Celebrating over 1 Million Downloads and 50,000 Free CEUs on the Sound Bites® Podcast | NEW: Get 1 years’ worth of CEUs with the new 15-CEU Podcast Course
Obesity Medications, Nutrition Therapy & the Unique Role of Dietitians in Obesity Care
According to the Centers for Disease Control and Prevention, more than 40% of American adults have obesity, costing the U.S. healthcare system an estimated $173 billion annually. The development of incretin-based therapies, such as glucagon-like peptide-1 (GLP-1) and glucose-dependent insulinotropic polypeptide (GIP), marks a major advance in obesity treatment. Registered Dietitian Nutritionists (RDNs) play a crucial role in providing medical nutrition therapy (MNT) to people using these medications as part of comprehensive obesity care.
Research shows that effective obesity care should include counseling from an RDN to support the adoption of lifestyle changes that optimize weight loss maintenance, prevent and/or reduce medication side effects, and achieve long-term health. RDNs offer essential services, including screening and assessment, medication support, and guidance on a nutrient-dense eating plan. They encourage healthy lifestyles, support positive body image, and promote physical activity to help maintain lean body mass during weight loss.
The newly published paper Incretin-Based Therapies and Lifestyle Interventions: The Evolving Role of Registered Dietitian Nutritionists in Obesity, highlights the RDN’s role in comprehensive obesity care. It provides expert guidance and advocates for expanded access to RDN-provided MNT in addition to obesity medications, opportunities for RDNs to advise on medication management, and a leadership role for RDNs on interdisciplinary care teams.
Tune into this episode to learn about:
the new paper published in JAND about injectable weight loss medications and lifestyle interventions
the unique and evolving role of RDNs in obesity care
why this new class of obesity medications has become so popular
how these medications work
the amount of weight loss needed to reduce obesity related comorbidities
the evolution of different terms for these medications
the pipeline of obesity medications we will see in the next few years
how these medications have impacted the role of RDNs in counseling patients
common side effects and nutritional considerations
concerns about loss of muscle mass and bone density
the importance of and role of exercise while taking these medications
emotional aspects of significant weight loss in a short time
how RDNs can be utilized in comprehensive obesity care in the long term
how RDNs can stay informed and up to date on the medications and obesity care in general
when people taking these medications should be referred to RDNs
how working with an RDN can improve a person’s experience and outcomes
additional information and resources for the public and health professionals
Linda Gigliotti, MS, RDN, CDCES, FAND
Linda has extensive experience in the clinical practice of adult weight management and multidisciplinary obesity treatment teams, having served as the Program Director of the Weight Management Program at the University of CA, Irvine for 20 years. She is co-editor of the Health Professionals Guide to Obesity and Weight Management, recently published by the Academy of Nutrition and Dietetics. Currently she serves on the Academy Foundation Board of Directors. Gigliotti is board certified in diabetes care and education and was engaged in the development of the interprofessional Certified Specialist in Obesity and Weight Management (CSOWM) credential. In 2021 she was awarded the Medallion Award by the Academy of Nutrition and Dietetics. She is also a recipient of the Excellence in Weight Management Practice Award by the Weight Management Dietetics Practice Group in 2017 and the CA Outstanding Dietitian of the Year Award in 2018.
Ideally every person prescribed an obesity medication should be referred to a RDN with expertise in obesity care at the point the prescription is written. These medications significantly impact appetite, food intake and the rate of weight loss. An RDN can optimize their use to manage side effects and potentially enhance outcomes.” – Hope Warshaw
Hope Warshaw, MMSc, RD, CDCES, BC-ADM
Hope has been a Registered Dietitian and Certified Diabetes Care and Education Specialist during her career that now spans 45+ years. Her work has ranged from counseling people with all types of diabetes and weight management concerns, to corporate consulting, freelance writing and book author. She is recognized nationally for her expertise and as a committed volunteer for several organizations including the Academy for Nutrition and Dietetics and the Association for Diabetes Care and Education Specialists. She has held national elected positions for both organizations. Currently she serves on the Academy’s Nominating Committee. Related to the content of this Sound Bites RD episode, over the last couple of years Hope has worked with the Academy’s Foundation, for which she served as chair in 2022-2023, to advance and enhance the role of the RDN in obesity care specifically with the incretin-based therapies/GLP-1 medications. In this role Warshaw worked closely with the Academy’s Foundation leadership to develop a successful webinar series held in early 2024. Another series co-led by Warshaw and Gigliotti on this topic is in development for early 2025. Additionally, Warshaw is a co-author on a publication: Incretin-Based Therapies and Lifestyle Interventions: The Evolving Role of Registered Dietitian Nutritionists in Obesity Care, recently published in the Journal of the Academy of Nutrition and Dietetics.
Obesity medications will be a component of obesity care and chronic disease management for years to come. This is an opportune time for RDNs to step up to enhance and advance their role in obesity care.” – Linda Gigliotti
Resources
Some links may be affiliate links. As an Amazon Associate, I earn from qualifying purchases.
Speakers: Melissa Joy Dobbins, Hope Warshaw, & Linda Gigliotti
[Music Playing]
Voiceover (00:01):
Welcome to Sound Bites, hosted by registered dietitian nutritionist, Melissa Joy Dobbins. Let’s delve into the science, the psychology, and the strategies behind good food and nutrition.
Melissa Joy (00:23):
Hey there, if you’re a dietitian and you’re trying to fulfill your continuing education requirements, be sure to check out my free CEU activities. I have nearly three years’ worth of free CEUs you can receive by listening to my podcast.
I also have a CEU package on sale for one year’s worth of continuing education credits, which offers the convenience of taking only one quiz and receiving one certificate for all 15 credits. Simply go to my website at soundbitesrd.com/freeceusfor all the details.
Hello, and welcome to the Sound Bites Podcast. Today’s episode is about obesity medications and the role that registered dietitian nutritionists can and should play in this evolving area of comprehensive obesity care. This episode is not sponsored.
My guests today are Hope Warshaw and Linda Gigliotti.
Hope Warshaw has been a registered dietitian and certified diabetes care and education specialist during her career that spans more than 45 years. Her work has ranged from counseling people with all types of diabetes and weight management concerns to corporate consulting, freelance writing, and authoring books.
Linda Gigliotti is a registered dietitian nutritionist and certified diabetes care and education specialist from Orange County, California. She has extensive experience in the clinical practice of adult weight management and multidisciplinary obesity treatment teams, having served as the Program Director of the Weight Management Program at the University of California Irvine.
Welcome to the show, Hope and Linda.
Linda Gigliotti (02:07):
Thanks, Melissa.
Hope Warshaw (02:09):
Happy to be back on your fabulous podcast.
Melissa Joy (02:12):
Yes, and this is Linda’s first time, but hope you have been on several times, so welcome back. I’d like to just start off with a little factoid, if you will.
According to the CDC, more than 40% of American adults have obesity, and the development of new medications such as these popular GLP-1s really marks a major advance in obesity care. And registered dietitian nutritionists (which I’m going to just refer to as RDNs from here on out), they can play a crucial role in providing medical nutrition therapy to people using these medications as part of comprehensive obesity care.
So, we are going to discuss a new paper recently published in the Journal of the Academy of Nutrition and Dietetics on the role of the RDN in obesity care, particularly when it comes to obesity medications. This paper is titled Incretin-Based Therapies and Lifestyle Interventions: the Evolving Role of Registered Dietitian Nutritionists in Obesity Care.
Now, Linda and Hope, you were first and second authors of this publication respectively, along with several other RDNs and also, two physicians. So, let’s start with you Hope, how did this paper come about and why was it important to have it published?
Hope Warshaw (03:32):
So, Melissa, as they say, one thing led to another. Linda and I have been working with the Academy and the Academy Foundation since about mid-2023. I believe I was past chair of the foundation at that point, Linda is now on the board of the Academy Foundation.
And I made a plea that the organization makes sure that they advance the knowledge of RDNs around these medications, and to make the case to healthcare providers at large, that nutrition therapy provided by RDN needs to be a critical component in the use of these medications in obesity care.
So, initially, Linda and I, with some funding to the Academy Foundation, organized a series of three webinars on the topic that I know you are familiar with and will hopefully link to in the show notes. These are still available at no cost. At the same time, Linda and I were also involved in an effort to help the academy draft a statement on this topic, the role of RDNs in obesity medications.
