Celebrating over 1 Million Downloads and 50,000 Free CEUs on the Sound Bites® Podcast | NEW: Get 1 years’ worth of CEUs with the new 15-CEU Podcast Course
This episode is not sponsored. Dr. Jay Shah is the Chief Medical Officer of Aktiia, a digital health company working on a better way to track, analyze and optimize blood pressure over time.
New Technology Supports Behavior Change in Hypertension Management
Hypertension is the most common modifiable cause of death in the world and when consistently managed is one of the most powerful benefits for someone’s health.” – Dr. Jay Shah
Hypertension, or high blood pressure, is the most common modifiable cause of death in the world and affects 1.3 – 1.4 billion people worldwide including almost 50% of people over the age of 65. Consistently controlling blood pressure over time is the most crucial element in minimizing the risks of blood pressure driven diseases such as stroke, heart disease, heart failure, kidney disease, cognitive decline, vision loss, reproductive diseases and more. Consequently, episodic monitoring of blood pressure is antiquated as it does not assess blood pressure values consistently over time. New technology offers “continuous” blood pressure monitoring and personalized feedback on how specific lifestyle changes are impacting blood pressure levels. While only 50% of people with HTN are “salt sensitive” there are some dietary modifications that can reduce the intake of sodium while keeping flavor in mind.
What really matters with blood pressure is not one point at any given time or episodic measurements. It’s what your blood pressure is over time, and how much of that time is your blood pressure in an optimal range or out of that optimal range. Expert guidelines have started recommending routine repeated and frequent measurements out of the office because we know that those one-time office measurements are really not reflective of this physiologic parameter.” – Dr. Jay Shah
Tune into this episode to learn about:
Hypertension (HTN) facts – definition, prevalence, diagnosis and management
Typical diet and lifestyle recommendations for HTN
Why episodic monitoring of blood pressure (BP) is antiquated
Average intake of and dietary recommendations for sodium
How only 50% of people with HTN are salt sensitive
How technological advances can help improve BP monitoring and management
The Hawthorne effect
How to seek out a registered dietitian nutritionist for guidance and support
Resources for health professionals and the public
It’s never too late to start or make a change. Seek out the services of a Registered Dietitian Nutritionist – you can find one at eatright.org.” – Angel Planells
Jay Shah, MD, FACC
Dr. Jay Shah is a renowned cardiologist who has over fifteen years of medical expertise and leadership in healthcare delivery from city general hospitals to community settings to the Mayo Clinic. He has brought his experience and expertise to the Swiss startup Aktiia to change the paradigm of how the world’s most common disease – hypertension – is understood and managed. Also an angel investor and advisor, he is passionate about applying technology to solve practical problems in medicine and believes strongly in the power of positive thinking and collaboration. Dr. Shah earned his Bachelor of Arts and Doctor of Medicine degrees at the University of Missouri, Kansas City School of Medicine and trained at Massachusetts General Hospital in Boston and Washington University School of Medicine in St. Louis.
Angel Planells, MS, RDN, FAND
Angel is a Seattle-based RDN, owner of a private practice consulting firm and National Media Spokesperson for the Academy of Nutrition & Dietetics. He is a former president of the Washington State Academy of Nutrition and Dietetics and Greater Seattle Dietetic Association. Angel has been honored for his work as chair of the Academy’s National Organization of Men in Nutrition member interest group for recruiting and retaining men in the nutrition and dietetics profession. He is also a member of the Academy’s Healthy Aging dietetic practice group and earned a certificate in adult weight management. He is a graduate of Tulane University and earned a master’s degree from Columbia University.
[00:00:01] Melissa Joy Dobbins: Welcome to Sound Bites, hosted by registered dietitian nutritionist Melissa Joy Dobbins. Let’s delve into the science, the psychology, and the strategies behind good food and nutrition.
