Celebrating over 1 Million Downloads and 50,000 Free CEUs on the Sound Bites® Podcast | NEW: Get 1 years’ worth of CEUs with the new 15-CEU Podcast Course
Click here to earn 1.0 FREE CEUs for listening to this podcast episode!
Disclosure: Commercial support has been provided by Simply Good Foods. Dr. Jim Painter was sponsored by an unrestricted grant from Simply Good Foods to speak on the podcast. No products or brands are discussed or promoted.
“Low” Carbohydrate Diets and Metabolic Health: What Does the Research Show?
Lower carbohydrate, higher protein and higher fat dietary patterns have seen a resurgence in interest in both the research community and in popular culture in the past decade. This has been accompanied by a clearer understanding of who may benefit from dietary patterns that reduce carbohydrate and increase other macronutrients and the ways in which these approaches change human metabolism to facilitate weight loss and improve glycemic control.
While often regarded as fad diets, there is a significant amount of clinical evidence that can be used to evaluate the potential upsides and downsides of these types of dietary approaches. This research can be leveraged to understand what dietary factors should be considered when trying to optimize lower carbohydrate diets and how other macronutrients need to be shifted in order to provide sufficient nutrition. It should be noted that there is a large body of evidence that can be used to help answer many of the outstanding questions related to carbohydrate reduction or restriction. Furthermore, this large body of clinical research has resulted in many high-quality meta-analyses that help give a clearer picture of the utility of such alternative dietary patterns, especially regarding improving glycemic control in those with type 2 diabetes.
Tune into this episode to learn about:
Research studies on low/lower carbohydrate diets and metabolic health
Research related to diabetes, prediabetes, inflammation
How “low carbohydrate” is defined in various research studies
Ketogenic diet research
Higher protein and fat intake related to lower carbohydrate diets
Popularity of higher protein diets
How the quality of carbohydrates, protein and fat may impact health
Intermittent fasting research
Insights on ketosis, autophagy
diabetes remission
the “best” diet(s) for diabetes
2025 Diabetes Standards of Care
If the Mediterranean diet can be considered low carb
Potential health benefits with or without weight loss
resources for health professionals and the public
Jim Painter, PhD, RDN
Dr. Jim Painter is an Adjunct Professor at University of Texas School of Public Health, Professor Emeritus from Eastern Illinois University, and MS in Integrative and Functional Medicine program director at John Patrick University’s Lifestyle Medicine program. His research specialties include heart disease and mindless eating. Jim has been an advisor for Sun-Maid Raisin Growers and Paramount Farms, and consults for the National Dairy Council. He worked for Marriott Corporation in the 1980s, taught at University of Illinois during the 1990s and at Eastern Illinois University until 2013. Jim has over 100 peer reviewed publications to his credit.
Resources
Some links may be affiliate links. As an Amazon Associate, I earn from qualifying purchases.
Welcome to Sound Bites, hosted by registered dietitian nutritionist Melissa Joy Dobbins. Let’s delve into the science, the psychology and the strategies behind good food and nutrition.
Melissa Joy (00:23):
Hello and welcome to the Sound Bites Podcast. Today’s episode is about protein intake and low carbohydrate diets. What does the research to date show regarding diabetes, pre-diabetes and metabolic health overall with regard to the potential benefits of lower carbohydrate diets.
This episode is sponsored. Commercial support has been provided by Simply Good Foods and we thank them for their support of the podcast. Also – today’s guest, Dr. Jim Panter, was sponsored by an unrestricted grant from Simply Good Foods to speak on the podcast
However, we are not discussing any products or brands today.
We are submitting this to the Commission on Dietetic Registration for one free continuing education unit for dietitians, diet technicians and diabetes educators. So, if that is of interest to you, please check that out on my free CEU page at soundbitesrd.com.
My guest today is Dr. Jim Painter. Dr. Painter is director of the Master of Science in Functional and Integrative Medicine at John Patrick University and Emeritus Professor at Eastern Illinois University. He earned a BS in nutrition from Southern Illinois University, which is my undergraduate Alma Mater, and he earned his Master of Science from Oklahoma State University.
He got his PhD from the University of Illinois and he’s also a registered dietitian nutritionist. His research specialties include heart disease and mindless eating, and he has over 100 peer reviewed publications to his credit. Welcome to the show, Dr. Painter.
Dr. Jim Painter (01:54):
Well, I’m glad to be here, Melissa. It’s been a while since we did this and it’s much improved.
Melissa Joy (01:59):
(Laughs) thank you, yes. So, Dr. Painter, you were I think guest number three when the podcast launched 10 years ago. So, yeah, it’s been a minute, so welcome back. It’s always good to talk with you. Oh, actually it was episode number four, I’m looking at my notes here.
So, it was April of 2015. So, we’ve known each other for about 20 years, I think, because I know we did at least one presentation together way back when I was working with the Dairy Council. We did this cheese and wine pairing at this winery out in the western suburbs of Chicago. It was so much fun.
Dr. Jim Painter (02:35):
Yes, it was.
Melissa Joy (02:38):
(Laughs) yes. I mean, time flies. So, I would love for you to share more about your background and the work that you do with our listeners and any disclosures that you have to note.
Dr. Jim Painter (02:50):
So I kind of started out working at, it was kind of like a new hospital in Tulsa, Oklahoma and I did that for 10 years and then I really enjoyed the teaching part of it, so I thought, “I need to get a degree.”
So, I got a master’s degree accidentally over a 10-year period from 1980 to 1990. It took a long time because you have a baby and stop and start and have a baby and stop and start. So, it took me nine years to get a master’s degree. It wasn’t the most prominent thing in my life.
So, I did that for a while and then I thought I’d really like to teach. And so, went to University of Illinois and taught there for more than 10 years. And after that I finally got a PhD while I was there and went down to Eastern Illinois and was the chair of the Department of Family and Consumer Sciences for about 13 years, I think.
And then stopped that in 2015 and started traveling and just speaking until COVID came in January 2020. One of my assistants said, “Get back on LinkedIn.” So, I did. I was only on for about a week, someone called me and said, “Hey, you want to run our master’s program in functional integrative medicine?”
So, I started that and it just flipped from traveling the country to sitting here looking out over the ocean on a South Padre Island and teaching classes.
Melissa Joy (04:25):
Excellent. Well, I’m just thrilled to have you on the podcast. This topic is very popular and I think there’s a lot of questions about increasing protein intake, decreasing carbohydrate intake, there’s a ton of things that we could talk about.
So, you and I kind of had a pre-interview call where we kind of put our heads together and both of us have a bunch of research papers in front of us. So, we are going to get into some science but also of course make it digestible for our listeners, which you always do a great job of it, always throwing in a side of humor as well.
Maybe the best place to start is when we talk about low carbohydrate diets or lower carbohydrate diets, what exactly do we mean? Is this term defined? I think this is an important place for us to begin this conversation.
Dr. Jim Painter (05:17):
You know it is, and everybody has their different idea. So, when you say low carbohydrate, you can just as well say high fat, high protein (laughs) because it’s the same thing.
If you take carbs away, you’re going to eat fat and protein. A low carb diet and people think it’s a keto diet, it really is not a keto diet.
