Celebrating over 1 Million Downloads and 50,000 Free CEUs on the Sound Bites® Podcast | NEW: Get 1 years’ worth of CEUs with the new 15-CEU Podcast Course
Beyond Thirst: The Crucial Role of Hydration on Health & Performance
The connection between hydration and health is a relatively new and still under-researched area of science. However, emerging evidence suggests that staying well-hydrated plays a far more significant role in our health than most people realize. While it’s widely known that adequate hydration supports healthy bowel function and helps regulate body temperature, research shows it also impacts a variety of health factors ranging from exercise performance to kidney function and even the risk of developing chronic diseases such as cardiovascular disease and diabetes.
Adequate hydration might be the most economical and practical way to improve health and wellbeing.” – Dr. Stavros Kavouras
Tune into this episode to learn about:
the difference between dehydration and underhydration
the paradox of hydration
common myths about hydration
what happens in the body when you’re not optimally hydrated
what research shows regarding the impact of hydration on kidney function, UTIs, kidney stones, cortisol levels, glucose regulation, development of diabetes, fatty liver disease, life expectancy, dementia and cardiovascular disease
how hydration Impacts endurance and strength during exercise
how to determine if you’re underhydrated
how much water/fluid people are actually drinking
if there’s any validity to the “8 glasses a day” recommendation
if thirst is a reliable signal for hydration
the difference between a high drinker and low drinker
tips for staying adequately hydrated
Stavros Kavouras, PhD
Dr. Kavouras is a Professor of Nutrition, Assistant Dean of Graduate Education for the College of Health Solutions at Arizona State University, and the founding director of the Hydration Science Lab. His lab studies how fluid intake impacts health and performance. Dr. Kavouras has been one of the top 2% of the world’s most cited scientists over the last 5 years, the author of more than 170 peer-reviewed articles, cited more than 12,500 times (h-index 60), and has given lectures in 31 countries. His current research focuses on:
Fluid composition for optimizing hydration and performance
Hydration and temperature regulation
Children’s hydration
Hydration, glucose regulation, and cardiovascular health
Professor Kavouras is a fellow of the National Academy of Kinesiology (#637), the American College of Sports Medicine, and the European College of Sports Science. He is also an elected member of the American Society of Nutrition, the Obesity Society, and the American Physiological Society.
I’m not saying that we’re going to cure diabetes by drinking more water, but it’s probably one of the players and potentially one of the easier targets that could help to protect yourself from hyperglycemia and diabetes.” – Dr. Stavros Kavouras
Resources
Some links may be affiliate links. As an Amazon Associate, I earn from qualifying purchases.
Speakers: Melissa Joy Dobbins & Dr. Stavros Kavouras
[Music Playing]
Voiceover (00:01):
Welcome to Sound Bites, hosted by registered dietitian nutritionist, Melissa Joy Dobbins. Let’s delve into the science, the psychology, and the strategies behind good food and nutrition.
Melissa Joy (00:23):
I’ve been getting a lot of questions from listeners about the continuing education credits that dietitians can get for some of my podcast episodes so I want to clarify that I do offer free CEUs for SOME episodes -but not ALL episodes. I have about 3 year’s worth of FREE CEUs as well as some very low cost CEUs and a package on sale for one full year’s worth of CEUs if you want the convenience of taking just one quiz and getting one certificate for all 15 credits. This is a fun and easy way to get your credits so check it out! Get all the details on my website at soundbitesrd.com/freeceus.
Hello, and welcome to the Sound Bites Podcast. Today’s episode is about hydration and dehydration or underhydration, and specifically, how hydration status impacts health and performance. And of course, we will share some tips and takeaways for staying well hydrated. This episode is not sponsored.
My guest today is Dr. Stavros Kavouras, who is also known as Dr. Hydration. He’s pretty active on social media, and he is a Professor of Nutrition and Director of the Hydration Science Lab at Arizona State University. He is one of the top 2% most sided scientists in the world, and his lab studies the role of hydration on health and performance. Welcome to the show, Dr. Kavouras.
Dr. Stavros Kavouras (01:48):
Thank you, Melissa. It’s my honor to be here. Thanks.
Melissa Joy (01:51):
So excited to talk with you about this topic. I’ve been seeing a lot more about hydration in the media and social media lately, and I think one of the things that I’ve come to think about is there’s a lot more than meets the eye.
So, before we get into the topic, I would love for you to share more with our listeners about your background and the work that you do, and please also include any disclosures to note.
Dr. Stavros Kavouras (02:17):
So, as you mentioned earlier, I direct the dehydration science lab at Arizona State University. I would say 99% of our studies are primarily focused on how drinking adequate amount of fluids can help health and performance. We have a keen interest on glucose regulation, which hopefully, we’ll go over that information a little bit later on.
I started as a hydration physiologist, primarily studying dehydration and exercise performance, and I think most of the people in the field that are working around hydration, this is how most of us started looking at how your body performs, what is your limits to performance when you exercise in difficult environments: heat, altitude, very high intensity of exercise, and how dehydration either limits your performance, or how fluid composition can enhance and maximize your performance.
So, this is how we started and done a lot of work on diabetes glucose regulation, obesity over the years, and circling back to how hydration ties up to all this health outcomes, I think has become the main focus of my work the last probably decade.
I’ve been in this business for a little bit more than 30 years studying hydration, health, and performance. It started I would say by accident probably. I started working with Professor Larry Armstrong from University of Connecticut who is one of the founders of the field, and I got excited working in this area and I’m still working in this field.
Melissa Joy (03:53):
Very good. You have some interesting degrees. I don’t have your resume in front of me, but I would love for you to share the various degrees that you have.
Dr. Stavros Kavouras (04:01):
Sure. So, my undergrad, actually, if you can say from my accent, I’m originally from Greece. I did my undergrad in exercise science in University of Athens. Then I worked at the U.S. Olympic Training Center working with U.S. Olympians, primarily from U.S. swimming team from University of Colorado at Colorado Springs.
Then I did my PhD in University of Connecticut, where this is when I really started concentrating on hydration. I followed up with more research on hydration and more on the mechanistic work on how your body handles water in different compartments, and I spent two years in Yale Medical School doing that.
Then I went back to Greece, I worked there for a few years as a professor. I was in the University of Arkansas before I moved here in Arizona State University in 2018.
I have also worked with elite athletes as a performance consultant, trying to provide them primarily, optimal hydration and how they can maximize their performance, especially when you look into performance in endurance events in harsh environments. So, that’s a little bit about my background, education, et cetera.
I forgot to mention my disclosures. It’s a long list because over the years, I’ve worked with almost every large beverage company probably in the world. I currently have several grants from USDA, from Standard Process, from Unilever, and the list goes on.
Melissa Joy (05:33):
Okay, wonderful, thank you. I know obviously, with performance, you’ve worked with a lot of athletes like you said, and I think as we go through our conversation, it will be helpful to learn are there many differences between the non-athlete and the athlete, so some of my questions are going to be geared towards that.
But I guess a good place for us to start would be just the term “dehydration.” Is there a definition of this that you could share? And I learned the term “underhydration” from you, so I think you prefer that term, and I’d like to have you talk to us about why.
Dr. Stavros Kavouras (06:08):
Yeah, I’ve been thinking of it extensively during the last probably 10 years about what is dehydration, and I know it’s a term that everybody’s using. I would say quite freely, people wake up in the morning like, “Oh, today I’m dehydrated.”
So, dehydration by definition (and dehydration is a medical term, it’s an established medical term for a long time) means significant water deficit. So, your body is lacking water. And the significant, usually, most people will define that of a water deficit of at least 2%. So, 2% of your body weight of water deficit, which is relatively small.
And if you think of clinical practice and hospitals, clinicians, they call up to 5% dehydration a mild dehydration, and 10% or more, they call it the serious dehydration.
Just to give a little bit of perspective of what dehydration means, like about 12 to 15% dehydration. So, if you lose 10 to 12% of your body weight in water, especially if it is relatively in a short period of time, this is usually the threshold that people start getting so many complications that they will probably die.
And primarily, the main complications you get are complications related to kidney failure, to kidney function. So, your kidneys stop working appropriately and then you have a lot of complications related to kidney dysfunction. So, this is dehydration.
So, if somebody haven’t had adequate amount of water the day before, you didn’t drink much – you woke up in the morning, you forgot to drink, you had maybe half a cup of coffee, you run to the office, you didn’t have water with you, you didn’t have water in your office. So, this is not dehydrated. You’re not dehydrated because your body has a variety of homeostatic mechanisms, so mechanisms that can protect you from getting significantly dehydrated.
However, the however question that I get: is it okay to be in that situation where you don’t drink much, that probably you don’t have a significant water deficit? So, by medical definition, you’re not really dehydrated.
So, that state where you’re not optimally hydrated but you don’t really have a clinical dehydration, this is what I call underhydration. And actually, it’s not only my idea, several scientists have been trying to describe that, and actually, I like to make the comparison between underhydration is something like preliminary stage of dehydration.
So, how we call diabetes for instance, if your fasting glucose is not 140, but it is 112, 115, that we call it pre-diabetes — I would like to think a little bit of that nature.
So, more like a continuum where if you are in the state of underhydration where you already are high in risk of health outcomes and performance, then you’re much closer to develop dehydration and have more serious implications, whether you’re an athlete or whether you are just a regular human being with I would say, relatively sedentary lifestyle.
Melissa Joy (09:32):
Okay, yes, I was thinking of that phrase when you were talking optimally hydrated, and then you said it, so that makes a lot of sense.
So, how much research is there on hydration?