And this led to a report on the academy website, which was not good enough for us because we all, the authors of this publication, felt it was critical for us to publish a citable publication. And with this, to put our stake in the ground about the critical role of RDNs in MNT when using these newer medications.
Really, to date, there’s only been a few publications that have been focused on nutrition, much more on the pharmacotherapy. But as standards and guidelines are being developed, it is so important that RDNs have a seat at the table, and if you will, muscle our way in which I think we have to do, and just making sure that the role of nutrition and RDNs is integrated into standards and guidelines regarding the use of these medications in weight loss as well as in weight loss maintenance, I know we’ll get into.
Melissa Joy (06:04):
Absolutely. Okay, very important points. Thank you. So, Linda, how about we turn to you. Can you describe this new class of medications to manage obesity and why they’ve become so popular?
Linda Gigliotti (06:18):
Sure, Melissa. I’ll answer the second part first: why have they become so popular? And that’s because we are seeing such significant weight loss with the medications much more than has been evidence in the earlier classes of obesity medications.
This new drug category mimic gut hormones, specifically incretin hormones, and we refer to glucagon-like peptide-1 or GLP, but also GIP, which is glucose-dependent insulinotropic polypeptide called GIP for short, fortunately.
But these are incretin hormones produced, secreted in the GI tract in response to food. The drugs mimic those hormones. They’re actually synthetic forms, and that’s why we call the drugs receptor agonist or RA forms. They’re synthetic forms of the gut-derived hormones that activate these receptors in various tissues in the organs of the human body.
Now, the relevance for weight management is huge, specifically in the gastrointestinal tract. They delay gastric emptying and glucose absorption, so that promotes greater satiety between meals. We also find that there’s an impact on the pancreas promoting the release of insulin, which in turn helps to regulate blood glucose and appetite. And they also impact parts of the central nervous system, decrease in cravings and what is referred to as food noise.
So, because there’s that decrease in appetite and decrease in cravings, it’s a perfect fit for an obesity management drug. What’s interesting is that we’re finding that these medications also exert a variety of other actions on other systems of the body: the immune system, the cardiovascular system, the cerebral system, muscular adipose tissue.
So, we’re finding that the medications are effective not only for reducing weight, adipose tissue, but also other chronic diseases, which I know we’ll touch on.
I do have to point out that while we say, “Oh, this new class of medications,” these really are not new medications. The first incretin-based therapy was approved in 2005 for treatment of diabetes, and there have been several others approved over the course of the last 20 some years.
Since 2005, there are five incretin-based medications that are FDA approved for diabetes. Three of those have been approved for the treatment of obesity, specifically Liraglutide, Semaglutide, and Tirzepatide for the treatment of obesity.
Melissa Joy (09:16):
So, Linda, as a follow up to that, I’m often curious because we hear that these are new medications, but as you just said, and as I know, being a certified diabetes care and education specialist myself, we’ve been using these for a couple of decades in diabetes.
So, what’s the difference? Is it just because now they’re approved for use in obesity, not just diabetes? Or is there something about the newer medications? What’s the difference?
Linda Gigliotti (09:45):
I think the most outstanding point that has drawn so much attention to this class of medications is really twofold. The earlier medications, including the earlier incretin-based therapies, the weight loss was in the range of 5 to 10% of body weight, which is medically significant. You don’t want to knock that at all.
However, with the newer meds with Semaglutide, the STEP 1 trial found a mean weight loss of about 15% of body weight. And the SURMOUNT trial, which was the major trial with Tirzepatide, weight loss was up to 21% of mean body weight.
So, that’s huge, it’s significant. And these were weekly injections instead of daily injections as the earlier medications required. So, that amount of weight loss with I say a little bit less invasive care involved with that drew a lot of attention to these medications.
Melissa Joy (10:50):
Okay, thank you. So, speaking of the percent weight loss, I know you shared a slide with me, so I’d like you to address this. What can you tell us about the percent of weight loss that we see with these medications related to minimum benefit, maximum benefit, therapeutic benefit.
Linda Gigliotti (11:10):
Sure. As I always emphasize with my patients, every pound that comes off is worth protecting and keeping off because it makes a difference in your health. Even with 3 to 5% weight loss, we see some improvements, let’s say with blood glucose level and triglycerides, but the more weight that is lost, the more improvement we see in obesity-associated comorbidities.
So, for example, if we can see up to 15% weight loss, we can see remission of type 2 diabetes. So, other medications, traditional weight loss methods, certainly can lead to some health improvements. But to get up to 15/20% weight loss, you can really see major changes in reduction of health risk and improvement with comorbidities.
Melissa Joy (11:58):
Can you just list some of those comorbidities so people who are listening might-
Linda Gigliotti (12:02):
Well, type 2 diabetes is probably the number one thing that jumps out, but GERD (gastroesophageal reflux), sleep apnea, liver improvement, infertility, PCOS (polycystic ovary syndrome), even arthritis, knee pain, and osteoarthritis, cholesterol, blood pressure, cardiovascular improvement, et cetera.
Melissa Joy (12:27):
Thank you. Hope, initially, these obesity medications have been referred to as anti-obesity medications, and in this paper, you’re using the term incretin-based therapies. It seems like there’s some evolution to possibly the term obesity medications. Can you tell me your thoughts on this whole terminology soup? (Chuckles).
Hope Warshaw (12:49):
Sure, and I think we were right in the middle of it when we were writing this publication. But I am pleased to see the term evolve from that anti-obesity medications term that definitely caught on in the early literature.
And as I traced back, it was not something that FDA did. They didn’t name these anti-obesity medications. I think it was more-industry related, but that term carries with it some underlying bias, and it’s just stigmatizing sounding. I mean, we certainly use the word anti-hypertensive meds, but in this case, it just seems more stigmatizing.
So, there definitely has been pushbacks and requests not to use the anti-obesity term. And I think for that, we use the term incretin-based therapies because really, saying GLP-1 medications is not accurate, and is going to become less accurate. So, we used incretin-based therapies.
But as we’ll discuss, there will be more of these medications, and I think Linda and I, through some conversations that we’ve had are beginning to see some nice evolution to just calling these obesity medications.
Melissa Joy (14:19):
Well, yeah, what can you tell us about this pipeline of medications that we’re likely to see coming down the pike?
Hope Warshaw (14:27):
Sure. So, suffice to say these obesity medications are not a passing fad by any stretch. Pharma companies and the public have already witnessed the popularity and success for some people of using these medications.
With the two main medications we have today, which we’ve just been talking about, we have Semaglutide or Semaglutide (it depends how you want to say it), which is the GLP-1 receptor agonists such as Ozempic and Wegovy. There’s some different dosages within that.
And then there is Semaglutide plus the gut hormone that Linda had the burden of abbreviating GIP, and that dual agonists are Zepbound and Mounjaro. So, Zepbound and Mounjaro or drugs from Eli Lilly, Ozempic and Wegovy are Novo Nordisk drugs.
So, these companies have numerous ongoing studies really on these drugs, not even new drugs, to demonstrate their benefit in improving other obesity-related health issues beyond weight loss and glycemic control. And Linda just mentioned those from that slide. That actually is included in our paper. So, renal disease, sleep apnea, liver disease, and it’s just because of the way that FDA requires the companies to seek additional indications for the use of these medications.
In addition to these and to moving towards medications that we do not currently have on the market, and pardon me if I am mispronouncing any of these generic names. But some of them are tongue twisters. Hopefully, they’ll be easier eventually when we get trade names like Zepbound.
So, in addition, Lilly is far along on we’re Retaturtide, and always that “T-I-D-E” ending because that’s the similarity. This is a triple agonist. So, where Tirzepatide is a dual agonist, this is a triple agonist with GLP-1 receptor agonist, GIP and glucagon. And many of us, particularly in diabetes, are quite familiar with glucagon.
Then from Novo, there’s CagriSema — this is a blend of Semaglutide and long-acting Amylin. And again, in the diabetes world, we are familiar with Amylin, which was a drug on the market, still probably is, but not heavily used.
Another potential drug from a couple other entities, also a tide is Survodutide that combines GLP-1 agonist and glucagon. Another is Dapiglutide, which is a blend of GLP-1 and GLP-2 agonist. And then there’s a newer whole category beyond the tides, if you will, to a group of meds with the suffix, G-L-I-P-R-O-N. So, maybe we can remember them with “ipron” or just “glipron.”