[music]
[00:00:22] Melissa: Hello and thank you for listening to this episode. Please stay tuned after the episode for some additional information regarding salt and sodium that you may find helpful. I hope you enjoy the episode.
Hello and welcome to the Sound Bites Podcast. Today’s episode is about hypertension or high blood pressure, and how advances in technology have given rise to an entirely new way to approach this disease, to be more proactive and preventive than we traditionally have been, and finally begin to get a handle on managing one of the most common modifiable causes of death in the world. My guests today are Dr. Jay Shah and registered dietitian nutritionist Angel Planells. Dr. Jay Shah is a cardiologist with over 15 years of medical expertise and leadership in healthcare delivery spanning city general hospitals to the Mayo Clinic.
He has brought his experience and expertise to the Swiss startup Aktiia to change the paradigm of how the world’s most common disease, hypertension, is understood and managed. Angel is a Seattle-based registered dietitian with 17 years of experience and expertise in aging and nutrition, behavior and lifestyle modification, men’s nutrition, and obesity and weight management. He is also a national media spokesperson for the Academy of Nutrition and Dietetics. Welcome to the show.
[00:01:40] Dr. Jay Shah: Thank you so much for having us, Melissa, it’s great to be here.
[00:01:43] Angel Planells: Thank you for having us.
[00:01:44] Melissa: My pleasure. I’m very excited about this topic and this technology that we’re going to be discussing today but I want our listeners to know that this episode is not sponsored and we may be submitting this episode to the commission on dietetic registration for continuing education credits. If that is of interest to you, you could always check out my free CEU page on soundbitesrd.com.
Dr. Shah and Angel, I would love for each of you to share a little bit more about your background, perhaps your education, and the work that you do with particular emphasis on hypertension the topic that we’re discussing today. Maybe how you got interested or ended up working in that niche, and anything else that you would us to know about your background and of course, as always, any disclosures to note, Dr. Shah, let’s start with you.
[00:02:32] Jay: Thanks, Melissa. As you said, my name is Jay Shah. I’m a cardiologist. I’ve been in practice in the United States for over 15 years. I did my medical school at the University of Missouri in Kansas City, which was a very much a city general hospital and it was a fun place to be a medical student because you were assisting in operating rooms and because chronically they were short-staffed. Then I did my residency at Massachusetts General Hospital, which gave me this great broad lens with which to view medicine. I met some phenomenal people and leaders of many companies and healthcare organizations around the world while I was there.
Did my cardiology training at Washington University in St. Louis. That gave me a really strong grounding in clinical practice and really how to be a great clinical cardiologist. I went out, did something quite a bit different, and started my own practice, in Portland, Oregon. Its not done these days very often and built that up over seven years. For the last three years, came down to Mayo Clinic to start their thoracic aortic disease program in Arizona – built that program.
For all these years of practicing cardiology, have really been seeing people after the fact, after some problem has occurred, after they’ve had a heart attack, after they have developed a major aortic aneurysm, after cardiac surgery, after some hospitalization for some problem. That’s really how the medical system is designed. It’s designed to react to some problem, some symptoms, some issue that has already occurred. What really got me interested in the work I’m doing now at Aktiia is really trying to look at and trying to make a broader impact before those major diseases take shape or have an event.
Before the person and the patient sit in my office and ask me, doc how could I have prevented this? Because almost always, in cardiology at least, the answer is this started decades ago with chronic diseases and the most common is high blood pressure or hypertension. That’s really what got me interested in this space. Then I have had a career shift at this point in my life wanting to take this deep clinical experience and then apply it to a much broader pathway to hopefully impact many more people. That’s what got me here.
[00:04:59] Melissa: Excellent. I love this shift towards more prevention and your background is amazing, by the way. I went to University of Missouri, Columbia. Not the same but two hours away.
[00:05:10] Jay: Close.
[00:05:11] Melissa: Angel, let’s hear about your background a little bit.