Dr. Stavros Kavouras (09:42):
I like to say that water has been or hydration has been the forgotten topic in nutrition science. When I talk about hydration, especially when I’m in a conference and I have a relatively introductory presentation on the topic, I like to go through the history of nutrition outlines, and trying to show different milestones in nutrition and what we know and what we don’t.
So, one of the exercises that I like to do is I take this series of peer review published papers on the history of nutrition. These are four papers that they were published, if I remember correct, it was by Carpenter in 2008, that they went in four different areas, chronological sequence of research and nutrition and different milestones like Vitamin C and big milestones in nutrition.
So, when I first discovered those papers, I did what most geeky scientists would do if you’re looking at something very specific. Very quickly, I opened the PDF file, I press control F, search bar popped up and I put the word “water” or “hydration” or anything related to that, enter, and I got nearly nothing. So, they’re four papers, I will do this exercise in every single paper.
And then in one window of time, I got about 15 references. I’m like, “Oh my goodness, there was something there that I completely missed, and I’ve never read about it.” And I started looking. So, the PDF reader picked the component “water” from the name Atwater who is one of the founders in nutrition, and the American Society of Nutrition has a national award in the name of Atwater who was a Connecticut resident. He was a professor in Connecticut.
I remember growing up as a scientist and one of our lecture halls in University of Connecticut, it was called Atwater. He’s like such an important person in the field. So, I got excited for about 10 seconds, then I’m like super-
Melissa Joy (11:46):
It’s not water.
Dr. Stavros Kavouras (11:48):
It did mean something, but on the other side, it wasn’t like anything that important.
Another piece of evidence that I like to use is when we talk about nutrition in general, we talk about consumer-friendly nutrition guidelines, which is my plate, this is what everybody recognize. And my plate doesn’t have water. If you look at it carefully, on the side of the plate there is a circle which it says dairy. So, our pyramids didn’t have anything.
You go all the way back from the beginning of the equivalent, we had the three elements, the five elements on and on over the years – the pyramidwith the bottom to the top, the pyramid with the slices, but it looked more like a pizza slice, and then to my plate now. So, we still don’t have water like if water is not important.
Melissa Joy (12:36):
Yeah, it’s crazy.
Dr. Stavros Kavouras (12:37):
So, I like to use the term water, the forgotten nutrient because you even look in research studies, you look in large epidemiological studies of the seventies, eighties, nineties, early 2000, and even up to relatively recent days, they will not even record water. So, they will record every liquid that people ever drink, every food, every micronutrient, but not water.
Melissa Joy (13:03):
Wow.
Dr. Stavros Kavouras (13:04):
I’ve heard people comparing water like oxygen, like you don’t need to think about it. Oxygen is important. You don’t have oxygen for five minutes, you die. We don’t think of oxygen as a nutrient. I’m like this is not the same.
So, this is, I would say, quite unfortunate there hasn’t been studied extensively. When I start talking more about hydration, maybe more than 10 years ago, I was a little bit less optimistic than I am today because the last 10, 15 years, we have a significant growth on what we know about water intake, hydration, and the mechanisms behind.
So, it’s not only what water does in your body, what we know about water, but also how does it work, and what is the mechanism of action, and how we can address problems that we never thought that we could address by drinking more water. And we’ll talk a little bit later about glucose regulation and water intake.
Melissa Joy (14:01):
Yes, I definitely want to get into that. As a certified diabetes educator, that really caught my attention, and yet, I was curious if we know the mechanism. So, we can definitely get into that.
So, maybe just give us an overall what research shows in general about the impact of hydration status on health, and then also performance because I imagine those are like two different things.
Dr. Stavros Kavouras (14:25):
I will start from performance because it’s a little bit easier, and there is also a lot of information in performance. So, we know now for many years that when you exercise, especially when you exercise even in a hot environment, you don’t consume adequate amount of water.
So, as you exercise, you are becoming dehydrated because you sweat more than you normally drink. Assuming that you have access to water, you can drink as much as water you have, and even if you have optimal situations where it tastes good and it’s cold and it has carbohydrates and it has sodium to help you … palatability and all that stuff – even in those situations, you are under drinking. We are programmed this way.
So, we know that when you are developing dehydration while you’re exercising, your performance declines. And it mainly declines because you lose a significant amount of water from the water in your blood, so your blood volumes shrinks.
And then as a sequence, your cardiovascular system, your heart doesn’t work very effectively. You cannot transfer heat from your active muscles to the skin to be able to dissipate the heat to the environment. Your metabolism, it doesn’t work effectively. So, exercise performance declines significantly.
And when we talk about exercise in the heat in endurance events like 10k marathon running, ultra events, Ironman, cycling, et cetera, then we have found actually in multiple labs and in my laboratory, that even a small decrement of total body water, like you lose 1% of body water, your performance declines.
We can pretty much predict how much hotter your body will be for every percent of dehydration that you’re developing while you’re exercising. So, your body’s hotter, your heart rate is higher, you perceive the same exercise as more difficult, and when you are competing at the race kind of intensity, you’re underperforming. So, those things are super straightforward.
And we also did a really interesting study in my mind trying to address the question that quite often people say that the studies that you do in a laboratory, they are a little bit what you find with even small degree of dehydration. You have what is called the anticipatory response.
So, when a volunteer comes in the lab and you tell them today you’re not drinking anything, it’s a dehydration trial, they’re expecting to do worse. And if they expect to do worse, they will probably do worse, which makes sense.
So, we did this study a few years ago. We took people, we put nasal gastric tubes. So, we put a tube from their nose all the way down to their stomach. We brought them back multiple times, and in one of the trials, we make them exercise without giving them any water through directly into their stomach.
In another trial, we were pumping significant amount of water to keep them optimally hydrated, and while we were giving them a small amount of water to drink so their mouth will not dry up, would not feel uncomfortable, et cetera – we went to a large extent, tried to blind them with the pilots, we manipulated the water temperature so they won’t feel the temperature of the water coming down and on.
And we found that even in that case where subjects were not thirsty, they could not say whether water was coming into their body or not. Still their exercise performance was lower. So, dehydration really decreases exercise performance. And this is pretty straightforward, especially for endurance events.
When you look in strength, it usually takes a little bit longer, a little bit larger degree of dehydration to start seeing differences on maximum strength, explosive power and stuff like that. So, for shorter, higher power events, it takes a little bit more dehydration. You need at least 2, 3% or more. But for endurance, even 1%, it has an impact.
So, that is a little bit of a brief summary of what happens when we exercise and we’re either not starting well hydrated, or we are getting dehydrated as we go, which is very common.
Melissa Joy (19:05):
Great. And I’m just taking some notes because this is kind of an aha for me, is like your hydration status depends on where you’re starting off at. If you were well hydrated the day before or when you wake up, that’s sort of a thing. So, that’s very interesting.
So, that’s kind of the overview for performance. What do you know about the impact of hydration just on health?
Dr. Stavros Kavouras (19:27):
So, health is something that we have started to learn the last few years, actually what hydration does on health. Of course, we know that if you don’t drink water for a few days, it’s going to be fatal because humans cannot survive without water.
And one thing that is extremely … it was for me at least what they call the aha moment, the paradox of hydration, what I call – is that water is the single nutrient that we have so much in our body, way more than anything else. Like half of our body is at least water. It depends on age and body composition and sex and on.
But about half of it is water. Like an average person has 10 gallons of water, and then I’m telling you, you lose like 20 ounces and your exercise performance declines. And you look from the other side, I keep going back to glucose regulation; you have five grams of sugar in your blood, which is like a teaspoon of sugar.
We say normal is anything between … for fasting, we say anything up to 110, 70 to 110, you’re okay. Or 70 to 125, you’re almost okay. Or any random throughout the day, you could be anywhere between 70 to 200 and you’re okay. So, you can double triple your five grams of sugar, and then you have 10 gallons, and you lose a tiny amount-
Melissa Joy (20:57):
You’re not okay.
Dr. Stavros Kavouras (20:58):
And I’m like, “Oh my God, they cannot thermoregulate well; oh my God, they cannot perform well.” But on health per se, I think the single area that we know the most right now is the impact of hydration on kidney function, and anything around how our kidneys operate. So, whether it is kidney stones, chronic kidney disease, urinary tract infection.
And just to emphasize again that the fact that we know still very little. It was less than five years ago that the first study was published on the impact of increased water intake on urinary tract infections. And most people go to their doctor and they say drink more water and that should decrease their recurrence of UTI. But that was an empirical advice.
Melissa Joy (21:50):
Seems to make sense, right?
Dr. Stavros Kavouras (21:51):
Yeah, it should make sense. So, the first study was published a few years ago, and it was published in JAMA, very well controlled large study with a lot of people and on. And so, that if you increase your water intake (I think in that study, they were giving one extra liter of water per day, which is 32 ounces, extra water per day) you decrease tremendously the frequency of recurrence, the consumption of antibiotics, the complications, and the recovery and on.
For kidney stones, people that they have tendency to develop kidney stones, the guidelines, if you talk to a urologist, they say you have to drink … actually, they don’t say how much you have to drink. They say you have to pee at least two to two and a half liters of urine per day. So, you have to pee a lot. So, to pee a lot, you have to drink a lot.
So, to be able to produce a lot and dilute urine. When the urine is diluted, then the possibility of crystallizing of creating new kidney stones, it’s way smaller. So, to pee two and a half liters, you have to drink at least three liters per day, which is about 12 glasses of water probably per day.
Those are the immediate things, the stuff that people think when they try to associate hydration and health. But nowadays, we have significant amount of information on factors that we have not thought about traditionally.
So, issues like cardiovascular disease, people that they consume small amount of water, and they’re not optimally hydrated, they have higher risk for cardiovascular disease. We have data on glucose regulation, diabetes development, fatty liver disease, the data on life expectancy actually and longevity.