The generics are like Danuglipron and Orforglipron. And I think what’s exciting about those, they’re smaller molecule, and the development is looking at can these be in an oral form of medication.
So, some of the newer medications are demonstrating even greater weight loss results than that 15 to 20%, but we’ll continue to see these studies. These are big, big, very expensive multicenter pharma trials, and the news will continue to come out.
And I did share an article with you that you’ll put in the show notes from Nature in 2024, and it was a very good article about the pipeline of medications.
Melissa Joy (19:20):
Great.
Hope Warshaw (19:21):
Sorry for being long-winded (chuckles).
Melissa Joy (19:23):
No, that’s very interesting. And you answered my next question, was are all of these injectables right now, is there anything oral? Like we’re looking at definitely-
Hope Warshaw (19:34):
I would say yeah. I mean, there is obviously a desire to do oral if you can, and I believe there’s discussion towards monthly. Right now, we’re at weekly. So, I mean you’re just going to see this whole area of obesity medications just continue to evolve.
I feel like it’s safe to say that we are in the early days of these medications. I think we’ll look back in 5, 10 years and agree that we were in the early days. I don’t know if Linda agrees or not, but-
Linda Gigliotti (20:16):
Absolutely.
Melissa Joy (20:17):
Interesting. So, how has the availability and use of these medications impacted how RDNs should be counseling people with obesity? Linda, perhaps you can weigh in on that.
Linda Gigliotti (20:29):
Yeah, Melissa, I think we need to step back and maybe look at the bigger picture of how we viewed obesity in order to best answer that question, and I’m thinking back to the early days of my career, really, we didn’t even use the word obesity.
We had patients, clients who came to us, and they were concerned with excess body weight. Often, it was for cosmetic reasons. There really wasn’t the appreciation that weight had much to do with health or that we could do much about weight at weight and health.
So, when our patients came to us, as dietitians, we worked with them on a calorie deficit plan to lose the weight, to promote that weight loss. And there were a variety of ways to do it and still use some of them today. There’s nothing wrong with that.
However, the amount of weight that could come off typically with a reduced calorie plan, 5% maybe — not really enough to make a health impact, and not enough for everybody to make the health impact that they wanted to.
And I think in this evolution, the whole medical profession, healthcare community began to view excess adipose tissue as a medical problem. Not really lack of willpower, but began to appreciate that there were so many contributing factors to the disease of obesity, and actually, labeled it a disease, a chronic disease.
So, as we begin to more and more accept that obesity is a chronic disease, then our role shifts to not just helping people lose weight on the scale, but look at all of those other numbers that are important, whether it’s their glucose level, how many blood pressure medications they’re taking, their quality of life with reduced knee pain, et cetera, et cetera. It really evolved into a more holistic view of obesity care, not focusing on getting to a particular number on the scale, but a much bigger picture of quality of life.
Now, with these medications, I think our role shifted even more because to lose adipose tissue, we have to upset that calorie balance of calories in, calories out one way or another. And what these medications do very often is to suppress appetite enough that people are consuming a calorie deficit plan because of the impact of the medications.
So, our role then shifts not so much to work with people, counsel our clients to reduce calories, but more to look at, well, what are they eating? If they’re eating less, what’s the quality of what they’re taking in? Are they getting a nutritionally adequate plant? Are there specific needs, protein, calcium, et cetera that need to be focused on? Are they remembering to eat if their appetite is suppressed so much?
So, ironically, sometimes I think now with these newer incretin medications, we actually are working with some of our clients to consume enough for safety reasons because their appetite occasionally is suppressed significantly.
Melissa Joy (23:43):
Yeah, absolutely. Hope, do you have anything to add perhaps from a diabetes perspective?
Hope Warshaw (23:49):
No, I don’t feel like our counseling strategies were that different until I would say we got to that early 2000s when we began to have some of the earlier drugs in this (the newer, as we’ve been calling them) obesity medications.
And I mean I do remember, I think this is still talked about today, but you would be going to conferences, and we would be seeing colleagues that were losing significant amounts of weight, and I think there was a lot of buzz about the use of these medications.
Melissa Joy (24:44):
So, what can you tell us about the side effects? Linda, you mentioned sometimes people are forgetting to eat or not eating quite enough, and I’ve heard about some of these side effects, and have concerns myself about adequate nutrition for people who are on these medications.
Talk to me about the side effects. Hope, maybe we can start with you. Can people stay on them? Do we need to adjust the dosage sometimes? What are we looking at?
Hope Warshaw (25:10):
Sure. So, let me take the first questions first. Some, but definitely not all people who go on one of these medications experience short-term side effects. The most common side effects we see, and I think people hear about are the nausea and vomiting.
For some people, these side effects are transient, and they may disappear, and then reoccur when the dose is increased or titrated up. We haven’t yet mentioned that people are started on a low dose, and then that dosing is increased as long as they do not have side effects, and it’s tolerated. There are definitely some people who have significant nausea and vomiting, and just cannot take these medications, and that’s just the reality.
So, the other common side effect and is less talked about, I think, is constipation and sometimes diarrhea. So, these GI tract issues can occur really related to how the medications work. They slow down the movement of food through the GI tract. And in our publication, there’s a figure that offers nutrition management strategies for these side effects.
I have to say as an RDN, I believe it would be optimal if people were referred to an RDN prior to starting one of these medications. So, we could even begin by talking about how these medications work (laughs).
Melissa Joy (27:00):
Great.
Hope Warshaw (27:02):
And also, so we could provide people with tips to implement before they start taking the medication, such as stop eating the second that you begin to feel full. That’s really a simple message and very important. And then there are longer term side effects that I think we’ll talk about.
To your second question, which is how often do these side effects cause users to discontinue use — adverse GI effects in clinical trials led to the discontinuation of medications in 5 to 10% of subjects. However, it is thought that the rate is higher once drugs are used in the real world.
Melissa Joy (27:56):
So, then what are some of the nutritional considerations that people who take these medications and the RDNs who counsel people, what are some of these nutritional considerations we’re dealing with?
Hope Warshaw (28:08):
Linda mentioned a couple, but I’ll build on that. Again, due to the action of these medications of decreasing gastric motility, decreasing appetite, the big concern … so, we’ve done this transition from counseling people on calorie deficit intake for weight management. Now, we’re concerned about adequate intake of calories and not only just calories, but quality of nutrients.
Another concern, perhaps even more so, is adequate hydration. Now, if people are eating less total food, you’re getting less fluid. And if people are forgetting to eat, they’re potentially also forgetting to drink.
And you may be working with people with obesity who go from constantly thinking about food and that sort of this food noise issue. And due to the loss of appetite and their delight with significant and sometimes rapid weight loss, they do not eat.
So, sufficient protein intake and the distribution of protein through the day is critical to maximize protein synthesis and minimize loss of lean body mass. Sufficient fiber consumption is important to decrease constipation, and as we RDNs know, only a small percentage of people who consume a decent amount of calories even get adequate fiber. So, making sure those fruits and vegetables and grains that give us fiber are consumed.
Inadequate food and nutrient intake can lead to potential micronutrient deficiencies, people may need at least a multi-vit and mineral supplement. And RDNs with the skills to perform nutrition focused physical examination may find these skills of value in assessing these patients for nutritional deficiencies.
But again, I think because we’re at such early days of using these medications and seeing this level of rapid weight loss and impact on appetite, we’ve only begun to see the role of nutrition.
Melissa Joy (30:43):
That’s a lot. Linda, do you have anything to add?
Linda Gigliotti (30:48):
Yes. It’s not just a matter of knowing what to eat, but I think sometimes even more important, helping our clients know how to eat, particularly if they’re not feeling hungry. So, it’s important to assess what a person’s food habits were like previously, how many times a day did they eat? Did they do their own food preparation? How many meals were consumed away from home, their cultural preferences and so forth.
And then work with the client on a meal schedule, a food plan, if you will, because when the appetite is suppressed, it’s helpful to take in smaller quantities multiple times through the day. In the case of protein, which has probably a heightened requirement during intense weight loss like this, the protein’s better utilized when it’s dosed multiple times through the day three or so meals per the day. So, working on that meal schedule.