A keto diet is really low, it’s like a carnivore diet. Carnivore diet is like zero grams of carbohydrate. You’re just eating meat, fish and eggs. And then the actual ketogenic starts at about 10%, maybe 50 grams of carbohydrate or less. So, generally it’s less than 10% of calories from carbohydrates and then you go up from there and then it’s just kind of a low carbohydrate diet. A low carbohydrate diet, whether it’s really low, medium or just low can be 150 grams of carbohydrate.
People go, “Really?” Yeah, because we’re eating 200 to 300 (laughs) grams of carbohydrate a day and so just cutting it down. There’s an amazing benefit in just reducing carbohydrates a little bit from the massive amount we eat to having more fat and more protein, does all kinds of great metabolic things in our body.
Melissa Joy (06:50):
Yes. We’re going to dig into that. I did want to share that the AMDR, the acceptable macronutrient distribution range for carbohydrate is 45 to 65% of daily caloric intake and the recommended dietary allowance or RDA is 130 grams of carbohydrate. So, yeah, to your point, kind of like sodium and other nutrients, we’re getting a lot more than that probably.
So, I imagine some of the different studies that we’re looking at here, I’ve noticed some studies define a low carbohydrate at this level or very low carbohydrate at this level. So, let’s touch on that as needed as we go through but thank you for kind of setting the stage there.
So, low carbohydrate, very low carbohydrate, ketogenic, what level of carbohydrate intake, and maybe I’m putting the cart before the horse here, but we’re going to talk specifically about studies, but what level of carbohydrate intake do you think is realistic or sustainable? Something that you can stick with long-term and maybe that’s something that isn’t necessary, maybe some of these lower diets do serve a temporary purpose.
Dr. Jim Painter (08:02):
I think they do. So, on the temporary purpose side, people can eat carnivore and eat no carbohydrates at all for a period of time. And it’s metabolically very beneficial because blood sugar drops, lipids drop, it’s just a fantastic diet but maybe for a couple of months. And so, it is short-term, but if you talk about ketogenic, less than 10% of the calories, jeez, I’ve known a thousand people that did it and quit.
But there are a few people that are just been on the ketogenic diet for 10 years and I know some children because some diseases of children that have like epilepsy or they have seizures, they’ll go on a ketogenic diet and they just quit. So, if they’re a kid and you can go without all these episodes by eating less than 10% of your calories from carbohydrate, you do it and you’re happy to do it.
So, people that definitely need it can do it for a long time. People that just are trying it, I know lots that didn’t stay on it. I do have some friends that are just loving the ketogenic diet and probably about 10% carbs or less and they’re doing great on it.
I have a friend who dropped so much weight on a ketogenic diet and he did it for a year or so and then he got off it and he went back to eating it and he came to me almost crying. He said, “I can’t get into ketosis anymore.” I said, “Sure you can, quit eating.”
“I don’t want to quit eating (laughs).” If you really want to get that little stick in your urine to show you’re ketogenic, then don’t eat. And if you fast you will be ketogenic but your body adjusts after a while in a ketogenic diet, our bodies are able to make glucose better. And so, it’s harder to get into ketosis sometimes for people that have done it in the past.
So, what’s the best level? I don’t know. Americans are 70% either obese or overweight. Really? Yes. The whole country is, so generally for most American humans that are eating too much and they’re overweight, something like a low carb diet and then tend to be super low, you can be down at 120 grams and get amazing benefits from just eating less carbohydrate.
Melissa Joy (10:09):
Yeah. So, that was a lot. I do want to point out that you mentioned the children and the epilepsy and a lot of our listeners may not know that that is the origin of the ketogenic diet and it is a medically supervised diet. It’s a thing, it’s not just a fat diet type thing.
So, following up on some of what you said then it just reminds me of we always talk like the only diet that works is the one that you can stick with.
So, whether it’s vegan, carnivore, somewhere in between, different strokes for different folks. Like some people are happier on one end of the spectrum or in the middle but we’re going to talk about the metabolic effects of this. You also said when we decrease our intake of carbohydrate, well, we’re going to increase our protein and/or fat to some extent.
I mean if it’s a weight loss diet, we are probably looking at a lower caloric intake to begin with. And so, percentage wise though, let’s say we just decrease our excess carbohydrate intake, percentage wise, we’re going to get more protein and fat, but it may not actually be that we’re eating more of those things. So, there’s a lot of different ways to look at that.
So, having said that, how much protein and fat make up the rest of the diet of a lower carbohydrate diet? I mean I think we’ve kind of already answered that for ourselves, but I wanted to make sure that you can address that like how much protein and fat would be considered in a lower carbohydrate diet.
Dr. Jim Painter (11:38):
And so, when you’re talking about low carbohydrate and people think keto, that’s 10% and that’s not the norm. You don’t need to be keto to get these benefits. But then you still have 90% of your calories, so what’s going to go up? Protein can’t go up too much. It can go up to 25% maybe. So, you’re really eating more like 70% fat (laughs) and people go, “Really? Is that good?” Yes, it is.
The Mediterranean diet, which is the wonderful diet for the world, is almost 50% fat. Really? Yes, it is. It’s 50% fat generally. And so, the combination of those two, it depends what your goal is. It’s hard to get a zone diet, 40% carbs, 30% fat, 30% protein. We did that in a scientist experiment one time 30 years ago.
To get 30% of your calories as protein, you can’t hardly eat and have only 30% fat because you’re going to be eating meats, they’re full of fat. And so, we had turkey for breakfast, turkey for lunch and turkey for dinner.
Melissa Joy (12:41):
A lot of lean protein in order to keep the fat at 30.
Dr. Jim Painter (12:45):
You just can’t hardly do it, eat nuts. Nope, can’t have nuts. It’s because of the fat. So, it will turn out to be probably double the amount of fat as protein and which is fine because that’s still pretty high protein and it’s high fat also.
Melissa Joy (13:00):
So, I’ve done a lot of podcast episodes on protein and I will link to those in the show notes for any of our listeners who want to dial back and check those out. But as we’re saying we’re decreasing carbohydrate, low, lower carb makes sense that we’re doing high or higher protein intakes. What are some of the reasons that people are so interested in protein and getting more protein? I mean it’s all the rage. What benefits are people looking for and/or receiving from increasing their protein intake?
Dr. Jim Painter (13:30):
Forever the people that are exercising, you’d always see these guys are lifting weights and they’re eating steak and eating eggs. And he’s doing great on it. And so, it’s always been to get more muscle mass, you need to eat muscle, you need to eat amino acids to be able to build muscle and so it does do that.
The thing is, is the muscle builders I don’t care about, I care about the little lady that I was talking about (laughs) that doesn’t get enough protein and she has no muscle. She’s bone and she’s skin and she weighs about 92 pounds. And for those people, building muscle is a key because Sarcopenia, you lose it. You don’t have it as you get older and you need it. So, protein is great for building muscle and it does.
But now we’re finding out that really higher protein, lower carb, it’s easier to lose weight. You just lose weight more by just having less carbohydrate and more protein and fat. So, weight loss has become an important issue too but it does a lot of things metabolically.
Your body functions better when you’re eating more protein, it’s good for your metabolism, just eating more protein. So, this is a variety of things that proteins do and I think it’s a good idea that people are trying to get the right amount of protein.
Melissa Joy (14:49):
What do you say, because I hear this all the time. So, what do you say to people who say, “We are all getting enough protein.” Americans eat enough protein or too much protein.