So, we published a study about three years ago. We took the NHANES data, the National Health and Nutrition Examination Survey. So, the national survey data, we identified people that there were small drinkers, people that they don’t consume adequate amount of water, we defined them with biomarkers, et cetera, and we use another database to see a number of deaths, et cetera.
And we found that people that were underhydrated – I’m not talking about people that they’re clinically dehydrated, that they end up to the hospital and they can die. So, I’m not referring to sick people that they were patients in a hospital. I’m talking about healthy people, apparently healthy people that are underhydrated.
So, people that they live underhydrated, they have shorter life expectancy, and underhydration is associated with chronic disease like hypertension, chronic kidney disease, diabetes, and actually an obesity as well. So, obesity was also one of the items that we found in that analysis.
And there are a couple more studies actually from the NIH, the National Institute of Health. They have, other than funding research to different universities that now people learn more about this process and with what is happening these days – NIH also does internal studies. So, they do their own studies, and usually, they do those very complicated, very prolonged studies that takes many years that are very difficult studies to do in a university or a hospital setting.
So, there are a couple papers that they have published from their internal studies, and they have also shown very similar results, showing that underhydration is associated with life expectancy, chronic disease, et cetera. And one thing that was very interesting that there is very low information in this topic, in a prediction of what are the disease that they’re high risk of somebody developing a chronic disease based on underhydration – the number one that came up was dementia, which is one of those black boxes disease that we kind of know what causes it. We kind of think we know, we’re still trying to figure out how to address it and what to do and how to prevent it and on.
But I would say it’s early indication, but I was extremely interested to see this kind of data that even the brain has significant amount of water is affected by being underhydrated.
Melissa Joy (26:22):
And are these studies that you’re talking about, are these association correlation epidemiology studies?
Dr. Stavros Kavouras (26:30):
So, most of them are epidemiological studies, and I keep using they’re associated. So, when we hear the word associated, it means epidemiological. This is usually the first approach. So, this is what you first do. The kidney studies actually, the data that we know from kidneys are randomized control trials. So, there are several of those studies with interventions, et cetera.
For cardiovascular disease and dementia that I mentioned and longevity, those are associative studies. So, the epidemiology is the first approach when you have a question, this is the first thing you do. You try to identify what is associated with, you cannot talk about causality per se.
But after that, then you follow up and you do other studies trying to examine the mechanism, and then you do the randomized control trials, which is the highest level of studies that you can do to see what is happening.
Melissa Joy (27:24):
Yeah. So, let’s talk more about the glucose regulation. Tell me about your research on that.
Dr. Stavros Kavouras (27:29):
Sure. So, the story started again from epidemiology, that was the first observations. There were a few studies, one of the first ones was from France. They follow a France cohort for six years and they found people that were consuming small amount of water, they end up having higher glucose levels, and higher incidents of converting from normal glucose to hyperglycemia and diabetes.
So, they were trying to figure out what causes – and I’m not talking what most people will probably say you drink probably more water because the water, if you drink a lot of soft drinks have a lot of water. So, you do take a lot of water, and it’s potentially the sugar and on.
I’m not talking about the sugar, I’m talking independent effect, independently of the amount of sugar that is consumed. So, the obvious culprit in that situation, when they start looking what happens when you consume small amounts of water, one of the first body reaction and low water intake is that your body produces a hormone from the brain, which is called antidiuretic hormone or vasopressin.
So, it’s the same hormone, it has two separate names. The original name was vasopressin because it was the first hormone that was discovered in 1896, and it was found for the effect on raising blood pressure. So, when you get dehydrated and you start getting dizzy and your blood pressure drops, your body produces this hormone that maintains your blood pressure. So, it has an effect on veins, on your vasculature.
So, it’s suppresses your vascular bed, and that helps you to maintain blood pressure. So, we know where those receptors are and how it works and on. Later on, we found that also the same hormone does another thing to prevent you from losing more water, which is the second name, the antidiuretic, so decreases the enuresis. So, the hormone decreases urinary output.
So, for many years, we have known that this hormone, antidiuretic or vasopressin, has an impact on blood pressure regulation and on urinary output. If you don’t drink much, you don’t pee that much. And when you pee, your urine is very concentrated because the effect of this hormone is trying to extract as much water out of the urine that is produced in the kidneys.
Melissa Joy (30:00):
To hold onto that water.
Dr. Stavros Kavouras (30:01):
Exactly. So, your body knows that you’re not drinking adequate amount of water and say, “Hey, hold on as much as you can.” And by the way, when you start losing even more water, then let’s keep the blood pressure normal so that person will not pass out. So, this is the hormone, which I believe is the key to many negative impacts of underhydration on health.
So, we have learned that this hormone outside of the kidney and blood pressure effect, there are many effects in variety of other organs, and there are receptors, there are some of the receptors for this hormones in the pancreas and in the liver. And it seems that those receptors, when they get activated, they play a significant role on how your body regulates blood sugar.
So, outside of the associated studies, we’ve done a few studies in my lab. So, first of all, we took patients with diabetes, we cut them off their medication, we brought them in the lab, and we did an oral glucose tolerance test.
So, you give them a significant amount of sugar and you’re looking at how they handle blood glucose. So, we found that their blood glucose was significantly higher when they were consuming for three days smaller amounts of water versus when they were consuming adequate amount of water. So, the amount of water that you drink impacts how your body handles glucose.
And we also found, which was a little bit surprised, but not surprised at the same time, that during the test, their blood cortisol, it was significantly higher. Even though we say when somebody eats food, when you eat sugar, when you eat glucose, cortisol gets suppressed, and you have lower cortisol – cortisol is a stress hormone.
When you’re underhydrated, cortisol is higher. This is one of the things that happened. There is physiology behind it how it happens. And we know the mechanism through ACTH and the adrenals, and how your body produces the thing.
But the interesting thing is with cortisol, is that if you’re (something that will describe in a little bit) a small drinker, somebody that chronically consumes small amount of water, you have chronically elevated cortisol, and that cortisol doesn’t go down until you start drinking more fluids to be able to suppress. So, you drink more fluids, you suppress the antidiuretic hormone, and then you decrease cortisol. So, this is the pathway.
So, we did the study with patients with diabetes. We did another study where we brought people in the lab, and we did a technique where we put something that looks like salty water. Intravenously, it’s called hypertonic saline. You infuse salty water and that stimulates. Your body sees it as a dehydration, so you’re doing a cellular dehydration on your body. Even though you put extra water, because it’s so salty, it dehydrates your cells.
So, we stimulate your body’s endogenous production of vasopressin, and then we measure again glucose regulation. And we found that when your body has high levels of vasopressin, your blood glucose is about 15% higher. And we also found that your insulin is lower.
And we also found that your glucagon, which is the emergency hormone that your body produces to release glucose from the liver, it’s also higher. So, your body sees that as an emergency situation when you have high levels of vasopressin or antidiuretic hormone, and it pumps more glucose in your bloodstream, and you have higher levels of glucose.
So, all these associative studies that we have found, they seem to be related to this hormone. So, we have more plans for the future. We did a study where we took the hormone as a drug and we did intravenous infusion in my lab and we measured very precisely insulin resistance.
But I would like to mention one study which is in mice, it’s not in humans, but the results are very interesting. So, they took mice, and they injected them for four weeks with antidiuretic hormone. Within two weeks, they developed hyperglycemia, within four weeks, they had diabetes.
Then they took diabetic rats, a specific strain of rats that are obese and diabetics, and they inject them with vasopressin blockers. So, specific drugs that they block the action of the hormone only in the liver and the pancreas. And they found that by injecting them with the blocker of antidiuretic hormone, their blood glucose improved significantly. It was significantly reduced during tests that they did in those animals. And also, their fatty liver disease was improved significantly as well.
So, there is a lot of things, I think we’re barely scratching the surface. I’m not saying that we’re going to cure diabetes by drinking more water, but it’s probably one of the players, and potentially, one of the easier targets that you could help your body to protect yourself from hyperglycemia and diabetes.
Melissa Joy (35:12):
Wow, very interesting. Thank you for sharing all of that.
You mentioned with the kidney stones having to pee two to two and a half liters per day, which means you would have to drink three liters per day. We used to hear this advice to drink eight glasses of water a day, and then there was a lot of talk about how that didn’t have any scientific basis. Is that true? And also, what is the recommended amount of water or fluid?
Dr. Stavros Kavouras (35:38):
This is a very interesting story that I have looked extensively to see why there is so much hate against eight glasses of water from people.
So, there was a retired professor emeritus I believe from Dartmouth University, Dr. Valtin, where he wrote the paper in 2004, a review paper trying to look in the literature and find where the eight glasses of water comes from. And eight glasses is eight by eight, actually – eight glasses of eight ounces, which by the way, nobody owns eight ounces glasses probably at home. Most of our glasses are much bigger nowadays I think, it’s difficult to find eight ounces.
Melissa Joy (36:19):
Yes, that’s a good point.
Dr. Stavros Kavouras (36:20):
Anyway, the long story short, the paper had no data to say that whether eight glasses is good or bad. There were no data to associate whether people that they drink, I don’t know, four glasses of water versus 12 glasses of water are better off or anything.
But the main outcome of the paper, of their synthesis, the review of the literature was that there is no scientific basis for the eight glasses of water. So, they had some potentially sources of how this thing started, but there were no data to support that eight glasses of water is what we’re supposed to drink. So, a lot of media people read that, and they translated as we don’t have to drink.
Melissa Joy (37:04):
We don’t need to drink eight glasses (laughs).