And then thinking about food preparation; is the client used to grocery shopping and preparing food at home, taking food to work, et cetera? If they’re not going to be doing food preparation, how can they find in the marketplace foods that are nutrient dense and readily available? Is this the time to use some prepared meals or even meal replacements to help that client build the schedule for adequate food intake. And build that while we’re addressing those needs for protein, minerals, vitamins, et cetera, et cetera.
Melissa Joy (32:30):
Right, right.
Hope Warshaw (32:31):
I just wanted to sort of bring us back to earth for a second because I think we would all to see RDNs being utilized a lot with people taking these medications. I think we all realize there’s a lot of roles for RDNs in counseling people who are taking these medications. And I believe we believe that we could have a lot of impact on outcomes.
However, the reality piece is we know that lots of prescriptions for these medications are being written in primary care, in internal medicine as well as in obesity centers. But I think very few people are actually getting the benefit of counseling from RDNs. So, I just wanted to bring us a little bit back to earth.
Melissa Joy (33:33):
To be clear, yes, that does not surprise me at all. I’m always saying how I wish more doctors referred patients to dietitians, and this is certainly no exception.
So, with this decreased intake, what can you tell me about concerns with loss of muscle mass, loss of bone density?
Linda Gigliotti (33:54):
Well, we know with any weight loss that there is loss of some muscle mass. It’s estimated 15 to 20, 25% or so. The concern being raised is, is the loss of muscle mass with the use of incretin-based therapies greater, and that’s the subject that’s being studied.
Along with that, is potential concern for loss of bone density. So, how do we address that? Well, one, is to make sure nutrient intake is adequate. The recommendations for protein intake are upwards to 1.2 to 1.5 grams per kilogram as compared to the RDA of 0.8 grams per kilogram for protein intake.
And as I mentioned, spreading it out throughout the day, adequate calcium intake, usually a supplement going along with that. We can touch on physical activity. That role in maintaining both muscle and bone density.
But I will say this is an area that’s being studied. We don’t have all the answers here of how much we can protect with this significant weight loss.
Melissa Joy (34:59):
Right, yes. So, I was just thinking about that with physical activity. We know that that helps maintain lean body mass and is helpful for bone density.
Hope, what can you tell us about the importance of physical activity while taking these medications, and also, what the role of the RDN should be talking to clients about physical activity?
Hope Warshaw (35:21):
Sure. So, engaging in various, really, all forms of physical activity is very important and important in general public, it’s important for people with obesity.
With these obesity medications that have the ability to cause rapid and significant weight loss, providing advice and encouragement to engage in various forms of physical activity can help minimize lean body mass loss, maintain muscle mass, physical function, and to minimize bone loss. But I think a lot of that still has to be explored.
Less relevant is really the role of physical activity in weight loss. And we know that from studies with these medications, but that where physical activity really becomes more important is after weight loss and in maintaining pounds lost. And that is critically important and really imperative.
RDNs can counsel clients on moving more and the basics of physical activity. Obviously, different people have different risk levels in terms of doing physical activity, but a recent publication that was in the Journal of the Academy of Nutrition and Dietetics by Robinson talked about evidence-based guidelines for the general population that RDNs can provide. And I think you’ll list that in the show notes, Melissa.
Melissa Joy (37:14):
Yeah, happy to do that. Great.
So, Linda, let’s touch on the emotional aspect of losing such a significant amount of weight in a short time, which we’re seeing with these medications.
Linda Gigliotti (37:27):
My experience in medical weight loss programs where people have lost a significant amount of weight in a short time is that often, the client is not prepared for the new person that emerges as they lose weight.
And sometimes, the expectations are unrealistic about what this new body is going to bring for them. People are often surprised, taken back about how their people relate to them. Family, friends can treat them differently. I’ve had family members sabotage because it’s not the same person and they can’t tease them, relate to them, count on them for a good time the way they used to at a higher body weight.
People can have unrealistic expectation of, “Oh, now, I’m going to get a better job or be in a different kind of relationship” or be off put by the way people approach them now that they’re at a much more lower body weight. So, I think people sabotage themselves, just not being prepared.
And then looking very holistically and perhaps beyond the emotional part, but what other uses has food had in a person’s life? Sleep habits can be disrupted. Perhaps food was being used as a sedative before, and now that the person’s eating less, they don’t have that sedating effective foods. So, do they need to practice some sleep hygiene?
Stress management — has food been used as an outlet for stress? Well, now that food’s not calling their name, how do they manage stress?
So, all of these issues can come up, so I think it’s really important to address the mental health very broadly, look at lifestyle, again, very broadly, beyond food and physical activity, and look at the whole person, all other aspects of their lifestyle that may need to be addressed during this time of weight loss and beyond.
Melissa Joy (39:30):
All really, really good points. Let’s change gears a little bit.
Hope, let’s talk about how RDNs can be utilized in comprehensive obesity care in the long-term.
Hope Warshaw (39:42):
Great and very important question. So, it’s critical for RDNs as well as all healthcare providers to get our heads around the fact that managing obesity is a chronic disease. We’ve mentioned that a couple times.
Just like hypertension or diabetes, do you go off medication? No. If anything, we see escalating amounts and types of medications for hypertensive, lipid lowering or improving or diabetes. So, as RDNs, it’s really important for us to be involved with the person with obesity prior to even starting one of these medications.
I think I mentioned that we can discuss with a client how the medication works and the side effects that they may experience. And as I said, even upfront, we can offer a few tips about how to minimize the common GI side effects such as stop eating the moment you feel full.
In addition, we can talk to people upfront about their long-term weight loss expectations and plan for the long-term maintenance of lost weight, which we know is so very, very difficult. We need to engage people in realistic conversations about their weight loss expectations, how they think rapid weight loss may impact countless areas of their life. Linda touched on a number of those.
As well as discussing the long-term behavior changes and food habit changes, they will need to be successful at keeping those lost pounds off. With the availability of these medications and others in the pipeline, we’ll likely be talking to people how they may use a lower dose of one of these medications very long-term, or they may find through trial and error that taking one of these medications intermittently.
This is really a whole new discussion area. We’ve never had the opportunity to have these discussions before, and I think these obesity medications are really pushing us into a full new area in comprehensive obesity care.
Melissa Joy (42:24):
Thank you. Hope, you’ve mentioned several ways that working with an RDN can improve a person’s experience or outcomes when taking one of these medications. Was there anything else you wanted to add? And Linda, you could weigh in as well?
Hope Warshaw (42:36):
Well, again, we’ve mentioned a few times we’re at the early stages of long-term studies with these medications and realities. The studies tend to be these big pharma trials that they have to do to get these medications approved by FDA. So, we really have no studies to date to objectively measure the experience or outcomes of working closely with an RDN when someone’s taking one of these medications.
But I conjecture that or hypothesize, I suppose, that knowing how the medication works, knowing potential side effects and having strategies to deal with them, understanding the need for an implementation of a long-term weight management plan. And so, being counseled side by side consistently by an RDN would be beneficial and would produce better outcomes.
I think we’ve got these medications being prescribed, as we mentioned by primary care and internal medicine who do not tend to have as much access, unfortunately, to refer RDNs versus in comprehensive obesity care centers. And I think the comparison would be interesting though I can’t point to any literature at this point.
Melissa Joy (44:02):
Fair enough. Linda, any other thoughts on that?
Linda Gigliotti (44:05):
Yeah, I think we should take off our weight management hat here, and look at how we are working with a client for that overall health management so that we’re not just focusing on this is to help the client lose weight, reduce their obesity, but rather, what is the overall management of other chronic diseases, comorbidities, quality of life for the client.
And yes, addressing weight may be one of the interventions, but it’s not the only thing we focus on. We look at that whole person for that overall management of comorbidities and quality of life.
Hope Warshaw (44:55):
And maybe that becomes a sort of winning argument for coverage of these medications in terms of reducing healthcare costs long-term.
Melissa Joy (45:05):
So, we’ve talked a little bit about weight loss maintenance, and I suppose it varies, but can some people come off of these medications? Do most people probably need to stay on them or perhaps change the dose?
I have a related episode with Dr. Jim Hill on weight loss maintenance if people want to take a deeper dive. But if there’s anything either one of you wanted to share regarding that question.
Linda Gigliotti (45:29):
Melissa, I think the answer here is we don’t know. Obesity care is evolving. So, I can’t answer the question yes or no, but I can say we need to accept obesity as a chronic disease. And if we do that, then we can step back and say, “Well, does a person with diabetes or hypertension need to take a medication forever?”