Dr. Jim Painter (14:59):
And that is true for some middle aged, overweight American adults. It is true, but children, they don’t always, older adults, they don’t always and you have to work with that. And even young women, they’re on a vegan diet in their bone building years from 15 to 25 and they’re not getting enough protein. It’s difficult.
So, there’s pockets of people in the United States, large pockets of people that don’t get enough protein.
Melissa Joy (15:42):
Depends on the population and the person. So, you mentioned vegan, there’s plant-based proteins and I have several episodes that address plant versus animal proteins. So, we don’t need to take a deep dive on this, but does the quality of protein matter, should I say the type of protein matter plant-based versus animal-based?
Dr. Jim Painter (16:02):
It does, and this has been common knowledge forever that plant proteins are not complete. You don’t get all the compliment of the 20 or it’s really only about 10 that you need amino acids. And so, you can eat less of it and get a better quality of protein.
I’ve just finished an article for the European Medical Association. It’s going to be published in about a week comparing dairy to non-dairy plant alternates and they just really don’t meet up. One of the things they just don’t have is protein.
So, you drink milk a lot of times for protein and they don’t have it. They got one gram, milk has eight and the gram that they have isn’t as good a quality of protein. So, you don’t even use all that little bit of protein you have.
So, yeah, the kind of protein makes a big difference and animal protein is better.
Melissa Joy (17:00):
Most of the plant-based milk alternatives have one gram of protein, like you said, like almond milk, rice milk, now soy is more comparable to cow’s milk, but all the rest. And people really need to check those labels and that’s something a lot of people don’t realize.
Before we jump into some of the specific research, studies and aspects that we’re going to tease out, I don’t want to wait too late to ask this question is what about fiber? Where does fiber fit into all of this? Most people are already not getting enough fiber in the large amounts or normal amounts of carbohydrates that they eat. So, how can we get enough fiber if we’re decreasing our carb intake?
Dr. Jim Painter (17:46):
That’s a good point. There’s a graphic I have that shows that when the food guide pyramid came out in 1980 that we had been decreasing carbs, at that time, people jumped on the carbs and what happened when they did, they weren’t eating the whole carbs. So, carbs went up but the fiber content went the same or went down bummer.
We pushed these carbs so much we didn’t push whole carbs and it’s so important to get the whole grain carbs where you’re getting it. You’re eating fruits and vegetables, eat the whole thing. So, the answer to that is eat whole foods because you get fiber in whole foods.
Melissa Joy (18:54):
And there are a lot of different sources of fiber but to your point, we can get most of our fiber from fruits and vegetables. The grains have some as well, but they’re not typically the higher fiber sources. But something like a carnivore diet, I don’t think since you’re not getting any fruits and even a piece of lettuce hardly with that diet, I don’t think you’re going to get your fiber.
But for other diets like keto or somewhere in between, I think, you can try to get more fiber from the fruits and vegetables. So, let’s talk about the research. What does the research to date show regarding the potential benefits of low-carb diets? Where should we start?
Dr. Jim Painter (19:37):
The one I’d like to start with is by Bazzano in 2014. I remember when it came out, I was depressed over it because it didn’t agree with what I thought. It compared the effects of low-carbohydrate and low-fat diets: it was a randomized control trial. And when I looked at it, one of the things I did expect was the fat free diet went down, the low carb diet went up by eating more protein. That was not a significantly different finding. I expected that. And then you look at LDL cholesterol, well it went up with the low-fat diet. Really? Yes. And it went down with the low carb diet. Both of those are not significant in findings. And so, the ratio of the good to bad cholesterol also improved with the low carb diet. And that was statistically significant.
So that is an amazing study and it was back in 2014. The thing that really got me, I know because the change was a 10-year Framingham risk score for dying of heart disease. it went up, really, it went up in three months, it went up substantially on the low-fat diet. It stayed up at six months, it stayed up at 12 months. Of all the things we could think of that would be a bad thing to happen with the low fat diet is that it made the 10 year Framingham risk score go up.
On the low carb diet, so we’re talking about death rates from heart disease, fats usually associated with it, but it’s really not. And so, if you eat a low carb diet that is very high in fat, it dropped at three months, it dropped at six months, they kept dropping at 12 months.
Which is odd because generally you get a J effect – with almost any diet – where it works for a while, works for 3 months, 6 months and by 12 months it’s not working anymore and that’s not what happened here. And this study was only 12 months long, it was still going down. (Laughs) this is just sad, the chance of diet on a low-fat diet was higher than a low carb diet that is full of fat and high in protein.
Melissa Joy (21:19):
And I have this in front of me. This particular study defined a low carbohydrate diet is less than 40 grams per day. So, would you consider that ketogenic?
Dr. Jim Painter (21:30):
Oh yeah, that’s getting down to the ketogenic area. So, it is ketogenic. And so, I understand they wanted to do this in this study 10 years ago. They wanted to get the biggest effect and by going ketogenic they got the biggest effect.
Melissa Joy (21:41):
Yeah, that’s an interesting point. What have you seen in other research; how low do we need to go to start seeing some of these benefits?
Dr. Jim Painter (21:51):
Most of the studies I’ve looked at over the past 20 years and a lot of the ones I have with me are just lower carb. They’re 120 grams of carbohydrate a day and it’s not trying to get down to 40 grams. So, just cutting back on the carbs is beneficial and you start to improve all those metabolic markers just by cutting down on it without going ketogenic, you still get the benefits.
Melissa Joy (22:15):
And I think it’s really important to touch on also, a lot of people think, well yes, with weight loss you’re going to see these better outcomes and improved outcomes but there’s research that shows you get these metabolic improvements even in the absence of weight loss. So, could you speak to that?
Dr. Jim Painter (22:33):
And that has been an issue from the beginning. And I remember in 1995 I was sending my students out every year compare the low fat to the low carb diet. They came back and said, “Doc, the Atkins diet one,” I said, “That’s impossible. The Ornish diet is low fat, it’s vegan, it’s got to do better.”
I sent them out semester after semester for five years and I thought, “What are you doing here, students?” They were coming back to me every time the Atkins diet is the one that’s working (laughs).
And so, I flipped my paradigm 30 years ago on this idea of what really works to reduce weight, to improve blood lipids, to reduce blood sugar, it was the low carb, high fat, high protein diet. And as I look at these studies, really they’re almost all, unless they’re saying they’re ketogenic, they’re looking at 120 grams of carbohydrate, which is a low carbohydrate diet.
Melissa Joy (23:25):
And a more reasonable amount than 40. So, let’s talk about diabetes. What does the research show regarding diabetes?
Dr. Jim Painter (23:35):
The one study, I have a lot of them here, but this first one is by Luo, it’s low carbohydrate, ketogenic diets, reduce cardiovascular risk factors for obese and overweight patients. Well, that’s what our country is obese and overweight with type 2 diabetes mellitus and it’s a meta-analysis, randomized control, it’s 21 studies (laughs) that that Luo looked at.
And it was amazing. Fasting, blood sugar went down significantly 0.000 and as you’d expect hemoglobin A1C, the long-term marker of blood sugar went down too, 0.003. And so, insulin went down significantly 0.000 and then HOMR is a risk of insulin resistance, it went down a significant at 0.015. So, it does many things besides losing weight. Weight, it does do, but it does these things in addition to the weight loss.
Melissa Joy (24:32):
And that was published in 2022, are there other studies? I mean this is a meta-analysis of RCTs, so I mean that’s pretty powerful. Are there other studies that you wanted to address with regard to diabetes?