[00:05:14] Angel: Sure. Born and raised in New Orleans, Louisiana. I’ll be brief, but I guess originally, since I lived in New Orleans I was going to go into the petroleum industry. I had a scholarship doing chemical engineering and everything was very exciting. Then I found out that I liked speaking with people. I did enjoy the calculating the numbers and playing on the computers, but I was looking for some connection with people. I met the chairperson for the exercise sports sciences department, and he was a sports psychologist and he worked with all these professional athletes and teams and I was like, I want to be that guy.
In the process, I ended up taking a sports nutrition course. We got to try every diet for a week and actually document how we felt about all the different things and it piqued my interest in this. I was a former athlete, played soccer, ran track, ran cross country, played a bunch of sports and I guess the question was if clearly some people are genetically blessed and they’re able to do a lot of things, but would nutrition be the difference between someone playing high school and college or college and professional? That was my entry into the field.
I was going to go get a PhD in sports psych. I moved to New York City to go to Columbia for grad school. I did the exercise physiology and nutrition route and, very fascinating – I guess the goal was going to be a one-stop shop that allowed me to do exercise psychology and nutrition. In the process living in New York City, it’s expensive and we got to probably get a job. If I won the lotto, I’d probably donate money to a school and go to school the rest of my life. Instead, I said let’s do the dietitian thing. I’ve been doing it ever since and yes, I’ve been doing this for 17 years.
The PhD dream for sports psychology probably has died because clearly, I have two children. They’re about to turn 10 and 14 next week or actually this week. Life pushes you in mysterious ways. Career-wise, I worked with Sodexo, I’ve worked with the VA doing home care for many years. The last four years I’ve been the vice president for a consulting company here in the northwest dealing with accounts in Washington and Oregon. My interest it’s not necessarily hypertension per se, but it’s just overall heart health, and improving quality of life for individuals has been my main mainstay.
Working with the VA, we got to work with a lot of individuals looking at high blood pressure, cardiac disease, and men’s health in general and just trying to improve. The sports nutrition aspect, working with the veterans was great because I’m dealing with former athletes and how can we improve their quality of life. One of the things with athletes is they finish their career and they eat the same way.
We’re going to talk about habits because these habits end up being lifelong and how can we modify the habits back to what the current setup is. The other interesting thing is physical activity almost ends up becoming a dirty word for some people. It’s scary and it’s like, we can modify our thought process to do activities that are enjoyable for you. I’m just excited to be here.
[00:08:17] Melissa: Great. Reframing the exercise piece for sure. I know we’re going to talk a lot about lifestyle modification and behavior change. It’s a huge aspect that this new technology that I’m teasing at the top of the interview here is going to connect with that behavior change component in a really interesting way. Let’s set the stage with some hypertension facts and statistics. Dr. Shah, should I call you Dr. Shah, Jay?
[00:08:42] Jay: It’s fine to call me Jay.
[00:08:43] Melissa: Okay. Jay, please give us a primer on high blood pressure. What is it, how prevalent is it and why is it important to manage it? Anything that we need to know to set the stage here?
[00:08:54] Jay: I’ll give you pretty much three bullet points, to start. One, it’s the most common disease in the world, 1.3 to 1.4 billion people around the world have it. 130 million Americans have it. It is the most common, as you said in your introduction, is the most common modifiable cause of death in the world by far. What is it? People often just think about it as a risk factor. That’s how it’s talked about. That’s how we talk about it in medicine oftentimes it’s a risk factor for some other problem. It’s a risk factor for a heart attack. It’s a risk factor for stroke, but actually, it’s a disease.
Disease and risk factor are two different things. Age is a risk factor that’s not modifiable. It’s not really a medical problem per se but we know as we get older, things happen and we get sick, in different ways. High blood pressure is a disease. Hypertension is a disease that affects almost 50% of seniors, people over the age of 65, around the world. It causes higher pressure within the arteries all throughout our body. Over time, over long periods of time. Not one day, not one week, not one month, but months to years and years to decades.
