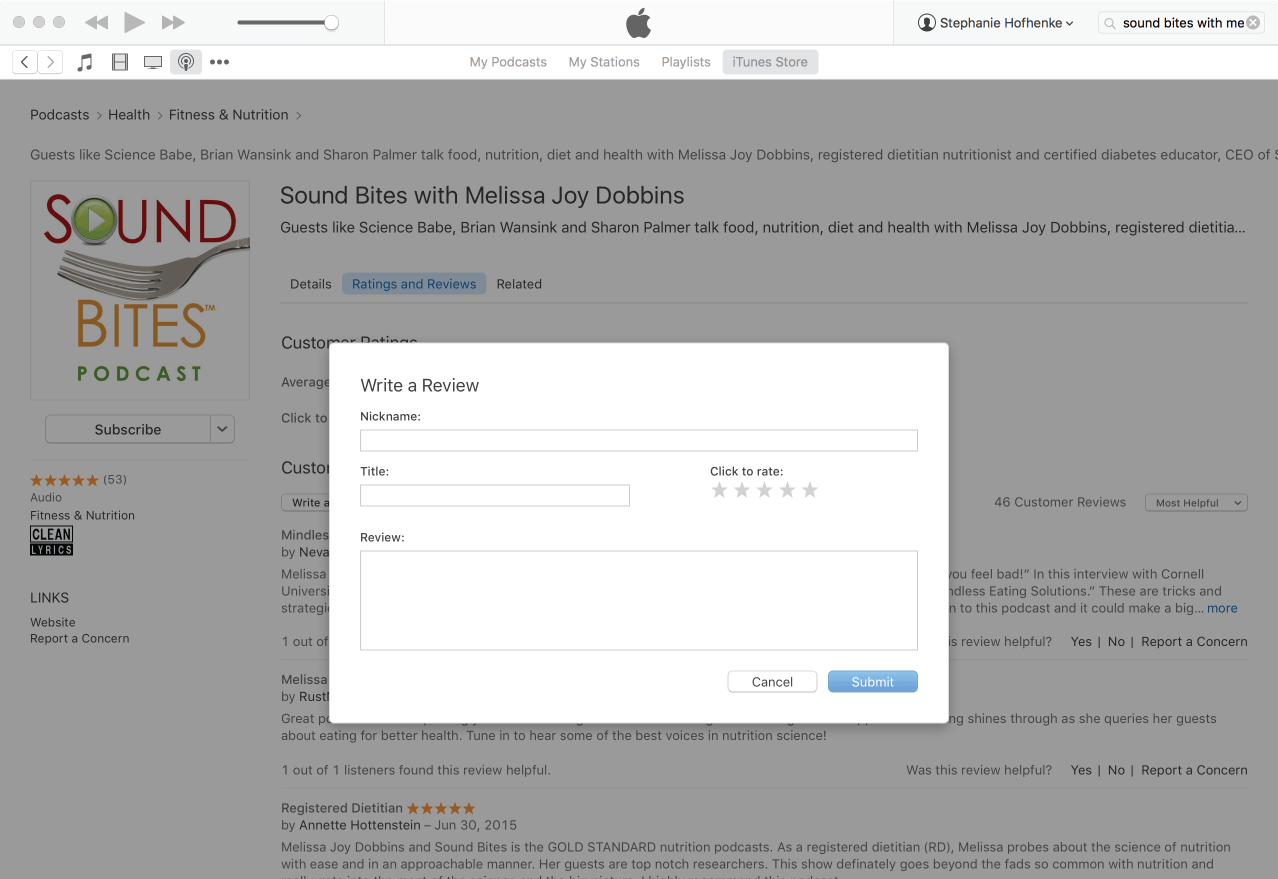
Write your review…. Thank you!
Write your review!
How to subscribe via iTunes
Click here to view the Sound Bites Podcastin iTunes, then click the blue “View in iTunes” button. This will open your iTunes application directly to Sound Bites Podcast. Click the “Subscribe” button, and your done!














excellent interview! great amount of information that was very practical – love the “whys” things happen…
Very informative!