Dr. Jim Painter (24:46):
Like I said, I started this with my students 30 years ago and they convinced me and now there’s multiple meta-analysis. How do you show something as settled science? Well, do a meta-analysis of 20 studies that all agree. Well, that’s good. But then if you keep getting meta-analysis because they keep showing the same thing, that is the proof.
And so, there’s a study by Ji and it came out 2024, it was last year. And the title is the effect of a ketogenic diet on inflammation related markers, systematic review, meta-analysis of randomized controlled trials, that’s what we want. Let’s see what these randomized controlled trials do. And so, meta-analysis are fun. I look at the forest plot where it shows this is it worked and on the other side it didn’t work.
And so, you can look at all the studies and see how significant is it. And so, this shows that C reactive protein, which is the first marker we use for inflammation, how’s your body doing? C reactive protein went down significantly. The P value was 0.000 in these, how many studies was it? I think it was 20 something studies.
I don’t see it right now, but it went down, which is amazing to me. And it wasn’t really consistent all the way. There were some studies that showed it increased but overall, it showed that it decreased significantly for C-reactive protein.
Melissa Joy (26:03):
As you know, I’m a certified diabetes care and education specialist and I have been for 27 years and I pulled out my book of the 2025 standards of care in diabetes. I have the book in front of me and I wanted to read some of the carbohydrate related information to address that this reduced carb intake is an acceptable approach from the American Diabetes Association perspective.
So first of all in chapter 3 which is: PREVENTION or delay of diabetes and associated comorbidities – it talks about Lifestyle Behavior Change for Type 2 Diabetes PREVENTION and one of the recommendations is “prescribe an eating pattern known to be effective in preventing type 2 diabetes to individuals with prediabetes. A variety of eating patterns such as the mediterranean style, intermittent fasting and low carbohydrate have shown benefit.”
Under the medical nutrition therapy section in chapter 5 which is facilitating positive health behaviors and well-being there are two tables on nutrition therapy recommendations and macronutrient specific recommendations such as
5.13 says “for diabetes prevention and management of people with pre-diabetes or diabetes recommend individualized meal plans that keep nutrient quality, total calories and metabolic goals in mind as data do not support a specific macronutrient pattern.”
So, individualized – we hear that all the time – and we know how important that is and just reinforcing there is no set specific macronutrient pattern so we have that flexibility to flex up or flex down on the carb amount as needed for individuals.
Another one is 5.15: “consider reducing overall carbohydrate intake for adults with diabetes to improve glycemia as this approach may be applied to a variety of eating patterns that meet individual needs and preferences.”
And just a couple more I want to mention. 5.24: emphasize minimally processed nutrient dense, high fiber sources of carbohydrate and it specifies at least 14 grams of fiber per 1000 calories.
In that same chapter in the section on carbohydrates it says:
For people with type 2 diabetes, low carbohydrate and very low carbohydrate eating patterns have been found to reduce A1c and the need for glucose-lowering medications. It also says that the wide range of definitions for a low-carbohydrate eating plan poses a challenge in interpreting carbohydrate-restricted research studies.
So, I just wanted to call those out specifically and see if you had any comment or anything you wanted to add to that.
Dr. Jim Painter (28:40):
I was just very glad to see when they specifically said low carb eating was recommended. I mean I thought about that in 1975 when I was starting into school and we would make plans for diabetic diets.
Okay, you get grams, grams, grams, two cookies here, three pieces of bread here, and you’d add up all this to 50, 55 grams of carbohydrate and no one ever talked about low carb diets, but they put it in there now and I’m happy to see it’s in there. And the other thing is they don’t really talk about sugar that much, they talk about whole food eating, which is another good idea.
Eat whole foods and it was a concentrated effort to look at sugars and just these really rapidly digesting starches. But even at that, this new guideline is to me wonderful by saying low carb’s important, by talking about whole foods, by not specifically talking about nutrients. And so, I like it. I like what they’ve done.
Melissa Joy (29:38):
Okay, great. What have you seen regarding pre-diabetes in the literature?
Dr. Jim Painter (29:44):
Many of the studies actually say that. They’ll say pre-diabetes, diabetes, and there’s not that many studies specifically on pre-diabetes. This is personal to me because I had pre-diabetes 50 years ago.
Melissa Joy (29:57):
Before they called it that.
Dr. Jim Painter (29:59):
(Laughs) yeah, before they called it that they tell us, “Yeah, you’re not diabetic.” “I don’t want to be diabetic, what can I do?” “No, come back in five years. We’ll look at it again.” I thought you’re joking. And so, the idea is, is generally, and it doesn’t work in every area of life, but with sugar metabolism, pre-diabetes and diabetes, the studies do the same thing to both. If you have pre-diabetes, it’s just a much smaller form of diabetes.
Melissa Joy (30:24):
Let’s talk about other benefits that we would see. You touched on inflammation and C reactive protein, what other benefits might we see, I mean we’ve talked about weight as well, but are there others?
Dr. Jim Painter (30:36):
Yeah, there’s many of them. And so, people talk about I lost weight and that’s great and I don’t really care if you lost weight but when you lose a weight, then your blood sugar goes down, just does every single time.
I mean, if my blood sugar was up, I think this is stupid, I’m just not going to eat now for, well 15 hours and then eat again and it’s down normal. But it’s not just that it’s triglycerides. You eat too much of anything, you get triglycerides.
And so, when you start changing your diet and you’re losing weight, just the fact of a body losing fat mass, muscle mass getting smaller, your blood lipids, triglycerides drop, LDL goes down, HDL sometimes goes up, sometimes it doesn’t.
But your markers of fat metabolism in your body change and long-term marker of blood sugar, hemoglobin A1C drops too when you just start changing the direction. I’ve been gaining weight for 55 years. Well, if you switch that and just start losing weight, you end up improving all of these metabolic indicators.
Melissa Joy (31:41):
Well, you mentioned not eating for 15 hours and that makes me think of intermittent fasting. So, not too long ago I did an episode on intermittent fasting or time-restricted eating and then I ended up actually submitting a proposal to FNCE, our annual dietitian conference for this researcher that I had interviewed Dr. Krista Varady, and the session got accepted and so I served as a moderator for that session.
We actually specifically addressed in this session more so than the episode that I did with her, the intermittent fasting or time restricted eating and diabetes. So, I was wondering if you had any comments or insights to share about intermittent fasting and what you’ve seen in the literature and how it might fit into our conversation today.
Dr. Jim Painter (32:29):
Well, we can begin now and we can stop after breakfast tomorrow morning. I have a PowerPoint slide with 350 different studies but I’m not share just one. (Laughs) it’s just one of my favorite ones and it’s called Impact of Intermittent Fasting on Health and Disease Process by Mattson and it was done in 2017.
I have questions all the time and people can’t answer my questions. I used to ask medical doctors, scientists, “What is it that causes you to go into ketosis?” Nobody knew. Really? And how does it happen?
I’d like to do a whole series with you just on getting into ketosis and what that does to your body in general, but also to autophagy, your body eating itself. But I found this study, it’s amazing by Mattson and it just shows that if you eat breakfast, lunch, dinner, and a snack throughout the day, how many ketones do you make? None. None? Yeah. None. Pretty much.