Over that period of time, it creates higher pressure on the underlying organs of our body, all our organs, and there are many organs that are sensitive to that higher pressure. We commonly talk about cardiovascular disease and it is a very prevalent one but brain health in multiple aspects is quite sensitive to this higher pressure. Not only do strokes result from high blood pressure or hypertension over decades but cognitive decline has been closely linked to high blood pressure.
There are multiple types of cognitive decline in dementia. Vision loss, high blood pressure is one of the most common causes of retinal disease in the world. It affects our heart in many different ways, heart failure, heart attacks, arrhythmias, it affects our aorta the big artery of our body causing aneurysms that affects our kidneys and it causes chronic kidney disease over the long term. It affects our reproductive system and causing either erectile dysfunction, or even in younger women it can cause pre or postpartum or peripartum around the time of pregnancy high blood pressure that can lead to problems over a long period of time.
It affects many different organs of our body but the key feature is that it does it over a long period of time and that is something that makes the idea of hypertension challenging to a lot of people for all the reason that Angel is going to talk about. Behavioral science and making changes of real lifestyle have to be done over a long period of time and have to be done consistently over many many years.
[00:11:42] Melissa: Thank you. One of the things that I always remember learning about it and then I had a personal experience, which I’ll probably share a little later, is typically there’s no symptoms. It’s considered a silent disease. There’s so many parallels between high blood pressure, hypertension, and diabetes where you might have it for a long time, not really having symptoms. With diabetes there are symptoms but as the blood sugar gradually goes up, you don’t really notice. You might have it a long time before being diagnosed.
I’m sure this happens a lot with hypertension and maybe you can speak to that as well but again those parallels there. Let’s talk a little bit Dr. Shah before I ask Angel about some of the dietary and behavior modification stuff because I do want to address the medication aspect. Like you said, it’s the most common disease. The first line of therapy typically is going on – there are a variety of blood pressure medications but I would love you to address that.
[00:12:40] Jay: Going back to your previous point of not having symptoms. This is also part and parcel of one of the most complex things about hypertension is that for many years people might develop the disease, especially in younger years when they’re not really interacting with healthcare on a routine basis. 20s, 30s, 40s of life that’s when hypertension really actually starts to develop but it’s also the time during which people are least engaged with the health care system and are not really paying attention to their health, most of us at least because we’re young.
Then you don’t really need to go to see a doctor. I don’t feel anything. I don’t have any symptoms. Why should I be aware but that’s actually the time when you have the opportunity to make the most difference because once something occurs when somebody’s 50, 60, 70 years old the horse is out of the barn so to speak. Now, yes, it’s important to control blood pressure after an event but the damage has been done so to speak.
[00:13:39] Melissa: That’s similar with diabetes as well, right? That long chronic.
[00:13:42] Jay: Exactly. Getting to your question about first line of therapy it depends. When somebody actually comes to a diagnosis of hypertension which may be, as you said years to decades after it started. Once they do come into a physician’s office and somehow gets a formal diagnosis it depends on what level their blood pressures are. There are different stages of hypertension that are classified by national and international guidelines and the higher the level and the higher the stage of high blood pressure, the more likely it is that somebody’s going to initially get a recommendation of medications but that will always be with an additional recommendation of certain lifestyle changes. Always.
If somebody is in an earlier stage of hypertension or a less significant less severe elevation of their blood pressure then actually for the first three to six months, the recommendation by the guidelines is to do significant lifestyle changes, behavioral changes, and modifications. We can talk through what those are and then to see how it goes, to see what happens, to see if that person is able to modify their own blood pressure with certain interventions. The interventions that we typically talk about outside of medications are everyone’s going to know these. There’s no mystery here.