Dr. Stavros Kavouras (37:06):
Exactly. So, this thing keeps going on for decades after 20 years ago that this paper was published. And more recently, a few years ago, there was a large consortium of scientists from the International – actually, there is what is called International Atomic Energy Commission, and what the atomic energy has to do with hydration …
But one of the tools that we’re using to assess energy expenditure in humans, we use what is called doubly labeled water. So, it’s a water which is a stable isotopic water that has heavier hydrogen. So, instead of the hydrogen-1, it has the deuterium, which is heavier, stable, and it’s not radioactive.
Deuterium, the hydrogen-3 is radioactive, and then there is instead of the oxygen-16, which is the regular oxygen, which is the 99.9% of whatever we’re breathing, there is also oxygen-18 which is slightly heavier, very difficult and very expensive to find. Both of them are expensive to find, and because it’s a stable isotope, it’s controlled by the International Atomic Energy Organization.
So, that heavier oxygen and heavier hydrogen, you can consume a small amount, take some urine samples a few days later, like a week later, and you can go back and say you burned so many calories, which it looks almost like magic. And it’s something as a gold standard, I would say in nutrition if you want to assess energy expenditure.
But based on those numbers, you can go back and calculate how much water people are drinking during the same period of time. So, when you have the decay of hydrogen-2, of the deuterium decay, you can do math and calculate quite precisely how much water these people were drinking.
So, they took a massive database of thousands of subjects over the years. They wrote this wonderful paper that they explain how much people drink across the world in relationship with their sex, their height, their weight, their non-physical activity levels. And then at the end, the conclusion of the paper was, by the way, you don’t have to drink eight glasses of water.
And I’m like, “Oh, hold on …” What confirmed like … we knew nothing, whether these people were healthy, whether they were sick. And actually, if you see how much most of these people were drinking, they were drinking close to 12 glasses of water per day, by the way.
Most of those people that they participate in this variety of studies, which is not necessarily the average people that you will see out in the streets. So, this is a little bit of a background, the eight glasses of water. So, many people feel quite passionate one way or the other without really having data to support one way or the other.
So, how much are we supposed to drink? You asked me that question, I gave you the very long answer why, what is the root of eight by eight or the eight glasses of water per day. So, by the way, the dietary guidelines that we have in the United States were published in 2000. The report was written in 2004, I think it was published in 2005.
It says for adult males, so it depends for babies and lactation and pregnancy in different stages throughout the life. But for adult males is 3.7 liters per day; for adult females, it’s 2.7 liters per day. So, number one issue is that most people in this country don’t understand liters. So, you confuse them right off the bat by giving them liters, even though most people know quarts, pints-
Melissa Joy (40:48):
Ounces.
Dr. Stavros Kavouras (40:49):
Gallons, whatever. Water is the nutrient of water, so it’s not necessarily tap water. So, water is any H2O, any water molecule that we ingest, whether it is water in the rice and pasta, water in bread, water in meat. Every food has water, everything. Even the driest food you think of, it has some water. And of course, fruits and vegetables, we say almost all the fruits and vegetables are at least 85, 90% water. And some are like, I don’t know, 95, 98%.
So, I’m saying all that because when people hear these numbers like, “Oh my goodness, this is a massive amount of water.” I’m like, “Yes, it is, because it includes everything, and it’s the water, the nutrient.” So, if you do the math, because most people consume about 20% of their total water comes from solid food and not from beverages – if you do the corrections for adult males, the equivalent number, it’s about three liters per day, and two liters per day for women.
So, for women, the two liters per day, which is 64 ounces, it happens to be eight glasses of water per day.
[Laughter]
So, eight glasses of water per day, it’s not necessarily wrong. For males, it’s a little bit higher. And those glasses, again, they’re not the 12, 16 ounces glasses that you have at home because most people have large glasses of water. They’re eight of eight ounces. So, for U.S. standards nowadays, I would say on the smaller (not necessarily the baby cups) size.
So, one thing to clarify how those numbers came out, so in 2004 when the Institute of Medicine at the time, now, it’s the National Academy of Medicine that they issued the dietary guidelines, when they published those, they did not have data to associate water intake amounts with disease and say, “This is how much you’re supposed to drink.”
So, what they did, they took reference values based on percentages from the United States. So, those are consumption means. They did not have biomarkers to say, “We’re going to find the people that are optimally hydrated and see how much they drink and give them that amount.” So, they could not do that. They did not have the data. So, some people argue that yes, we have some guidelines, but those are not necessarily scientifically developed guidelines.
So, we did this study a few years ago. We took people, we gave them this heavier water to know exactly how much they were drinking, we measured biomarkers (and again, this is only one study), and we found that the people that were optimally hydrated based on 24 hour urine biomarkers that indicate that their body is in good hydration state, the numbers came out nearly identical to the National Academy of Medicine guidelines.
So, we published this paper, and I think the title was something like The Dietary Guidelines for Water Seem to Be Fine.
So, with all this very long intro, I think eight glasses of water, it’s not that bad. I think eight glasses of water, it’s probably a good reference number for somebody to have a target. Of course, it’s not one size fits all.
So, if you are, I don’t know, a 90-pound small human being and a 400-pound linebacker professional NFL player who trains six hours a day, everything is supposed to be different, not only how much water you drink, how much energy you consume, how much protein you eat, and all.
So, a lot of people get really upset that eight glasses of water, and if I run an Ironman, I’m like, “How many people run Ironman? How many people do you know personally that run Ironman?” Most people are sedentary, they don’t run Ironman. Most people are not NFL players. Most people are not 400 pounds.
Melissa Joy (45:00):
Right. That was one of my next questions, was do some people need more water?
Dr. Stavros Kavouras (45:04):
Absolutely.
Melissa Joy (45:06):
You already mentioned lactating, pregnant, etc. So it sounds like body size too, because if so much of our body is water, that would make sense if you’re a smaller body or bigger body that you would have different needs. And then if somebody is sweating more or exercising more, they would need more. That all makes sense.
Dr. Stavros Kavouras (45:22):
If you live in Phoenix in the summer, for instance, where-
Melissa Joy (45:26):
Where you live, yes.
Dr. Stavros Kavouras (45:28):
This is where I am. We had nearly four months last year with over 100 degrees Fahrenheit every day.
Melissa Joy (45:36):
Yes, I know.
Dr. Stavros Kavouras (45:38):
So, you live in Phoenix, or you live in Alaska, it’s not the same. But the dietary guidelines are guidelines at the population level. It is not the guideline for every single individual human being.
Melissa Joy (45:54):
Right, right. And one of my other questions, I think you may have answered earlier: do we know how much water or fluids Americans tend to drink? I think you said that NHANES isn’t even collecting that data.
Dr. Stavros Kavouras (46:09):
NHANES collects this data actually.
Melissa Joy (46:11):
Oh, good, okay.
Dr. Stavros Kavouras (46:12):
We do have this data from NHANES, and we have the last 20 years now that they collect continuously. So, at the beginning, there used to be waves of NHANES. Now, we have continuous data. They report them in windows of two years.
The data that we know actually is that, especially in some groups, most people don’t meet the dietary guidelines. And those groups, the higher risk groups are the children and the older adults, especially male older adults. More than 90% of male older adults do not meet dietary guidelines. And the average deficit is nearly minus, I believe, three, four glasses of water per day compared to what they’re supposed to consume.
And older adults, there are multiple things with older adults. They don’t get thirsty quickly. When they get thirsty, they don’t drink as much. When they drink less than younger adults, they pee more than younger adults So, it’s quite complicated.
And with older people, especially fragile populations, if they take medication, some of the medication might impact thirst. Like a simple medication that very few people know that suppresses health-
Melissa Joy (47:25):
Suppresses thirst.
Dr. Stavros Kavouras (47:27):
Yep. It’s the SSRIs (the selective serotonin reuptake inhibitors or Prozac), most of the antidepressants suppress thirst.
Melissa Joy (47:35):
Wow.
Dr. Stavros Kavouras (47:36):
There are newer data now that GLP-1, which I’m afraid that the rest of the population is going to be consuming and anybody who wants to lose weight will start using Ozempic or the brothers and sisters of Ozempic. Ozempic seems also to suppress thirst along suppressing appetite.
Melissa Joy (47:55):
I have seen that, yeah.
Dr. Stavros Kavouras (47:56):
So, the medication that suppress thirst is complicated. So, older adults and children are probably the ones with higher risk of consumption.
Melissa Joy (48:07):
You mentioned a low drinker earlier, and I saw one of your research articles talking about low drinkers and high drinkers; define those.
Dr. Stavros Kavouras (48:18):
So, low drinkers, high drinkers is something that scientists came up with this idea to study the impact of how much we drink and how well we are. So, the original idea was like this is what we’re going to do, we’re going to screen people for how much water they drink. And water, again, I’m referring to total H2O.
So, we will classify them as high drinkers if we take the top 25%, and low drinkers if we take the lowest 25%, get rid of the middle 50%, and trying to see what is different between those low drinkers and high drinkers.
So, it’s not any metabolic condition or anything, it’s just people that they tend to consume more fluids versus other people that actually, we do a lot of studies looking at low drinkers. A lot of people self-report when they hear what I’m doing for research. I have people that they say, “You should study me because I rarely drink any water. Maybe some coffee, maybe some with my meals, but I don’t drink that much.”
So, this is the definition of high/low drinkers. So, we took those two different groups and tried to see what is different between those two people. Those were some of the first cross-sectional descriptive studies that we did, and we found higher levels of antidiuretic hormone, we found the higher cortisol, we found the more concentrated urine and on, and things like that.
Melissa Joy (49:38):
In the low drinkers, interesting. I’m a self-diagnosed high drinker. Anybody who knows me knows that I usually have (if I’m at a restaurant) several beverages in front of me at any given time. And of course, I have my water right now that I’m drinking.