And then if you could say, “I’m going to eat today and not eat tomorrow.” So, you eat tonight and you don’t eat all night and then you don’t eat breakfast, by about 11 o’clock you start making ketones. And so, you make ketones all day, all night until you eat the next morning at six, you make a huge amount of ketones. But my question was, “Does intermittent fasting, time restricted eating, does it work?” And the answer was yes.
So, they also have a wonderful diagram. So, if your group out there is going to come to your site and get something, get the Mattson study, because it shows that at this day, they ate at two, five and eight o’clock. And so, they ate for a six-hour period and then they didn’t eat after that. So, midnight came, they didn’t eat breakfast came, they didn’t eat, then they quit eating at eight.
And so, by the next day, by about nine o’clock they started making ketones. So, they made it all day from 9 to 12:00 PM past noon to two o’clock, so for six hours they made ketones. And so, the answer to the question is, how long do you have to not eat before you start making ketones? At least 12 hours and 14 is better. From 14 to 16 to 18 hours, you just make ketones.
And if we could talk about something that’s wonderful, ketones do so much.
And so, I look at this study by Mattson and it’s amazing. It taught me that yes, if you don’t eat for a period of 12 to 14 hours, you start making ketones. So, you can make ketones every single day by just eating fewer hours of the day.
Melissa Joy (35:12):
And like I said, I mean I’ll link to that episode in my show notes as well. Just interestingly, and I think this kind of speaks to what we’ve touched on a little bit here, is I believe in the intermittent fasting research, the alternate day fasting had better results than the restricting daily windows of eating but the adherence was not as good long term.
Dr. Jim Painter (35:39):
If you’ve ever tried doing that, it’s hard. To eat one day and not eat the next, eat one day and not eat the next, the problem comes, it’s not in the day that you don’t eat, it’s the day that you eat.
You can’t eat enough. If you want to lose weight, just do that because you can’t eat enough in one day for two days, it’s just not possible. And people get so tired of it. I’ve had people try it, I’ve never ever seen anyone stay on that, ever.
Melissa Joy (36:04):
Yeah. Well, that’s interesting. I mean, yeah, Dr. Varady kept saying, because I was like, “Well, but the results are so much more significant, I want people to know that.” And she’s like, “Yeah, but nobody sticks with it.” I’m like, “Okay (laughs).”
Dr. Jim Painter (36:16):
That is very true.
Melissa Joy (36:18):
Yeah. Changing gears a little bit, we’ve been discussing how lower carb diets impact diabetes management, but yeah, I hear this question a lot, so I’d like to ask you, does excessive carbohydrate intake or sugar intake cause diabetes?
Dr. Jim Painter (36:34):
Well, absolutely not in the fact that it doesn’t really cause it but it shows you if you have it (laughs). And so, if you are having trouble metabolizing carbohydrates and your blood sugar is going up, then in that instance the sugar you eat is causing the diabetes because if you didn’t eat the sugar, it would stop.
And so, when someone says is it remission or is it cure and you get remission or a cure, I think you can get a cure if you just don’t eat sugar. So, in the big picture it doesn’t cause diabetes, but if you have diabetes, it’ll show you that you have it.
Melissa Joy (37:09):
I always tell people there are some people who can be overweight and eat a lot of sugar and they’re never going to get diabetes. They’re just not genetically predisposed to it. But if you are, then that’s a surefire way to trigger it and make it show up. Is type 2 diabetes, genetic? You mentioned remission or cure, is it reversible?
Dr. Jim Painter (37:29):
I found out it was reversible when I was 15. My dad lost his pilot’s license because his blood sugar went up and he was 40 pounds overweight. He lost 30 pounds in a short period of time. And he went back and he got his license back. Really? You can reverse type 2 diabetes. Yes. He got his pilot’s license back.
So, even while I was studying the literature going, “Is it possible, it’s not possible? Is it possible?” I knew it was possible the whole time. And then I read this study by Goldenberg it was published in 2020. It’s called the Efficacy and safety of low and very low carbohydrate diets for type 2 diabetes remission. So, it’s actually looking at remission, stopping the type 2 diabetes.
And so, what Goldenberg found was fascinating in the fact that over a period of time – all of these studies in this meta-analysis were 12 weeks or less and they were randomized at 130 grams or less of carbohydrate. That’s what we were talking about earlier 26% of the calories. And then they did a very low carb diet at 10 and both functioned well.
Melissa Joy (38:37):
10 grams a day?
Dr. Jim Painter (38:38):
No, 10%.
Melissa Joy (38:39):
10%, okay (laughs).
Dr. Jim Painter (38:40):
Thank you again. 10 grams, that’s really low.
Melissa Joy (38:43):
Like why even bother? Why even bother? That’s a cup of broccoli.
Dr. Jim Painter (38:47):
(Laughs) that’s right. And so, he looked at the remission rates and he found that those people that had low risk, the studies that had low risk of bias, they found out that they all reduced the blood sugar and the P value was 0.001.
Then they looked at the studies that had high risk or some risk of bias in their studies, they still had a P value of 0.009, they almost all lost weight too and their blood sugar normalized. So, can you go into remission? I think you can. I mean I’ve seen it personally in my family and then I’ve seen it with so many people that really take the weight off and they keep it off.
Melissa Joy (39:30):
And I mean it is a progressive disease. So, if you’re younger and you get it and you’re doing a great job with your diet and lifestyle, it could progress at some point as we age. That’s another one of the risk factors.
And I always tell my patients, “Yeah, you want to do the best you can with your diet and lifestyle, but at a certain point if you do need some help from medication, it doesn’t mean that you failed. It is a progressive disease.” So, is there a best diet for diabetes? I mean we already talked about it needs to be individualized, but in your opinion and looking at the literature.
Dr. Jim Painter (40:06):
I think generally, like I said, for the people that need it, the average American, 73% of us are overweight or obese, what is the best diet for those people? It’s a low carbohydrate diet. Is low carbohydrate best for everybody? Well, I’m not talking about everybody, I’m talking about diabetes, pre-diabetes.
For them it’s almost certainly the best diet, a low carbohydrate diet. Are there some people that can’t for some reasons? Yes, you’re pregnant, you’re nursing, you’re very young or very old. Is there a reason it might not work? Yeah, because sometimes people just need to eat food.
Well, I won’t eat anything but sugar. Fine, just eat it then because you don’t have any weight on you. But generally, for everybody that is middle aged, older and it is high blood sugar, pre-diabetes, type 2 diabetes, the low carbohydrate is the best.
Melissa Joy (40:54):
And the Mediterranean diet, it’s ranked number one diet all the time and we touched on it briefly before, but you’re saying the Mediterranean diet can be considered a lower carb diet.
Dr. Jim Painter (41:06):
You know, and think about it, they eat a lot of pasta. Yeah, they do but they eat a lot of whole foods (laughs), they eat a lot of meats and they eat a lot of vegetables, they eat fruits and so, the Mediterranean diet I think is a wonderful diet. It is a high fat diet, it is a lower carbohydrate diet and it’s pretty moderate in protein levels and there’s a study called PREDIMED.
And I got to know one of the authors about 10 years ago, it was done from 2003 to 2013 and they compared three groups. They had some people eating their normal amount of food, normal breakdown of their food and then they had two groups that were on the Mediterranean diet.