It’s going to be diet, looking at sodium, looking at calorie reduction, looking in trying to lose weight, exercise, alcohol reduction, sleep hygiene, among certain others. Smoking is another one. This is a very common laundry list of lifestyle interventions and one of the things that’s difficult and as we start talking about the behavioral aspects of it, is that we give that laundry list to everybody, irrespective of who they are, where they come in their socio-economic background, lifestyle, cultural background. Everyone gets the same laundry list of six seven things to do.
They get it within 10 minutes or so or whatever time they’re sitting in the office, and they say, now go do that. Go execute on these things. Even one of those aspects, let’s just take sodium reduction as an example, even to be diligent about sodium reduction is so incredibly difficult. How can someone possibly be expected to do seven different things when just minimizing your salt intake to 2,300 milligrams or 2,000 milligrams a day, I won’t say it’s impossible, but it’s close to impossible in this day and age in Western culture. It’s an extremely difficult thing.
That’s why unfortunately, most physicians healthcare, we talk about lifestyle, we do recommend it but really, what generally people go to is a pill or multiple pills as medications. There is a fairly standard approach to medication management with hypertension, not very individualized, everyone gets the same standard regimen of medications in the same order roughly and they do work. They do improve health outcomes, but people are on medications then and generally it’s indefinitely. It’s the rare person at least in my practice that are able to come off medications, or to reduce their medications because they have done so much work on their lifestyle.
[00:17:10] Melissa: I appreciate you addressing that. Again, there’s the parallels there with diabetes and I always say on the show medications get a bad rap, people don’t want to be on them, there’s risks. I know I say that this is a conversation that you need to have with your healthcare provider about the risks and the benefits and which medications might be the right one to try first and second and so on. Yes, it doesn’t mean that the lifestyle modifications don’t matter, they do. Those things can be in conjunction but having been a certified diabetes educator for 25 years, I just feel like that is such a common conversation that I would have with patients.
I would reassure them like, “Yes, you’re doing the best you can with lifestyle. We continue to try to do better but the medication is there to help you.” Again, teasing my personal story of what I’ll talk about a little bit later, is those side effects are real. Again having an open conversation with your healthcare provider and trying to figure out what might be the best choices for you is an ongoing thing and sometimes people don’t necessarily feel like they can have the time to talk with their doctor or have the courage to ask questions, and all of that that goes into it.
Thank you for addressing the medication. If there’s anything that comes up regarding medication as we move forward, I’d be open to hearing about that. Angel, let’s talk about the diet, the lifestyle, how you would work with a patient top line, because as you and I talked about before the interview, I want to get into the technology sooner rather than later and then circle back with, whether somebody is using this technology or not, what can people do to better manage their blood pressure? Just like Jay talked about the typical laundry list of what we give people, walk us through that bit.
[00:19:07] Angel: We’re all creatures of habits, and whatever lifestyle we grew up with, your parents could be preparing homemade meals every day, your parents could be eating out every day, you could have a mix in between, you could be very active, you could have been in sports, whatever. kids might be active in school and then they get into high school, some people drop activity, some people continue being active.
They get into college, you have the freshman 15 and people stop activity. We’re young, we’re invincible, you feel like you can live forever and then they meet you, Dr. Jay, maybe about 45, 50 and they might have had a cardiac event or something like that, , they might have gained weight, and now they’re coming to meet one of us. these habits have been put in over time, this is not like a snap your finger and congratulations, you have high blood pressure, this has been built in over time.
The interesting thing for me that I like to relate to individuals is, it’s taken you a long time to get here, what can we do to rectify this situation? Clearly, some things can be modified, eating, activities can always be better. We have to try to fit into people’s lifestyle because if you go in with a laundry list saying, “Do A, B, C,” and they eat out every day, , yes we could idealize and want things to be great. Perhaps, “Let’s do homemade meals every day, and you bring your homemade lunch and do all these things.”