Maybe not, maybe not — maybe not the same medication, but a different medication, maybe a different dose of the medication. Maybe there’s even another intervention for that chronic disease. But we do know that with obesity being a chronic disease, it will require long-term management. What it exactly looks like, I don’t know. That’s evolving.
Melissa Joy (46:12):
Very good. As we’re wrapping up, if there was any bottom-line takeaways you wanted to share or summaries — I mean, I think we’ve talked about quite a bit, but if there was any more points that you wanted to share regarding that, and then we will talk about where people can get more information.
Hope Warshaw (46:29):
So, I’ll take a start at that. I think for RDNs who are listening and those who are involved in obesity care or want to be, I want to encourage you to step up and insert yourself. And so, take on the important role that we should be playing in the use of these medications, either at your place of employment, in your institution, or in organizations that you’re involved with, perhaps those that are writing standards of care.
So, let’s have RDs at the table as these standards and guidelines are written. And I think for consumers who are interested in taking one of these medications or currently take them, consider asking for a referral to an RDN, and don’t think of this as a one-time visit. I think you’ll be benefited by a longer-term partnership with an RDN, particularly, I think in sort of that weight loss maintenance phase.
Melissa Joy (47:47):
Linda?
Linda Gigliotti (47:48):
Yeah, I think it’s important for RDNs who are practicing in this space to stay up to date, gain knowledge, and there are so many ways to do that.
What I have found most valuable is to connect with other colleagues in obesity care, not just RDNs. Talk to the physicians, talk to nurse practitioners, talk to pharmacists, work with them. I’ve gained so much working with interdisciplinary teams and talking with colleagues and other disciplines.
Look at some of the organizations that are now focused around obesity care: The Obesity Society for one, Obesity Medicine Association — just get on their websites, see what they’re posting, some of them have continuing ed, see who’s doing the writing, find out who’s doing the research.
I love following people on LinkedIn, and one person leads to another and who’s commenting, and follow some interesting sometimes debates or discussions. Because this is evolving, you can be really on the cutting edge in finding out what’s going on. Read the research from reputable sources, look at evidence-based journals, sign up for the continuing education that’s available.
As we mentioned earlier, the Academy and Academy Foundation offered a three-part webinar series last year, which are readily available on the Academy website. And again, this year, April, May, June of 2025, there are three more webinars that will be available at no cost on various aspects of using these medications.
Melissa Joy (49:28):
Excellent, yes. And I will have all the links to the article that we’ve been discussing, the academy’s webinar series, the other resources that we’ve been talking about, the other articles and so on. I’ll have all of those links in my show notes at soundbitesrd.com.