And so, they gave one group was a Mediterranean diet with extra olive oil. Really? And they had a second group was Mediterranean diet with extra nuts (laughs). Really? So, they had two by fat then they had a third group that was, we want you to just cut back on fat, need to eat less fat.
And so, they did, but they cut the fat, fat was in their diet was at about 37%, 39%, they were 39%. And the two heavy fat diets went from 39 up to 41%, which is about where we were in the 50s when they said, “You eat too much fat.” But that’s exactly what those people were eating.
And then they took a low-fat group and they went from that 39 to 37 (laughs) that’s it. It’s 2% difference, 39 to 37 and 39 to 41 or 41. After four and a half years they noticed, wait a minute, there’s one group that’s dying way too fast. Whose group is that?
They looked at the data and they found out that those people on the low fat, 37% fat, were dying at a significantly higher rate than those on the high fat, two levels of a Mediterranean diet. So, is a Mediterranean diet good? Yeah, it has been. It’s been a good diet for the last 5,000 years.
Melissa Joy (43:03):
Very good. So, would you suggest that people first kind of get a feel for how much carbohydrate and protein and fat I guess that they’re eating and then make some adjustments from there and kind of see what kind of results they get and how well they feel like they can stick with it?
Dr. Jim Painter (43:21):
Yeah, it is probably a good idea to see how much you’re doing without people going too nuts and weighing their food and counting the carbs. And it’s difficult to do, but to just assess your diet and look at it and see how are you eating a lot of carbs?
You have a cereal for breakfast, and you have a sandwich and bread for lunch and you having rolls and pizza for dinner, then that’s a lot of carbohydrate (laughs) and to try cutting back on it, to have a low carb diet that’s cutting a third of amount is amazingly beneficial.
Melissa Joy
Very good, as we’re wrapping up, I would love for you to share some sort of bottom-line takeaways for our listeners keeping in mind that some of our listeners are dietitians and healthcare professionals, but we also have the general public listening as well.
Dr. Jim Painter (47:52):
I think that the main thing is eat whole foods and someone says, “Wait, should I be vegan or should I be paleo or carnivore?” You didn’t hear what I said, eat whole foods. “But which ones should I do?” It really depends on your metabolism, what diet is best for you.
And they said, “You’ve been studying this for 50 years.” “Yes, 50 years.” “And the only thing you can say is eat whole foods.” Yes. Eat whole foods. That’s the first thing I say. And no matter what diet you go on, but then the next thing I say is really low carb diets for Americans living in the age we’re in today is better to cut back on the carbs.
Melissa Joy (49:19):
Okay. Very good. Where can people find out more about this topic and connect with you?
Dr. Jim Painter (49:25):
They can connect with me on my website. I’m on LinkedIn. And I’ve got a YouTube channel too.
Melissa Joy (49:49):
Oh, okay, great. I didn’t know about the YouTube channel, I have to check that out. And of course, I’ll have links to your LinkedIn, your website, any of the research articles that we talked about, I will try to link to at least the abstracts. If they’re open access, I will link to those as well. I’ll put as much as I can into the show notes at soundbitesrd.com.
There’s also, I’ll link to the 2025 Diabetes Standards of Care information and then the simplygoodfoodscompany.com “about” section so people can learn about that. And you also wanted me to include a visual in the show notes. Do you want to talk about that visual briefly?
Dr. Jim Painter (50:33):
Well, I talked about that a little bit already, and it’s just talking about how long do you need to go before you stop eating, that you get this benefit of increasing the right things in your diet? And so, when you talk about how long do you have to eat, it’s a nice little diagram. It’s from the Mattson study.
Melissa Joy (50:48):
The intermittent fasting, sort of.
Dr. Jim Painter (50:50):
Intermittent fasting and how long do you have to not eat? And it’s really 12, 14 hours, it starts the benefit, it goes great for as long as you can keep your mouth shut (laughs).
Melissa Joy (51:00):
Okay. Yeah, we’ll include that visual as well. That would be helpful for our listeners if they want to come to the show notes at soundbitesrd.com. Well, thank you so much Dr. Painter for coming on the show and sharing all this information with us.
Dr. Jim Painter (51:12):
Thank you, Melissa. It has been a privilege.
Melissa Joy (51:14):
And for everybody listening, if you liked this episode, please share it with a friend, tell a friend or colleague about the podcast and as always, enjoy your food with health in mind, until next time.
[Music Playing]
Voiceover (51:29):
For more information, visit soundbitesrd.com. This podcast does not provide medical advice, it is for informational purposes only. Please see a registered dietitian for individualized advice. Music by Dave Birk, produced by JAG in Detroit Podcasts, copyright sound bites, Inc. All rights reserved.
LISTEN, LEARN AND EARN
Listen to select Sound Bites Podcasts and earn free CEU credits approved by the Commission on Dietetic Registration (CDR) for registered dietitian nutritionists and dietetic technicians, registered. Get started!
Get Melissa’s Sound Science Toolkit here!
Partnerships:
Sound Bites is partnering with the Association of Diabetes Care and Education Specialists (formerly the American Association of Diabetes Educators)! Stay tuned for updates on the podcast, blog and newsletter!
Sound Bites is partnering with the International Food Information Council! Stay tuned for updates on the podcast, blog and newsletter!
Mary Linneman RDN LD CDCESon April 29, 2026 at 10:46 am
Awesome User friendly for a CDCES and teaching nutrition for Diabetes Been an RDN for >35 yrs glad we have come to a more common sense type of educating our clients
Sign up for my monthly newsletter and episode eblasts so you never miss an update!
Listen on Stitcher (Android)
Install the Stitcher App
1. Search for “sound bites with melissa joy dobbins” 2. Choose Play Current Episode or Add to Playlist
Choose “Play Episode”
Subscribe & Review on iPhone
Open the “Podcast” app on your iPhone
Search for “Sound bites with melissa joy dobbins”
Open the podcast and click “Subscribe” and your done!
Write a Review
Click “Reviews”, then “Write a Review”.