Is it possible for somebody to drink too much water or too much fluid? I remember hearing back in my clinical days that there were only two situations, and that was a certain medication that people were on that I don’t know if it made them want to drink more water or they wouldn’t have that signal in the brain to stop drinking water, and also maybe some psychiatric issues. But you tell me, is it possible to overdo it?
Dr. Stavros Kavouras (50:18):
So, I’ll give you two versions of the questions. So, the short one is no, and the evidence for that is when the dietary guidelines were published, they did extensive research and they specifically looked at this condition, psychiatric condition, it’s called psychogenic polydipsia, where people consume more than two gallons of water per day, either plain water or soda drinks, massive amounts of fluid.
And they found that even in those situations, there was no real threat to health. So, because of that, they did not establish what is called an upper limit, a UL in dietetics. So, there is no upper limit for water.
The European Food and Safety Authority that they published their guidelines, they said no more than 10 liters of water per day, which is two and a half gallons. And one thing that I can tell you if you are drinking more than even close to a gallon per day, there will be a lot of peeing involved. So, you’ll be going to the bathroom very often.
And I like to say this is a feedback mechanism. Your body has already a built-in metering system. When you pee every 20 minutes, you’re probably drinking way too much.
Melissa Joy (51:37):
There you go, unless you have a urinary issue.
Dr. Stavros Kavouras (51:39):
Yeah. So, the short answer is no. I know with some cases, and this is one of the things that quite often I get frustrated looking at people – there is so much communication on don’t over drink, and more often than you’re not drinking enough.
Melissa Joy (51:56):
Exactly, right. I hadn’t heard that.
Dr. Stavros Kavouras (51:59):
And sports, I’ll give you one example with numbers to get an idea of what it means. In sports, there is this condition in endurance sports and actually endurance to ultra endurance (so, marathon and up type of events) – there is a condition that’s called exercise-associated hyponatremia or water intoxication where you drink so much of non-sodium containing drinks that you sweat sodium, you lose sodium, you drink plain water. So, you dilute your body’s sodium levels.
And if you do that very quickly, your body cells swell. You see it in your rings, your rings get stuck, you cannot get them off. But when this thing happens in your brain, you get brain edema, you get lung edema – especially in the brain, you can die from that. So, it is dangerous. By any means, I would not recommend anybody to drink above and beyond what their body needs.
So, they did this study that was published in the New England Journal of Medicine, which is considered if not the number one, number two best journal you can publish. And they took marathon runners from the Boston Marathon, and they found that the high risk, the people that were high risk in developing hypernatremia, they were the people that they’re drinking so much that in a marathon race, they will gain 7 to 12 pounds.
Melissa Joy (53:24):
Wow.
Dr. Stavros Kavouras (53:25):
So, imagine how much drinking as a whole, when you run a marathon, you run 26 miles, and you gain 7 to 12 pounds in one race. This is like you have to be drinking above and beyond of what your body needs.
So, what they found in that study is that the high-risk runners develop exercise-associated hyponatremia or water intoxication, was the ones where they gain 7 to 12 pounds during a marathon race. So, can you imagine you finish a marathon – you start the race 170 pounds and you finish the race 182. I’m like how much drinking was involved in that race?
And imagine that you’re already sweating. So, you’re exercising and you’re sweating, you’re losing fluids as you’re going in the race, so you must be drinking so much. But for some reason that we really don’t know, even though you’re drinking so much, you’re not urinating enough to be able to excrete the extra fluids.
Exercise quite often competes – exercise is stimulus for antidiuretic hormone, and that hormone decreases urinary output. So, that could potentially contribute.
Melissa Joy (54:42):
To help protect your body from losing too much fluid through sweat.
Dr. Stavros Kavouras (54:47):
So, yes, it can happen. If you go crazy, if you start drinking like above and beyond, above your kidney’s ability to excrete extra fluids, there is a possibility that you can hurt yourself. But this is very difficult, and you really have to try very hard to do that.
Melissa Joy (55:06):
Yeah. Well, I’ve never heard a recommendation to not drink too much, and I also never thought about the eight by eight lack of scientific evidence to support that as a message that we don’t need to drink that much. That’s interesting.
We’ve talked about a lot of potential myths about hydration, is there any other myth or misinformation that you think is important to address before we wrap up?
Dr. Stavros Kavouras (55:37):
One of the things that I think beyond the don’t drink too much, that it’s quite an over advertised thing, is the drinking to thirst message, get people to drink whenever you’re thirsty. So, if we look at all this data of people that are not consuming adequate amount of fluids, it’s because when you ask them, they say, “I’m never thirsty, why should I drink? I’m not thirsty.”
So, if you wait to drink only whenever you’re thirsty, you’re not drinking enough. And what is interesting is this, when you look how your body produces the antidiuretic hormone that we mentioned earlier versus how your body stimulates thirst, it’s much more difficult to stimulate thirst than to start antidiuretic hormone.
So, what is happening, and what I’m trying to say (and this is I think the importance of the message with underhydration) is when you start getting underhydrated, when you’re not drinking adequate amount of water throughout the day, your body knows immediately. Your body produces antidiuretic hormone, so you’re not peeing much to prevent you from developing excessive dehydration.
But the problem is that your body doesn’t let you know that vasopressin is up. One thing that you can see is that you’re not peeing much, this is probably a simple thing to pay attention to. You’re not going to the bathroom much, and when you go to the bathroom, urine is very concentrated.
Melissa Joy (57:07):
Yes. So, can’t rely on thirst, and the color of your urine is an indication of your hydration status, and the frequency of urination. So, what should we be looking for, for those two things?
Dr. Stavros Kavouras (57:20):
Okay, that’s an excellent question. So, even though I’m a very geeky scientist and I love to do experiments in the laboratory and measuring biomarkers and trying to find the molecular mechanism, I think it’s very important to identify simple kind of like home-based assessments that normal human beings can do.
So, we thought of exactly those two things. So, how often you go to the bathroom and how dark is your urine. So, we know that both of them independently, you can do one or the other. And when you look at those independently, they’re not perfect, but they give you a good idea of how well hydrated you are.
But this is what we did – people that we collected 24-hour urine samples from them, we had hydration biomarkers from urine and blood, and based on biomarkers, we classified them whether they were well hydrated or not. And then we tried to find how many times they were peeing and how dark was the urine. So, this is what we found.
We found that if you pee at least six to seven times per day, and if your urine is more like straw color, what I like to say more like lemonade and less like orange juice or apple juice, then the possibility of being optimally hydrated, it’s almost 100%. So, it’s a very accurate way when you combine both of those.
And the six to seven times throughout the day., if you look at it, how many hours we are awake, and you do the math, this is approximately you have to pee every two to three hours. If you wake up in the morning, say you go to the bathroom and then you go to work, and you sit in a desk until noon and you haven’t been to the bathroom, you’re not drinking enough.
Melissa Joy (59:03):
Or like my children who don’t go to the bathroom at school the entire day, that’s not good (laughs).
Dr. Stavros Kavouras (59:11):
Exactly. This is another story. This is how environment impacts your behavior. When I’m on a plane for a long flight, and if I have window seat, I intentionally try not to drink that much-
Melissa Joy (59:25):
Fluid restrict.
Dr. Stavros Kavouras (59:26):
Because I don’t want to bother the people to go to the bathroom every couple hours. So, it’s the environment. If the restrooms are not close to your office, if the restroom is not very clean, if things happen in the kids’ bathroom in school and they don’t want to be there.
So, it’s quite normal for kids to change their behavior. So, I am not going to drink enough so I don’t have to go to the bathroom, so I don’t have to deal with the kids that are in the bathroom that do crazy things when I’m there.
Melissa Joy (59:54):
And we know seniors do this a lot with fluid restriction too. So, as we’re wrapping up, are there some best ways to hydrate or rehydrate, or any other tips we should know to do at home?
Dr. Stavros Kavouras (01:00:00:09):
I think the indication, what I mentioned earlier, the times, it gives you a good idea. An important thing, I mean, most of the time when I talk about hydration, people think drinking only plain amount of water. So, drinking plain water, which many people don’t like plain water.
Dr. Stavros Kavouras (01:00:25):
We have a lot of data in children, particularly, we know that one in four children in the United States do not consume plain water at all. They don’t like the taste of plain water. They find it boring, they just don’t like it.
So, can you find ways where you have some options of something that tastes better than water? Is that adding a little bit slices of fruit or adding a little bit of natural juice that you can mix? Of course, we don’t want every time that you need to hydrate to consume 40 grams of sugar with every glass of drink that you are consuming, of course.
So, I think lately, there have been many options of low sugar content that they taste good. And whether bubbles work for you, you like sparkling water, you want some flavor in there, I think that might help you to stay better hydrated.
So, find what works for you. Try different things, experiment. It’s not that difficult. It’s not much cooking. Some people like slices of cucumber, strawberries, lemon, it’s lemon and lime. It’s some of it or slices of fruits.
Melissa Joy (01:01:37):
Very good. Back in the day, we didn’t carry water bottles around with us all the time. I was a ballet dancer and maybe once during the day, we’d go to the water faucet, and the drinking fountain and get some water. So, at least, we’ve got our water bottles we can take with us.
But yeah, and I’m a bubbles person, so that works for me. But yeah, I like that suggestion to just find a way to make it a little bit more interesting and make it a habit. Work it into your schedule.
Dr. Stavros Kavouras (01:02:04):
There are also other options with electrolytes, adding electrolytes in your drinks. You don’t have to drink all day electrolytes obviously, but adding some electrolytes in your drink might make it more palatable, and also, it can maintain thirst for a little bit longer.