The reality situation is a lot of people are busy, maybe they don’t have the cooking skills, working with the VA, you’d be surprised. I had a person that never made a sandwich or salad or a bowl of cereal in her life, my children can do that. It’s one of these that if we don’t have this experience, we have to try to meet them where they’re at. Going back to hypertension, clearly the recommended amount, 2,000 milligram. I know American Heart Association even wants 1,500, and the average American gets 3,400 milligrams a day.
[00:21:23] Melissa: At least.
[00:21:23] Angel: It is very easy to do it. it’s very easy to go above and beyond. It’s not just the table salt that people sometimes look at, it’s like, I can stop this but there’s other things. Clearly, lifestyle modification is wonderful and there’s always an opportunity for improvement, I’d like to say, because you can’t expect for someone to have 20 years of poor dietary habits and that they meet you for 10 minutes for Dr. Shah they might go in for you for 10 minutes. For me, I might get to spend 30 minutes with them and now they’re going to be an expert, not going to happen.
It’s constant follow up, it’s constantly checking in, and there’s apps and other things, label reading, and just making sure that they try their best. On top of that, Melissa, it would also be looking at improving overall dietary habits, not just looking at sodium, increasing the fruit and vegetable consumption, trying to incorporate more whole grains into there. Finally, as Dr. Jay mentioned, there’s physical activity, good sleep hygiene, a good advocate for mental health, making sure all of it is in check,
[00:22:49] Melissa: So, as we’re talking about blood pressure, and behavior change, all the things that we need to do, I’m just really curious to hear about this new technology, this company that you’re working with, Dr. Jay. I know that technology has been a game changer in the diabetes space and this sounds really interesting, we’ve got continuous blood glucose monitoring now. You’re going to talk to us about this new technology for monitoring and managing blood pressure.
[00:23:21] Jay: Aktiia is a Swiss company and the founders have been working for now almost 20 years on the underlying technology that we’ve commercialized and are in the market in Europe and the UK, where it’s an optical based device, so a device that’s just worn on the wrist, where passively the person doesn’t have to do anything. We get multiple readings, about 27 or so readings, every day of blood pressure and heart rate. It’s not continuous in the sense where it’s every second beat to beat measurement of blood pressure but it’s continuous in the sense that you don’t have to do anything to really activate it to measure your blood pressure.
In the course of a week, you might get 200 blood pressure measurements a week, 800 in a month. The first question would be, why do you need all those measurements? Don’t we just check it one day, and then we’re fine, we know what it is? The truth is just like glucose, or just like any other physiologic parameter, it continuously changes, your blood pressure never stays really just exactly the same. It might be in a range, but it’s continuously fluctuating up and down. Even the expert guidelines have really started recommending routine repeated and frequent measurements out of the office because we know that those one time office measurements are really not reflective of this physiologic parameter.
As I spoke about in the beginning, what really matters with blood pressure is not one point at one day, or one minute, or one time measurement or episodic measurements. It’s what is your blood pressure over time, and how much of that long period of time, months, years, decades, is your blood pressure in an optimal range or out of that optimal range? Really, there’s no tool that we have to really be able to measure that but that’s what matters for blood pressure, and so that’s what this company has developed.
That’s the primary innovative technology, is to be able to measure over a long period of time significant derangements of blood pressure and to really get a more accurate sense of blood pressure driven risk. That’s the underlying core technology but what we think about is, how do we actually make that meaningful to people? Because one thing that is largely true, at least from my experience in medicine is that people look at blood pressure and it’s just a number, don’t really have some sense of urgency to it, 140 over 90, maybe it’s a little high. I ran in the office today, I had two cups of coffee, I got a little anxious. It’s fine.
We have to make it meaningful to people. Angel was talking about, you have to meet them where they are, you have to meet each person where they are. That’s something we struggle with in medicine especially around hypertension or chronic disease in general is that we have this laundry list of things. Let’s say you have this innovative technology that gives you a sense of blood pressure over time and let’s say somebody’s out of their optimal range. What does that actually mean? What can we help that person do to individually make their measurements and make that behavioral change meaningful?