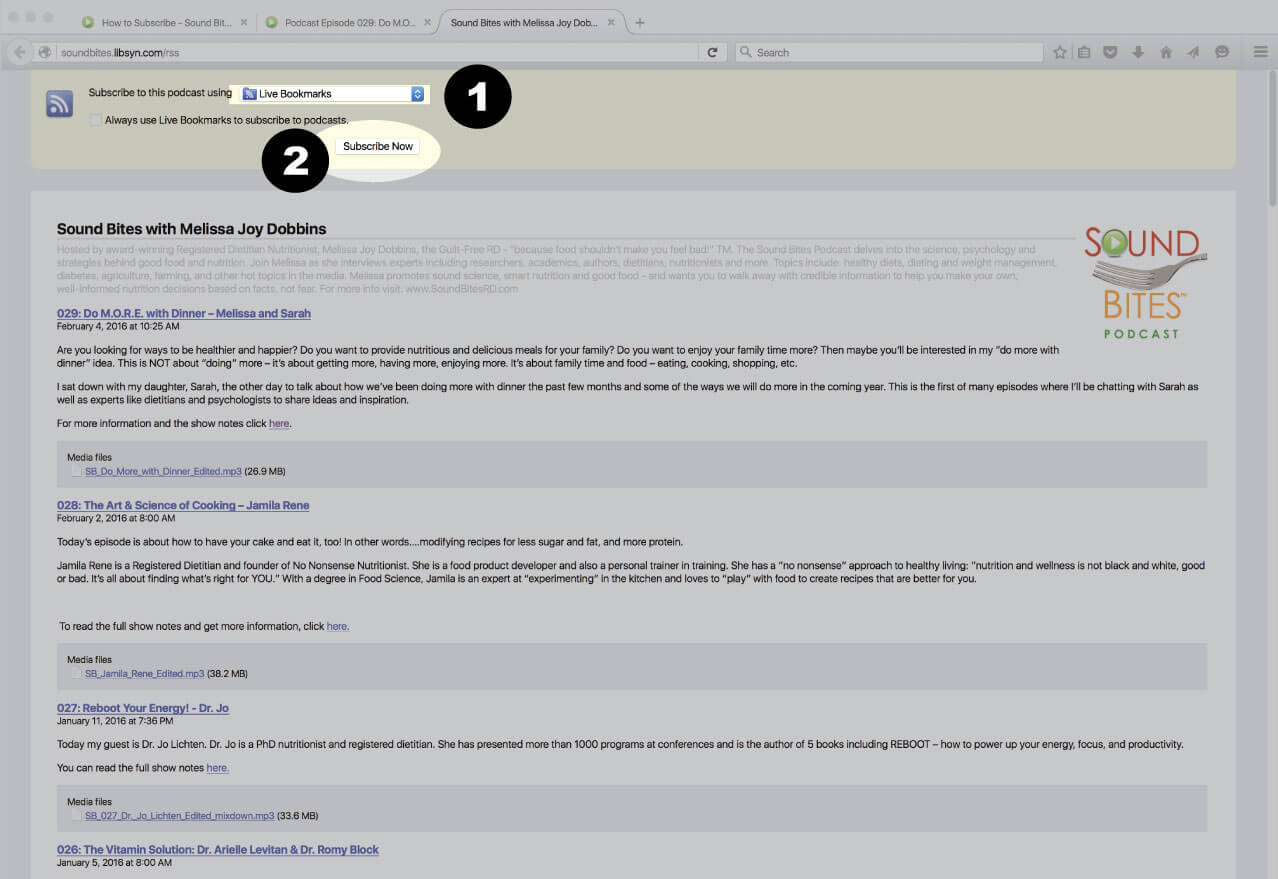
Subscribe via RSS Feed
Navigate to any podcast player . Click on the RSS feed icon.
Click on the RSS feed icon.
Click on RSS Feed
Choose which application you would like to use to receive the RSS feed
Click “Subscribe Now”
Confirm settings and subscribe.
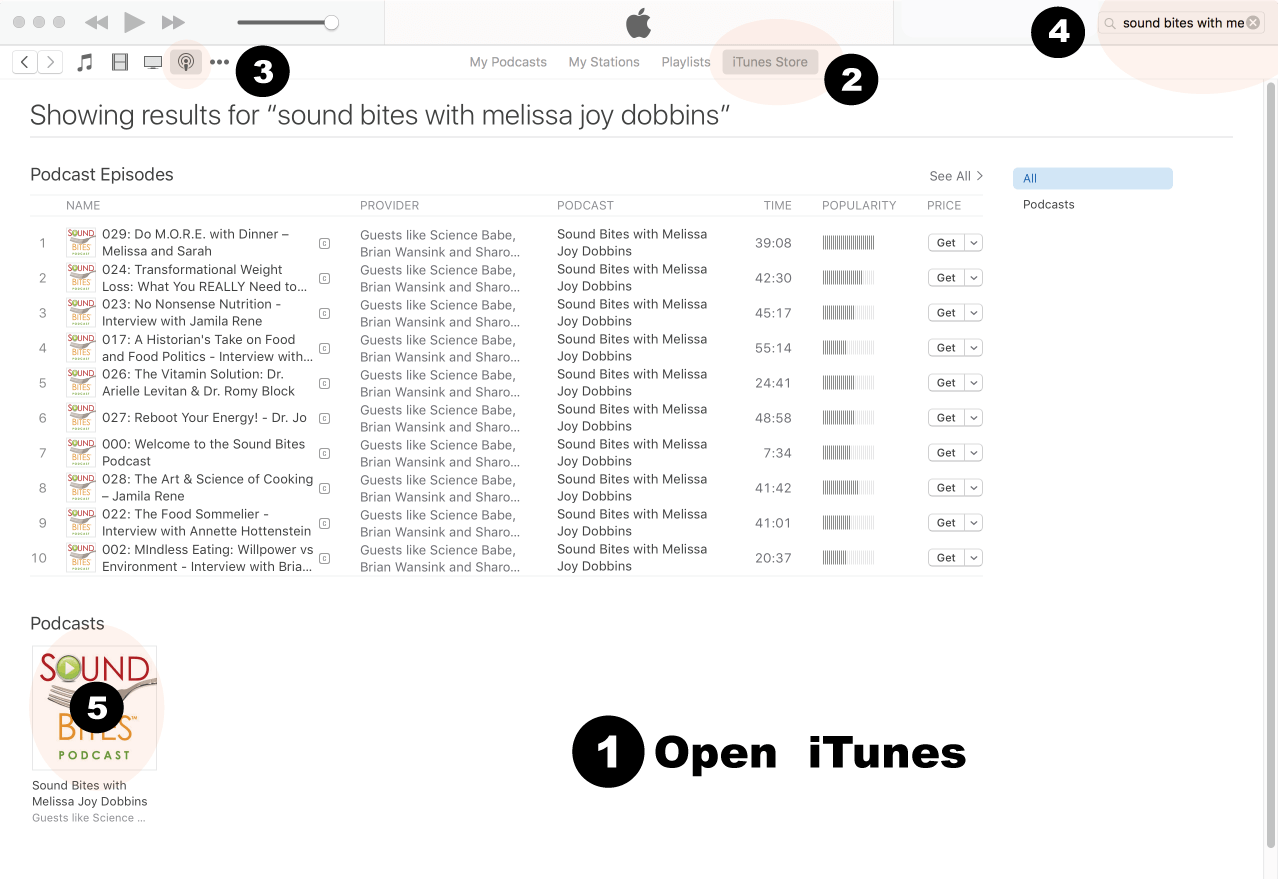
How to Review in iTunes
Open iTunes desktop application
Click iTunes Store
Click on Podcasts
Search for “Sound bites with Melissa Joy Dobbins”
Click on podcast image
Search for Sound Bites podcast in iTunes
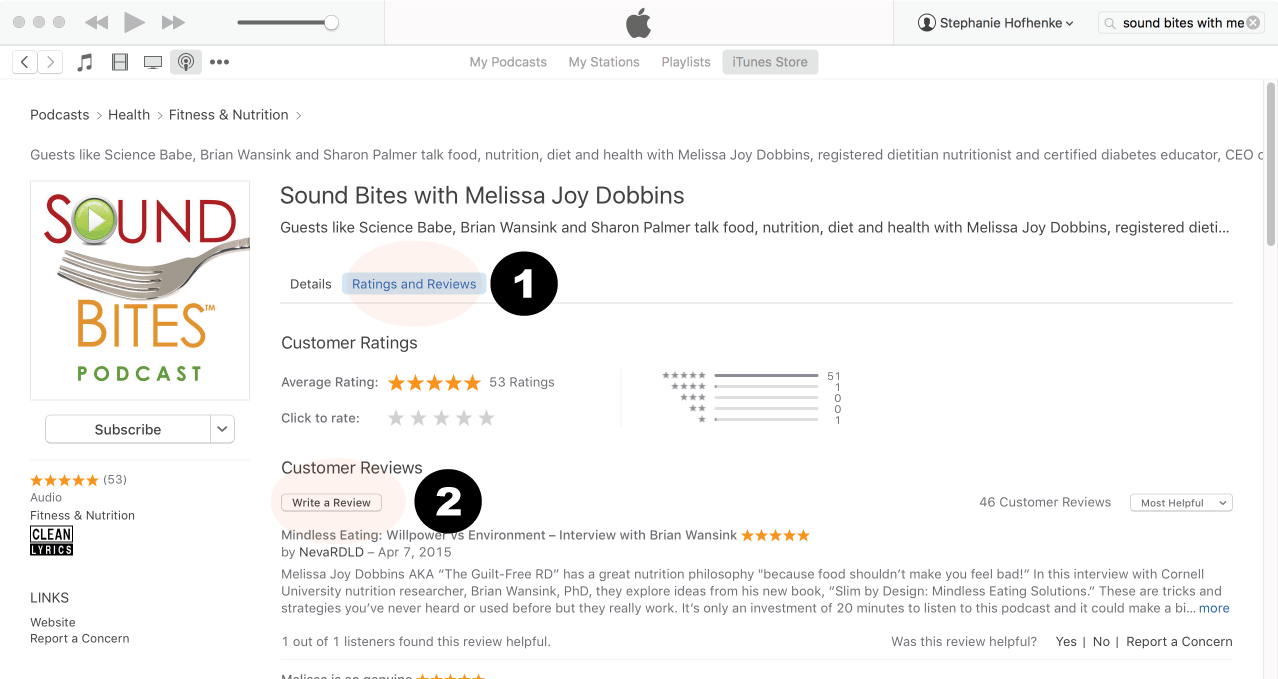
Click Ratings & Reivews
Click Write a Review
View reviews and write your own review.