But was there any other resources? I know Hope you were just recently on Jim Hill’s podcast with Holly, the Weight Loss And … Podcast. Was there any other resources that you wanted to call out that I’ll be including in the show notes?
Hope Warshaw (50:01):
So, Holly Wyatt, she’s an endocrinologist. And Jim Hill, many of us know, they’re both at University of Alabama, and their podcast, which is Weight Loss And …, I’m finding valuable to listen to. They certainly have some good perspective. And certainly, Melissa, the episode that you did with Jim, I thought was really, really good, and you covered a lot of ground.
And Linda mentioned the next series of webinars that the Academy Foundation is sponsoring. And we’ve invited Jim to be one of the speakers on the third. So, I expect that he will creatively explore some of the things he’s thinking about in terms of how do we use these medications in weight loss maintenance. Those are really a few things. Looking at references in recent papers is a good thing to do as well.
Melissa Joy (51:07):
Yes, and just to reiterate, for those of you listening who are not healthcare professionals — if you are interested in these medications, if you’re taking these medications or a loved one, family member, friend, it’s never too late to see an RDN and to get that advice, and it’s very, very valuable. Hopefully, we’ve made that point very clear.
Well, Linda and Hope, thank you so much for coming on the show and sharing all of this wonderful information.
Linda Gigliotti (51:32):
Thank you for having us.
Hope Warshaw (51:33):
Thank you, Melissa. Great to be back with you.
Melissa Joy (51:35):
Alright, and for everybody listening, as always, enjoy your food with health in mind. Till next time.
[Music Playing]
Voiceover (51:44):
For more information, visit soundbitesrd.com. This podcast does not provide medical advice, it is for informational purposes only. Please see a registered dietitian for individualized advice.
Music by Dave Burke, produced by JAG in Detroit Podcasts, copyright Sound Bites, Inc. All rights reserved.
LISTEN, LEARN AND EARN
Listen to select Sound Bites Podcasts and earn free CEU credits approved by the Commission on Dietetic Registration (CDR) for registered dietitian nutritionists and dietetic technicians, registered. Get started!
Get Melissa’s Sound Science Toolkit here!
Partnerships:
Sound Bites is partnering with the Association of Diabetes Care and Education Specialists (formerly the American Association of Diabetes Educators)! Stay tuned for updates on the podcast, blog and newsletter!
Sound Bites is partnering with the International Food Information Council! Stay tuned for updates on the podcast, blog and newsletter!
Sign up for my monthly newsletter and episode eblasts so you never miss an update!
Listen on Stitcher (Android)
Install the Stitcher App
1. Search for “sound bites with melissa joy dobbins” 2. Choose Play Current Episode or Add to Playlist
Choose “Play Episode”
Subscribe & Review on iPhone
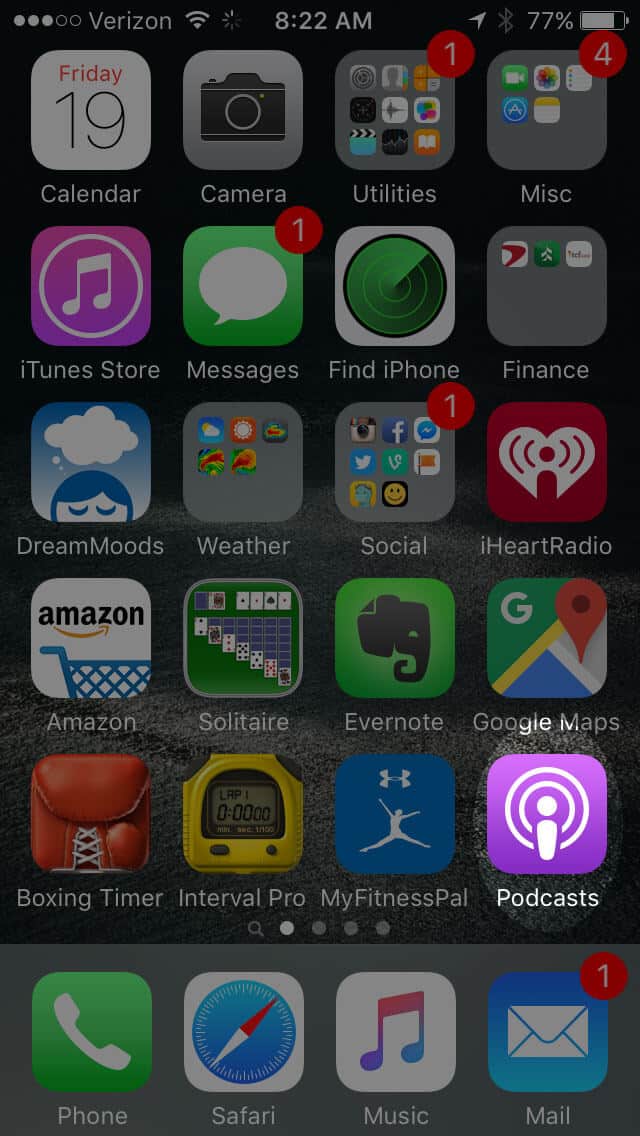
Open the “Podcast” app on your iPhone
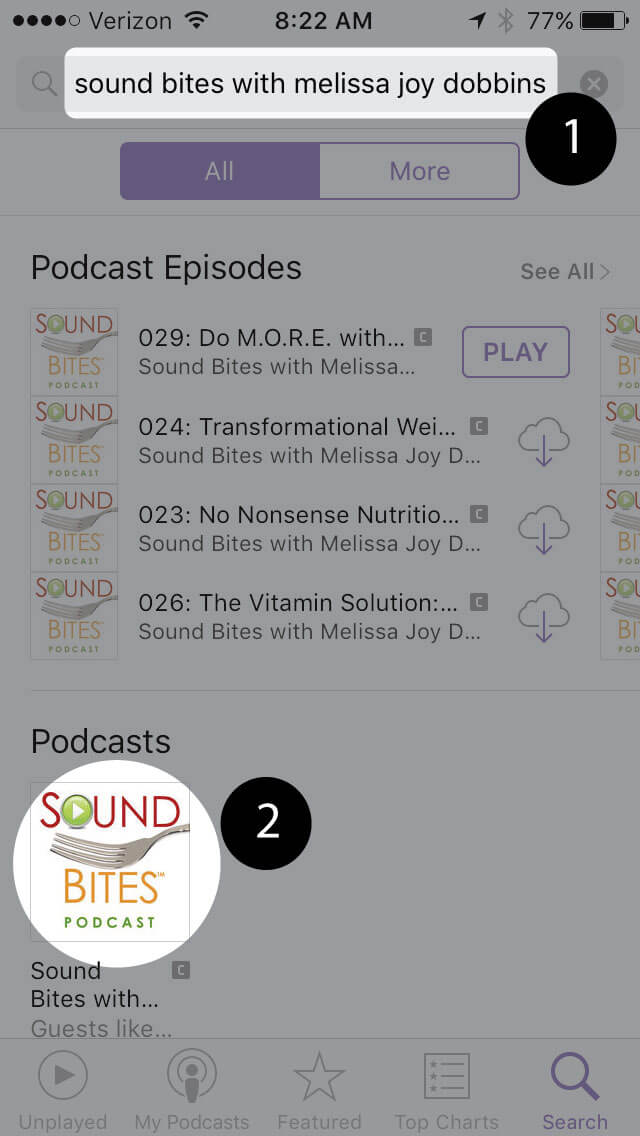
Search for “Sound bites with melissa joy dobbins”
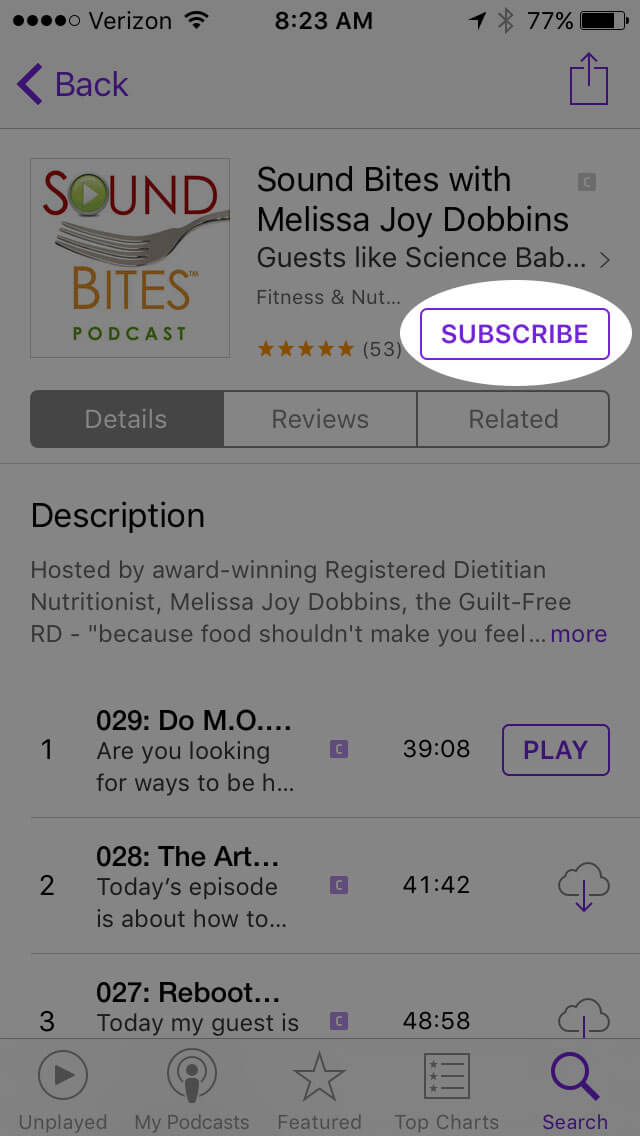
Open the podcast and click “Subscribe” and your done!
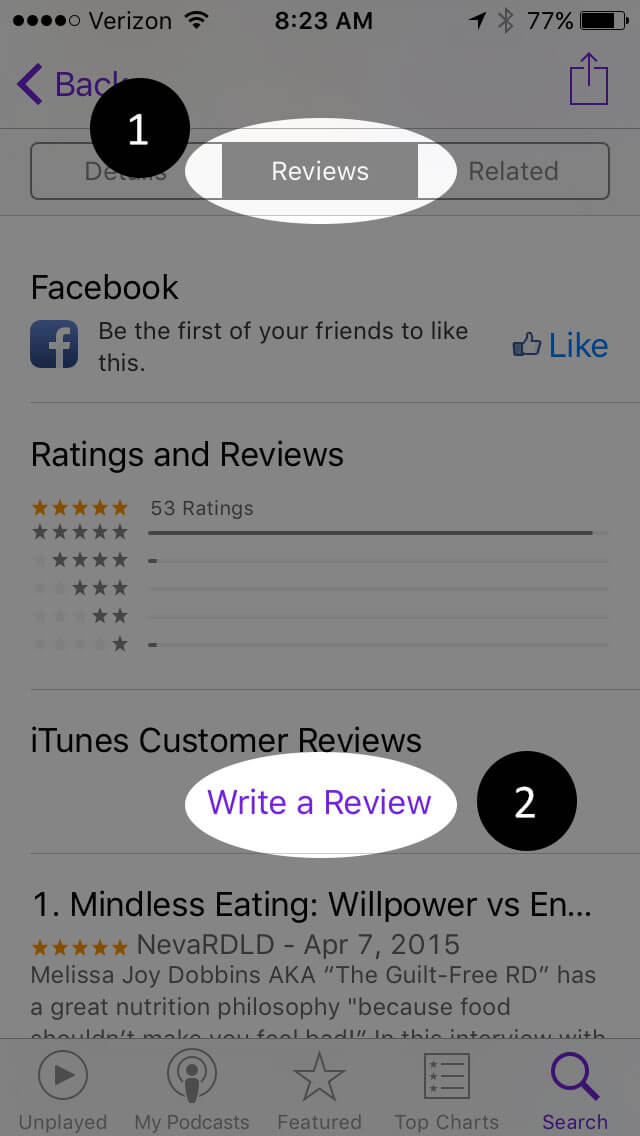
Write a Review
Click “Reviews”, then “Write a Review”.