So, when you consume electrolytes, then your desire to drink more fluids, it’s prolonged versus if you drink just plain water. So, for people that are difficult and people that they don’t drink or people that they have massive fluid losses, they’re very physically active, they work outside in a warm environment and they need extra ways to hold that water, then that might work well as well.
Melissa Joy (01:02:45):
Yeah, I was going to ask you about that for people who tend to sweat a lot more too. I had heard, it sounds like you’re reinforcing this or even have a salty snack with the water would help you retain some of that fluid, right?
Dr. Stavros Kavouras (01:02:58):
Yeah, that’s important. Sweat is not extremely salty, but you lose significant amount of sweat. So, I see the workers here in Phoenix in the summer, especially roofers and people that work for the electricity companies, that they’re all day out running around in the heat. There’s not enough to drink to be able to stay hydrated.
Melissa Joy (01:03:19):
Yes. So, the electrolytes you’re talking about, there’s a lot of products out there, there’s sports drinks. I interviewed a sports dietitian, Nancy Clark a while ago, and she shared a homemade sports drink recipe, I can put that in the show notes.
But I’m trying to think of products that you can add to water, the electrolytes, there’s all kinds of products out there these days.
Dr. Stavros Kavouras (01:03:39):
I think those are helpful, especially when you’re physically active. And Nancy actually, who’s a good friend of mine, Nancy Clark is one of the probably most famous worldwide, one of the most famous dietitians.
Melissa Joy (01:03:51):
Yes, yes.
Dr. Stavros Kavouras (01:03:53):
And I’ve seen her recipe before, which is a great recipe and it’s a ballpark idea of what you need to take when you are exercising.
But one of the things that we have to keep in mind is that sport drinks are specifically developed with many, many things in mind. It’s not as simple as it sounds, like, “Oh, you just put 6% sugar, you put, I dunno – in a quarter of water you put 60 grams or quarter cup of sugar, and that’s it, and you make it taste good.”
Robert Crane was the person who suggested first the process that your body hydrates by ingesting sugar and sodium together. And there is a cotransporter, it’s called SGLT-1 (Sugar Glucose Cotransporter) in your GI system and on and on and on. And we’ve been stuck since 1960 that everything on hydration is only SGLT-1. There is a lot of stuff that we’re still learning.
There are amino acids that can impact hydration, there are different carbohydrates, low glycemic index carbohydrates or resistant carbohydrates that they don’t spike your glucose, but they can help to hydrate better.
Melissa Joy (01:05:03):
Interesting.
Dr. Stavros Kavouras (01:05:04):
There are a lot of things actually that many people – and actually, we do studies like that in my lab, and we’re presenting some data. This summer in the American College of Sports Medicine, we will be presenting some new and exciting from one of the studies we did.
Melissa Joy (01:05:19):
Very good.
Dr. Stavros Kavouras (01:05:20):
So, yes, this is a ballpark, you can make your own at home. If you’re an elite athlete and you want to have the best and the greatest, I think there is a lot of room to improve.
Melissa Joy (01:05:28):
Excellent. This is all very interesting. I will stay tuned to maybe have you on again to talk other things beyond this just hydration conversation.
People can follow you on social media, you’re on LinkedIn, Instagram, Facebook, Dr. Hydration is your handle. And you also have a website that I’ll link to in the show notes. Is there anything else you wanted to share as we’re wrapping up here?
Dr. Stavros Kavouras (01:00:05:52):
Staying hydrated and drinking more water might be probably the easiest thing you can do to improve your life and feel better.
Melissa Joy (01:06:00):
Excellent, thank you so much. And for everybody listening, if you like this episode, please share it with a friend. Check out other episodes, tell all your friends and family about the podcast. And as always, enjoy your food and beverages with health in mind. Till next time.
[Music Playing]
Voiceover (01:06:21):
For more information, visit soundbitesrd.com. This podcast does not provide medical advice. It is for informational purposes only. Please see a registered dietitian for individualized advice.
Music by Dave Birk, produced by Jag in Detroit Podcasts. Copyright, Sound Bites, Inc. All rights reserved.
LISTEN, LEARN AND EARN
Listen to select Sound Bites Podcasts and earn free CEU credits approved by the Commission on Dietetic Registration (CDR) for registered dietitian nutritionists and dietetic technicians, registered. Get started!
Get Melissa’s Sound Science Toolkit here!
Partnerships:
Sound Bites is partnering with the Association of Diabetes Care and Education Specialists (formerly the American Association of Diabetes Educators)! Stay tuned for updates on the podcast, blog and newsletter!
Sound Bites is partnering with the International Food Information Council! Stay tuned for updates on the podcast, blog and newsletter!
Sign up for my monthly newsletter and episode eblasts so you never miss an update!
Listen on Stitcher (Android)
Install the Stitcher App
1. Search for “sound bites with melissa joy dobbins” 2. Choose Play Current Episode or Add to Playlist
Choose “Play Episode”
Subscribe & Review on iPhone
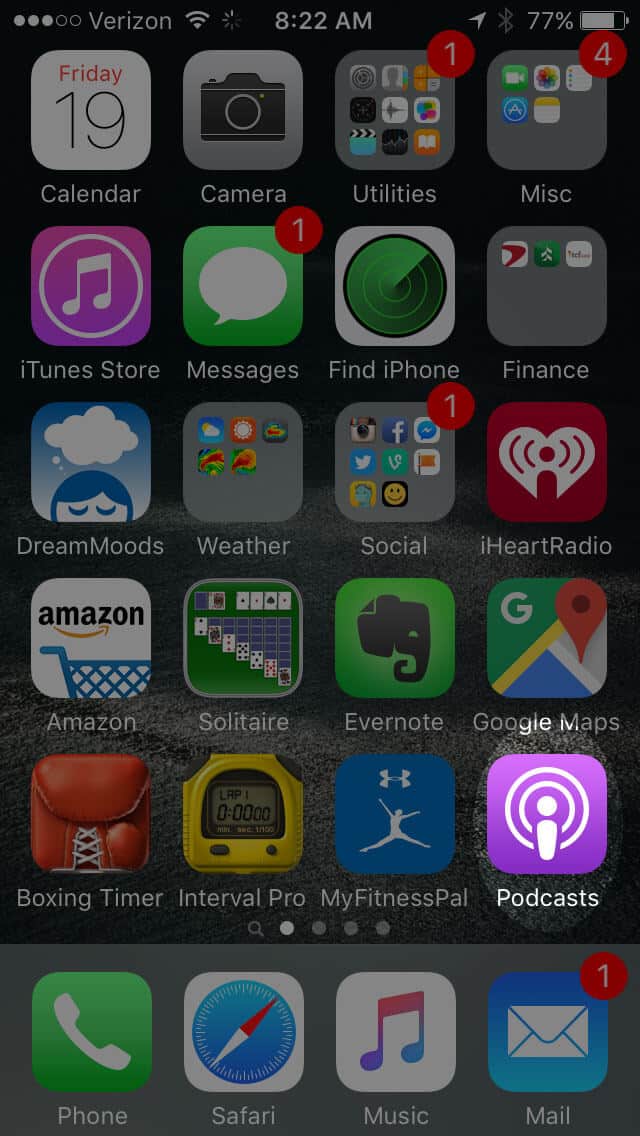
Open the “Podcast” app on your iPhone
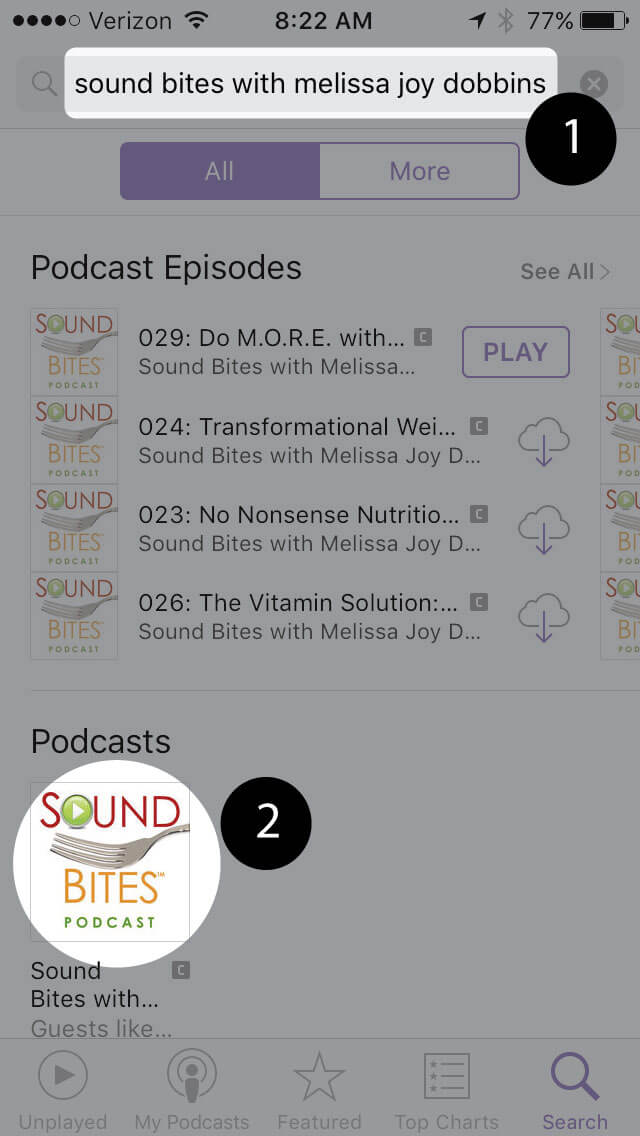
Search for “Sound bites with melissa joy dobbins”
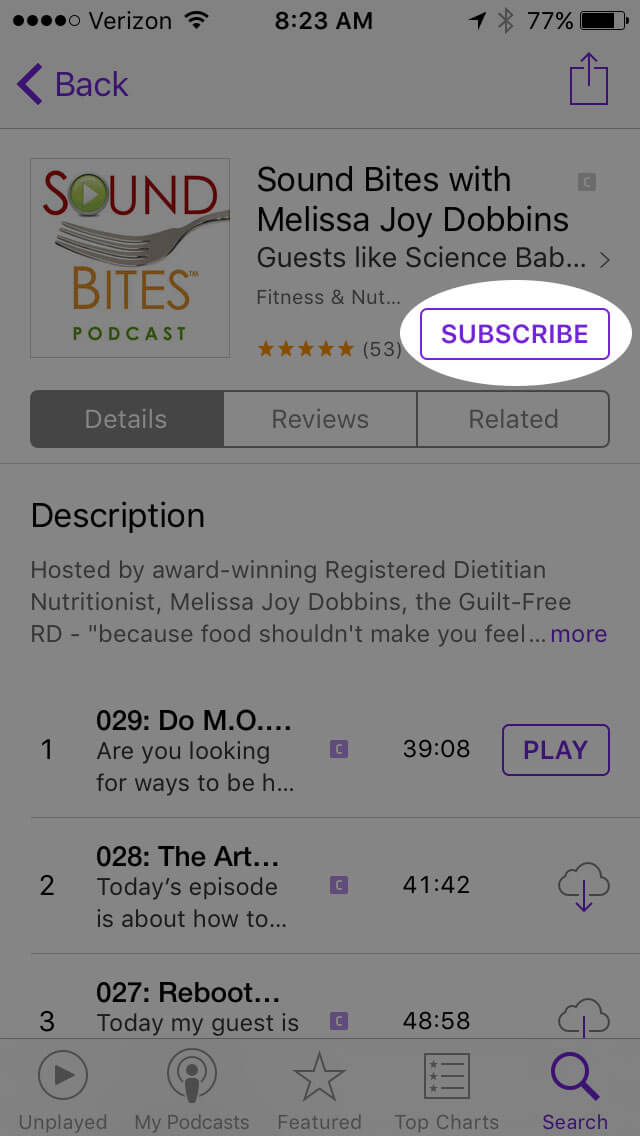
Open the podcast and click “Subscribe” and your done!