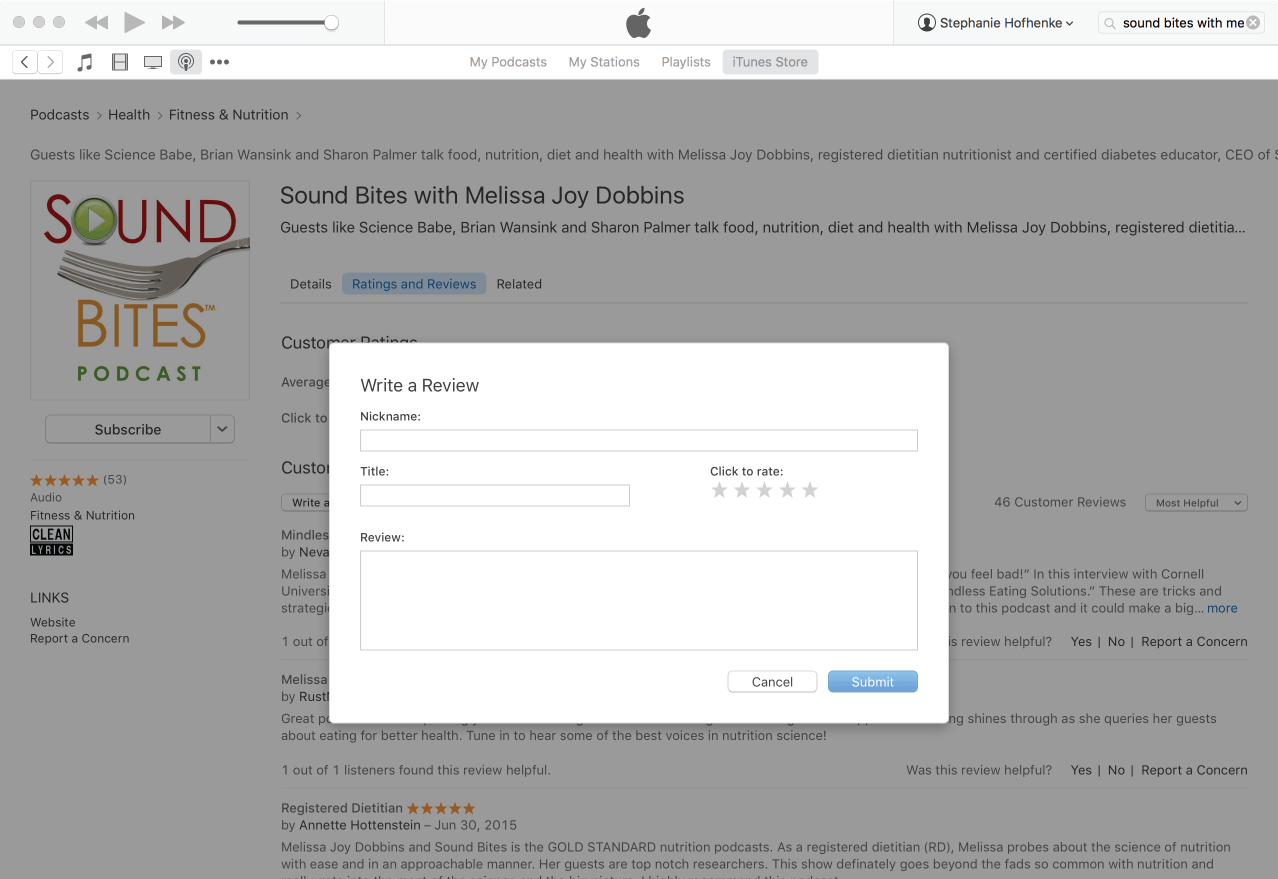
Write your review…. Thank you!
Write your review!
How to subscribe via iTunes
Click here to view the Sound Bites Podcastin iTunes, then click the blue “View in iTunes” button. This will open your iTunes application directly to Sound Bites Podcast. Click the “Subscribe” button, and your done!
 Dr. Jim Painter is an Adjunct Professor at University of Texas School of Public Health, Professor Emeritus from Eastern Illinois University, and MS in Integrative and Functional Medicine program director at John Patrick University’s Lifestyle Medicine program. His research specialties include heart disease and mindless eating. Jim has been an advisor for Sun-Maid Raisin Growers and Paramount Farms, and consults for the National Dairy Council. He worked for Marriott Corporation in the 1980s, taught at University of Illinois during the 1990s and at Eastern Illinois University until 2013. Jim has over 100 peer reviewed publications to his credit.
Dr. Jim Painter is an Adjunct Professor at University of Texas School of Public Health, Professor Emeritus from Eastern Illinois University, and MS in Integrative and Functional Medicine program director at John Patrick University’s Lifestyle Medicine program. His research specialties include heart disease and mindless eating. Jim has been an advisor for Sun-Maid Raisin Growers and Paramount Farms, and consults for the National Dairy Council. He worked for Marriott Corporation in the 1980s, taught at University of Illinois during the 1990s and at Eastern Illinois University until 2013. Jim has over 100 peer reviewed publications to his credit.











Great Podcast on Low” Carbohydrate Diets and Metabolic Health: What Does the Research Show. Thoroughly enjoyed it.
Thank you, Doreen!
Awesome User friendly for a CDCES and teaching nutrition for Diabetes Been an RDN for >35 yrs glad we have come to a more common sense type of educating our clients
Thank you, Mary!