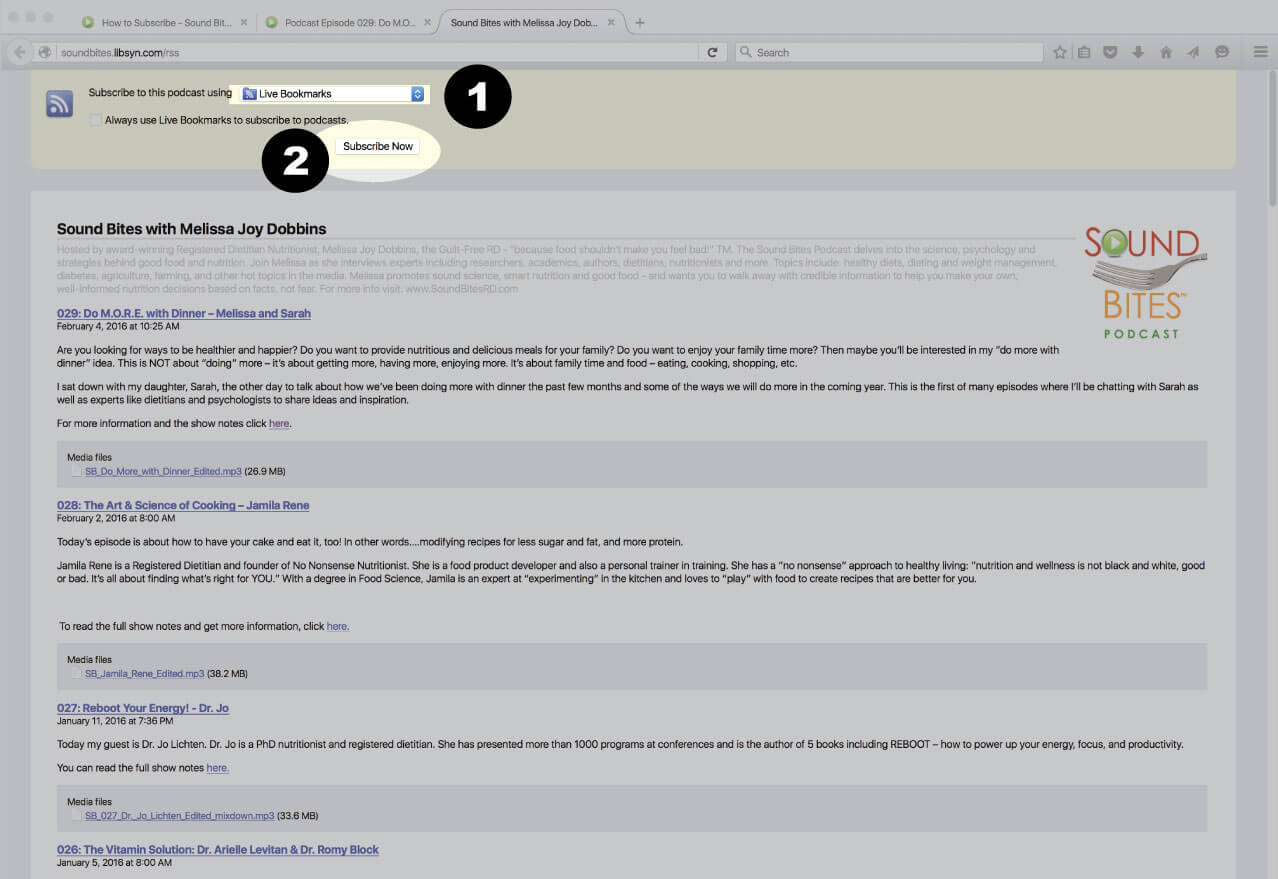
Subscribe via RSS Feed
Navigate to any podcast player . Click on the RSS feed icon.
Click on the RSS feed icon.
Click on RSS Feed
Choose which application you would like to use to receive the RSS feed
Click “Subscribe Now”
Confirm settings and subscribe.
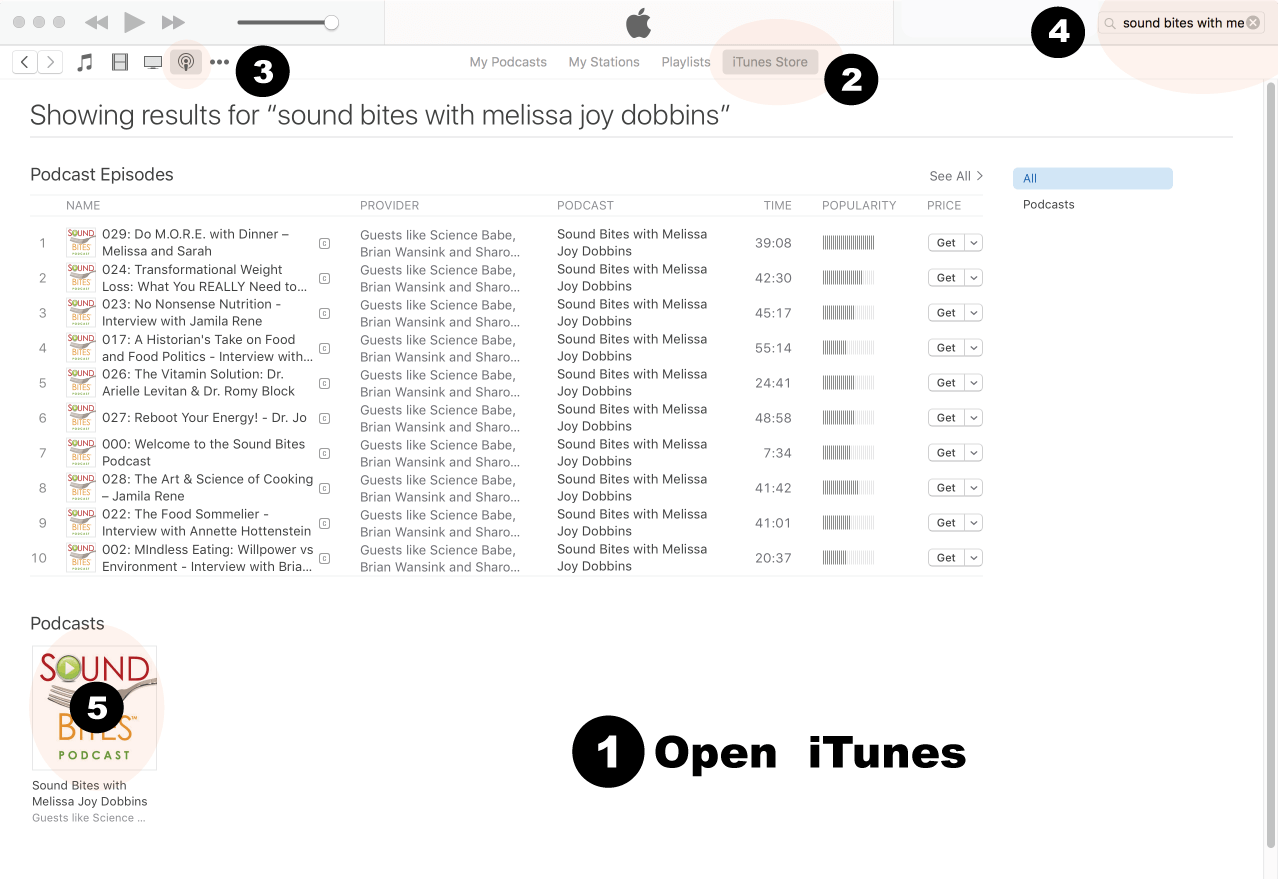
How to Review in iTunes
Open iTunes desktop application
Click iTunes Store
Click on Podcasts
Search for “Sound bites with Melissa Joy Dobbins”
Click on podcast image
Search for Sound Bites podcast in iTunes
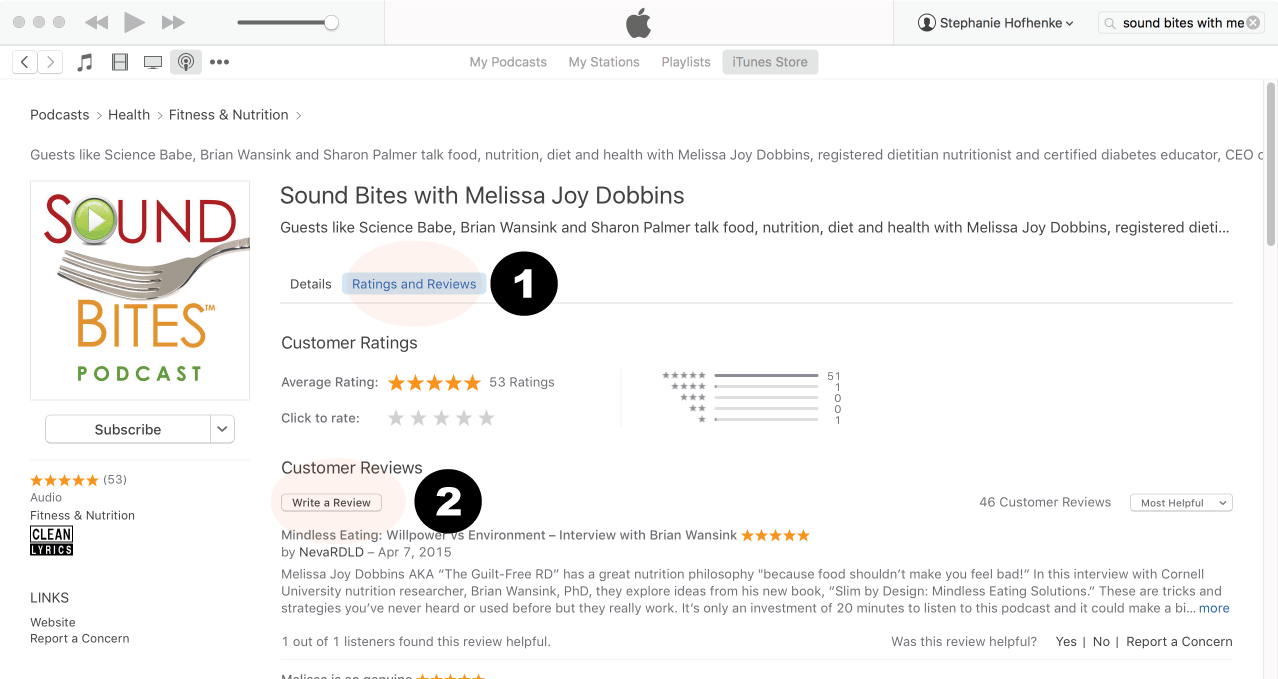
Click Ratings & Reivews
Click Write a Review
View reviews and write your own review.