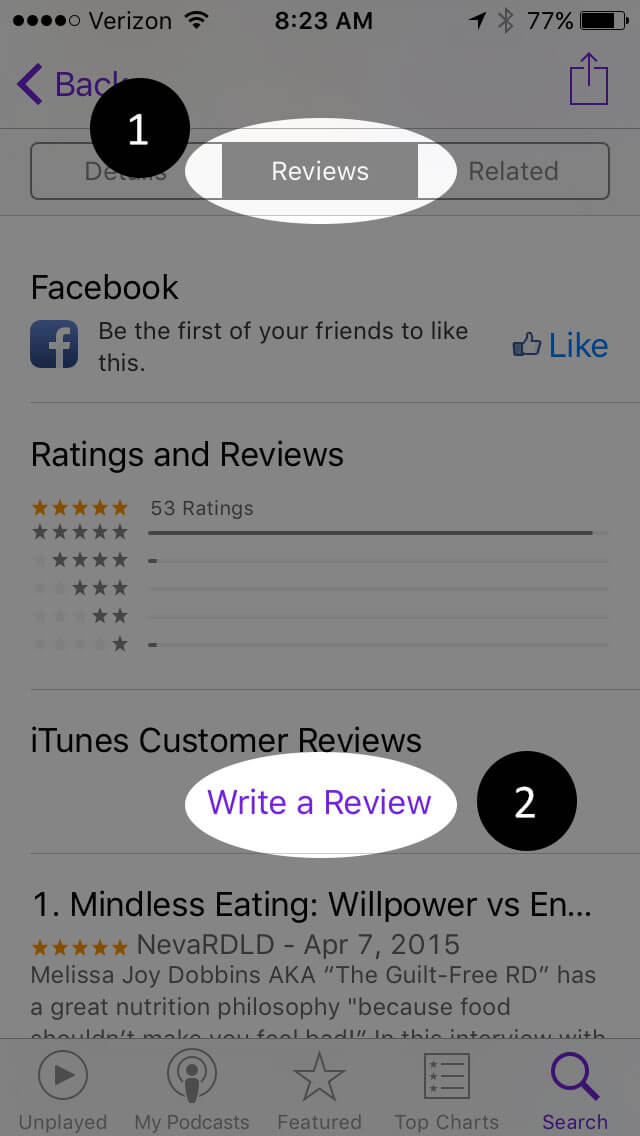
Write a Review
Click “Reviews”, then “Write a Review”.
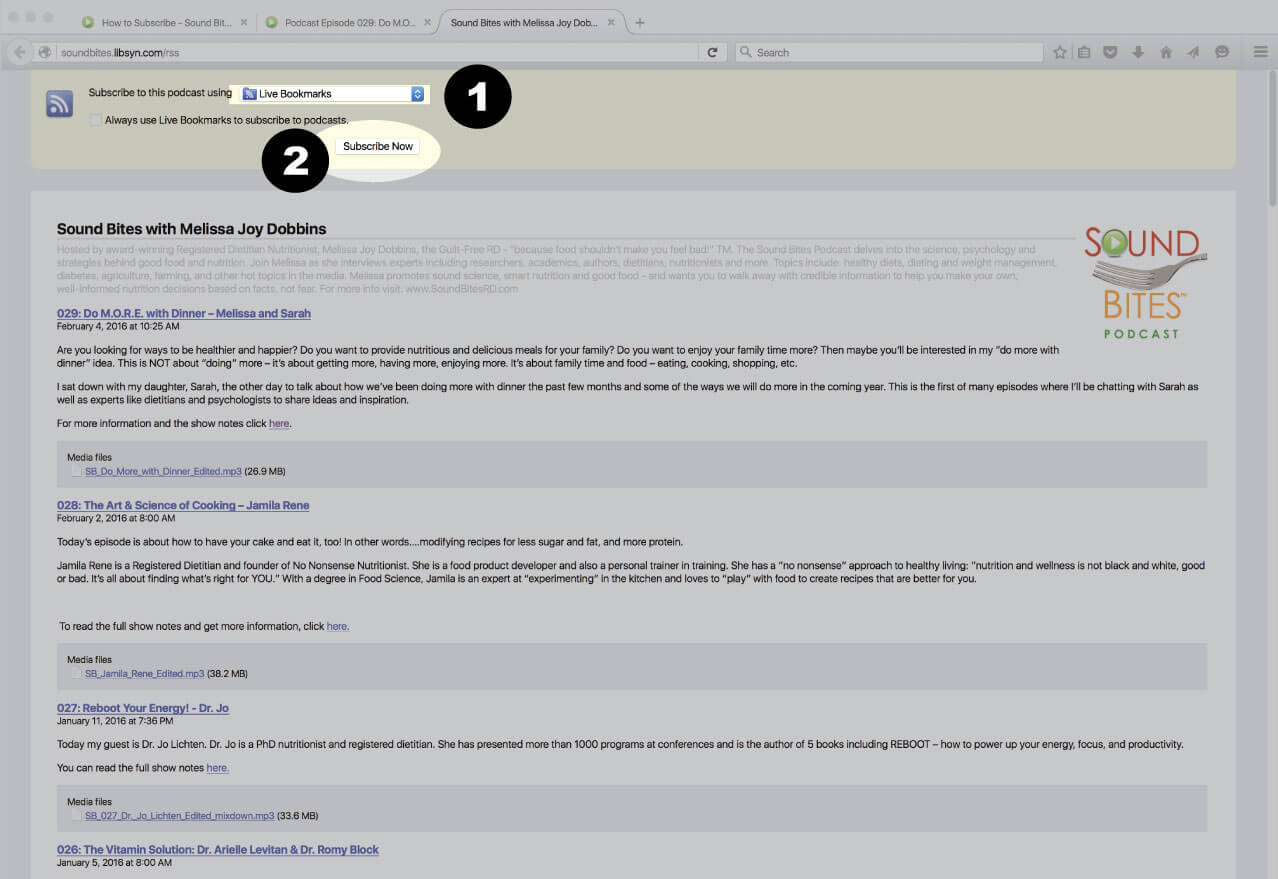
Subscribe via RSS Feed
Navigate to any podcast player . Click on the RSS feed icon.
Click on the RSS feed icon.
Click on RSS Feed
Choose which application you would like to use to receive the RSS feed
Click “Subscribe Now”
Confirm settings and subscribe.
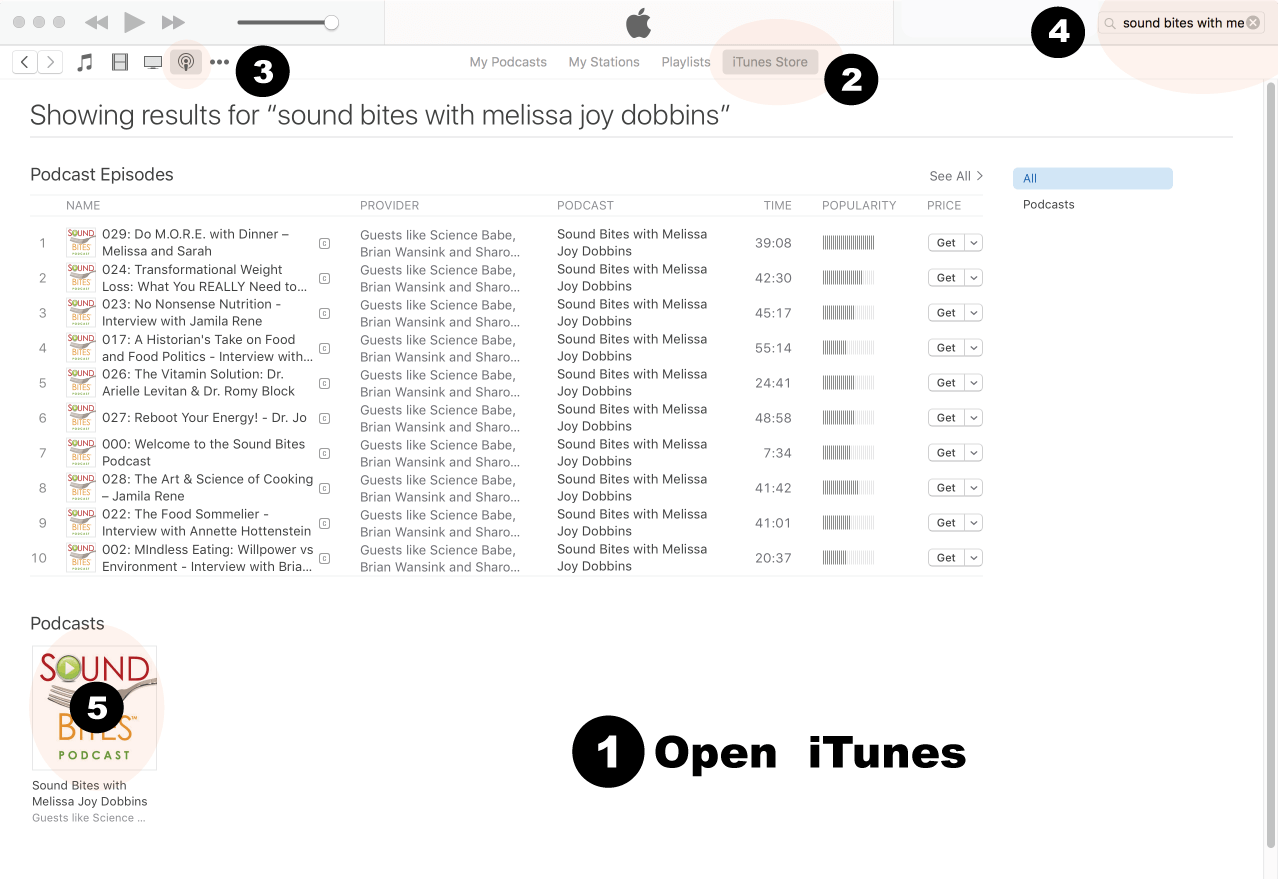
How to Review in iTunes
Open iTunes desktop application
Click iTunes Store
Click on Podcasts
Search for “Sound bites with Melissa Joy Dobbins”
Click on podcast image
Search for Sound Bites podcast in iTunes
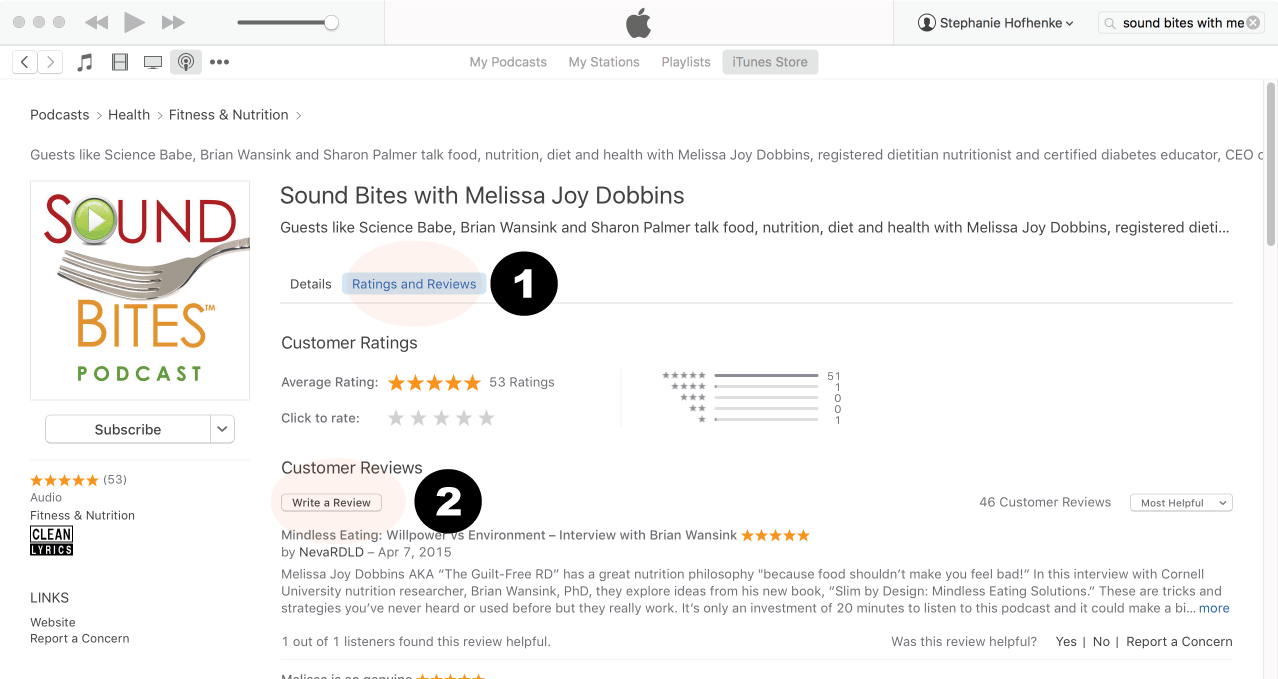
Click Ratings & Reivews
Click Write a Review
View reviews and write your own review.
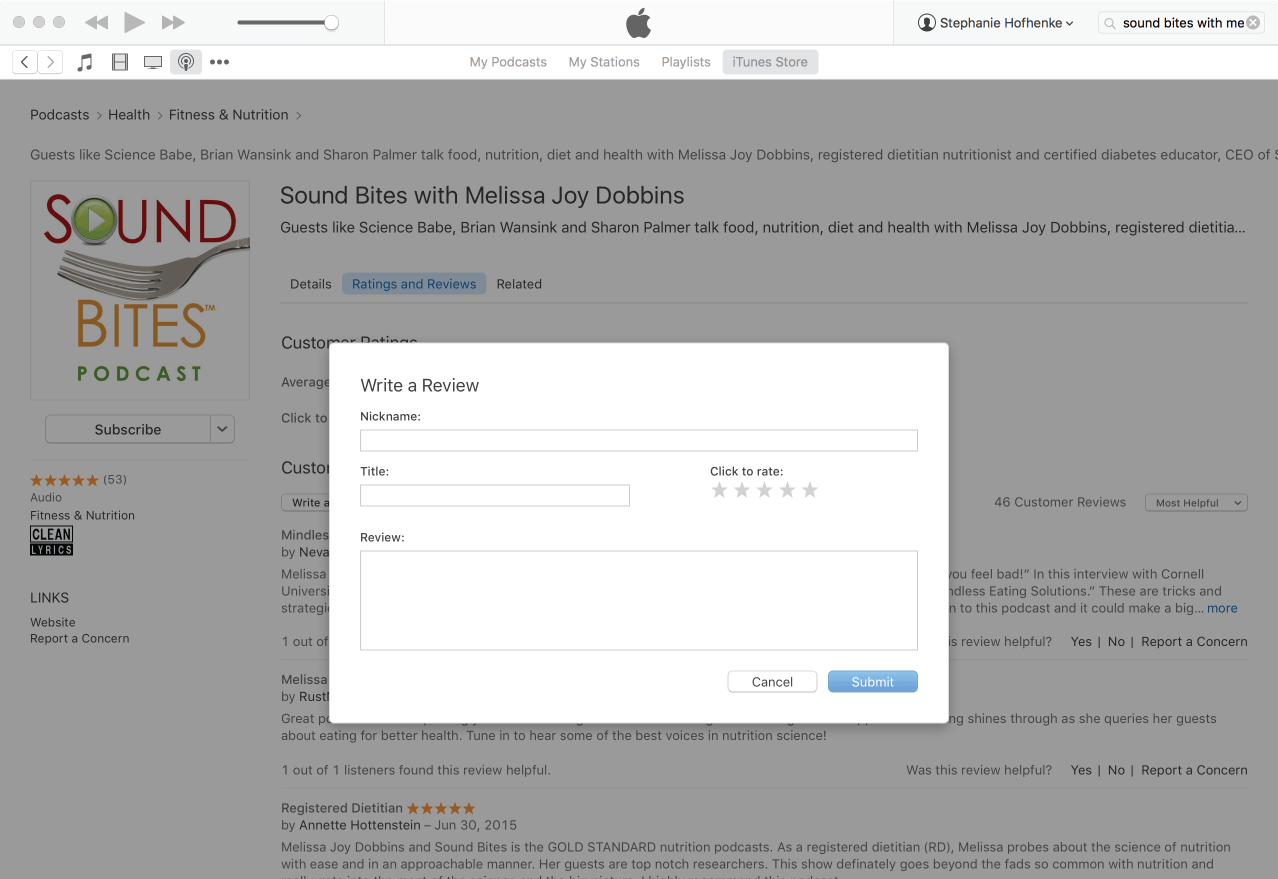
Write your review…. Thank you!
Write your review!
How to subscribe via iTunes
Click here to view the Sound Bites Podcastin iTunes, then click the blue “View in iTunes” button. This will open your iTunes application directly to Sound Bites Podcast. Click the “Subscribe” button, and your done!