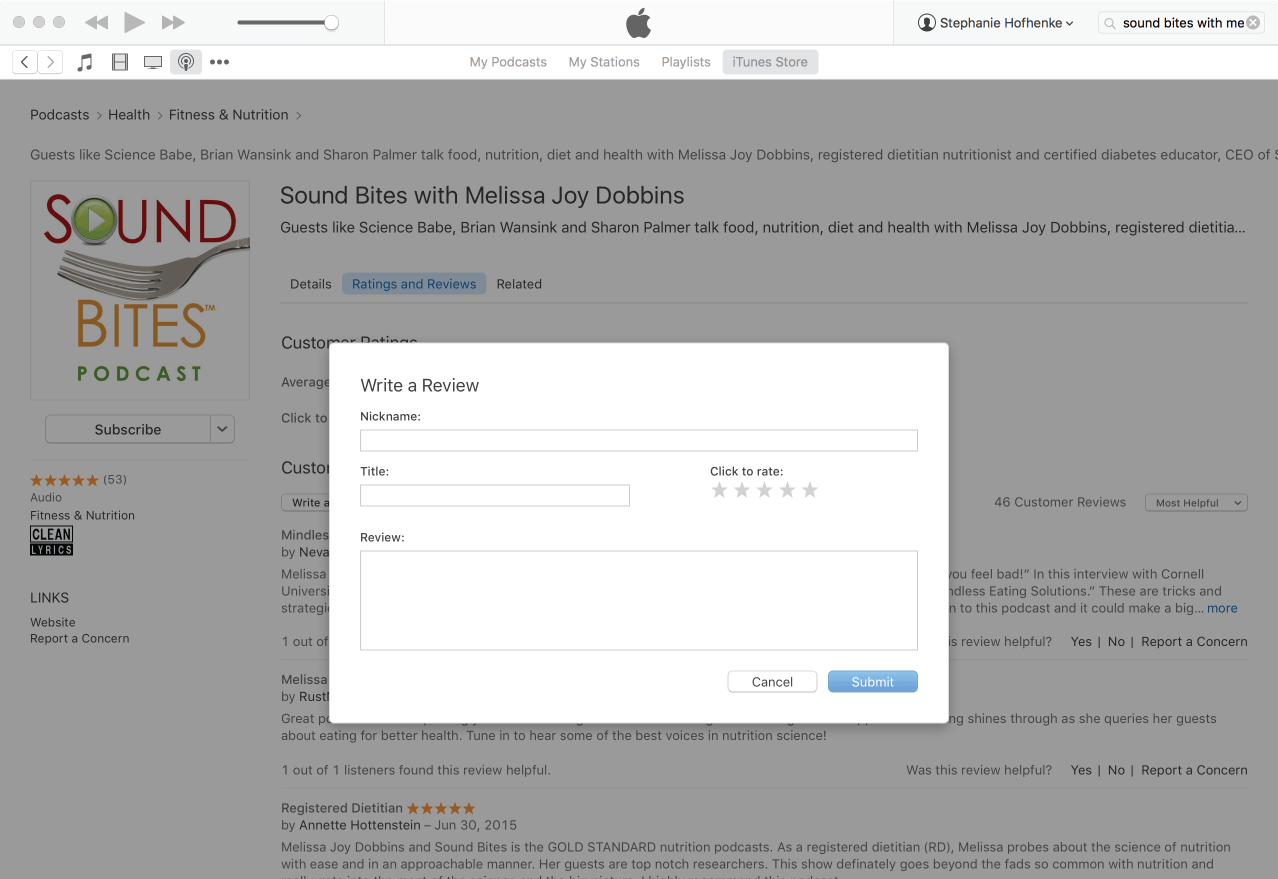
Write your review…. Thank you!
Write your review!
How to subscribe via iTunes
Click here to view the Sound Bites Podcastin iTunes, then click the blue “View in iTunes” button. This will open your iTunes application directly to Sound Bites Podcast. Click the “Subscribe” button, and your done!
 Linda has extensive experience in the clinical practice of adult weight management and multidisciplinary obesity treatment teams, having served as the Program Director of the Weight Management Program at the University of CA, Irvine for 20 years. She is co-editor of the Health Professionals Guide to Obesity and Weight Management, recently published by the Academy of Nutrition and Dietetics. Currently she serves on the Academy Foundation Board of Directors. Gigliotti is board certified in diabetes care and education and was engaged in the development of the interprofessional Certified Specialist in Obesity and Weight Management (CSOWM) credential. In 2021 she was awarded the Medallion Award by the Academy of Nutrition and Dietetics. She is also a recipient of the Excellence in Weight Management Practice Award by the Weight Management Dietetics Practice Group in 2017 and the CA Outstanding Dietitian of the Year Award in 2018.
Linda has extensive experience in the clinical practice of adult weight management and multidisciplinary obesity treatment teams, having served as the Program Director of the Weight Management Program at the University of CA, Irvine for 20 years. She is co-editor of the Health Professionals Guide to Obesity and Weight Management, recently published by the Academy of Nutrition and Dietetics. Currently she serves on the Academy Foundation Board of Directors. Gigliotti is board certified in diabetes care and education and was engaged in the development of the interprofessional Certified Specialist in Obesity and Weight Management (CSOWM) credential. In 2021 she was awarded the Medallion Award by the Academy of Nutrition and Dietetics. She is also a recipient of the Excellence in Weight Management Practice Award by the Weight Management Dietetics Practice Group in 2017 and the CA Outstanding Dietitian of the Year Award in 2018. Hope has been a Registered Dietitian and Certified Diabetes Care and Education Specialist during her career that now spans 45+ years. Her work has ranged from counseling people with all types of diabetes and weight management concerns, to corporate consulting, freelance writing and book author. She is recognized nationally for her expertise and as a committed volunteer for several organizations including the Academy for Nutrition and Dietetics and the Association for Diabetes Care and Education Specialists. She has held national elected positions for both organizations. Currently she serves on the Academy’s Nominating Committee. Related to the content of this Sound Bites RD episode, over the last couple of years Hope has worked with the Academy’s Foundation, for which she served as chair in 2022-2023, to advance and enhance the role of the RDN in obesity care specifically with the incretin-based therapies/GLP-1 medications. In this role Warshaw worked closely with the Academy’s Foundation leadership to develop a successful webinar series held in early 2024. Another series co-led by Warshaw and Gigliotti on this topic is in development for early 2025. Additionally, Warshaw is a co-author on a publication: Incretin-Based Therapies and Lifestyle Interventions: The Evolving Role of Registered Dietitian Nutritionists in Obesity Care, recently published in the Journal of the Academy of Nutrition and Dietetics.
Hope has been a Registered Dietitian and Certified Diabetes Care and Education Specialist during her career that now spans 45+ years. Her work has ranged from counseling people with all types of diabetes and weight management concerns, to corporate consulting, freelance writing and book author. She is recognized nationally for her expertise and as a committed volunteer for several organizations including the Academy for Nutrition and Dietetics and the Association for Diabetes Care and Education Specialists. She has held national elected positions for both organizations. Currently she serves on the Academy’s Nominating Committee. Related to the content of this Sound Bites RD episode, over the last couple of years Hope has worked with the Academy’s Foundation, for which she served as chair in 2022-2023, to advance and enhance the role of the RDN in obesity care specifically with the incretin-based therapies/GLP-1 medications. In this role Warshaw worked closely with the Academy’s Foundation leadership to develop a successful webinar series held in early 2024. Another series co-led by Warshaw and Gigliotti on this topic is in development for early 2025. Additionally, Warshaw is a co-author on a publication: Incretin-Based Therapies and Lifestyle Interventions: The Evolving Role of Registered Dietitian Nutritionists in Obesity Care, recently published in the Journal of the Academy of Nutrition and Dietetics.