Here’s an example, just as an example, let’s take sodium, since that’s what everybody thinks about it, talks about it. Sodium reduction, we talk about it all the time when we talk to people who have high blood pressure. As Angel said, very difficult to do, you have to read labels, you have to do all this stuff. Even if you do, we also know that only 50% of people with high blood pressure are salt sensitive. That means for 50%, half the people we’re giving this advice to, it doesn’t really matter for them. The same goes for almost all the other stuff on the laundry list.
How do we really know if, we talked about alcohol reduction, but not everyone drinks significant amount of alcohol. We talked about weight loss? How much weight loss does it take to actually impact your blood pressure? There are plenty of people who have high blood pressure who really aren’t overweight. How do we make those recommendations meaningful to that person and show them that their behavior change or their interventions are making a difference?
If you start taking this longitudinal measurement tool of measurement and software that sits on their smartphone that’s with them all the time, and then start helping them do their own internal experiments, let’s do dry January and see what happens with your blood pressure pattern over a month and then decide, does alcohol really make a difference for your overall blood pressure pattern? So on and so forth.
Let’s look at a sodium challenge and let’s see if over a month or two, sodium reduction has actually made a difference, so that people can really focus on what matters for their blood pressure, and what matters for them, and really focus on optimizing individually their own blood pressure driven risk. That’s the software we build around the underlying core innovative technology. Hopefully, we can make it more meaningful and impactful to each person and therefore cement that behavior change that’s so difficult to maintain over decades much less a few weeks or months.
[00:28:29] Melissa: That’s what’s so exciting is at first glance, it’s like, continuous blood pressure monitoring, like we have continuous glucose monitoring, but it’s really this tool to help connect the dots with the management of the really exciting and that lifestyle behavior modification aspect, because we struggle with this. Again, we see this with diabetes, but how much time is the patient in the healthcare setting? The majority of their life is not in the healthcare setting, it’s outside the healthcare setting. How much time do they get with the doctor? Lucky if they get time with a dietitian. They’re the ones, and I know, Dr. Jay, you said this before the interview when we were having our call, that the patient is really in the driver’s seat.
I say that all the time. The doctor’s not, the patient is the one who has to decide what they’re going to do and how they’re going to do it. We can all support them but that’s what I find is really exciting about this new technology is the behavior change component. Talk to me about how is it being used now with patients. I know you’ve got some research studies but there’s also some practical results of real patients using it. How accessible is it? How affordable is it? Is this something that– How do people say, “Hey, I’m going to talk to my doctor about this?” How available is it?
[00:29:43] Jay: The first thing to say is that, just to be clear for the listeners, that right now we have regulatory approval across Europe and the UK and actually access to many other countries, but right now we do not have access to the United States. We’re moving through the regulatory approvals as far and fast as we can. We are looking to come into the US market, but it’s going to be over a year at least. Just to be clear and upfront. But in those markets where we have regulatory approval since all blood pressure devices are actually required to have regulatory approval, they’re class 2A medical devices, you can get it over the counter.
Just like any other blood pressure device, you can buy it yourself, you can buy it on our website, we get it shipped directly to you. We have many users where that’s the situation. They are just interested in a different, better, faster, easier, and more technologically advanced way to track and monitor, and hopefully optimize their blood pressure. We have also have several, many actually at this point, healthcare organizations and insurance companies even where they’re actually in care delivery settings where they’re deploying the technology over large patient populations and tracking all those patients in one place.
We have an enterprise software tool where one organization can track all the patients who are using our device, look at their blood pressure real-time and proactively without that person having to come into the office, proactively monitor and manage them and give them communications and be very proactive about it rather than the reactive way that we traditionally look at blood pressure. That’s kind of how it’s being used right now in the clinical setting.
We also have about 40,000 now real-world users. When we look at their real-world data, those that have consented for us to do some research on their data, we can see that those who are hypertensive to begin with when they start using the device and the software have a significant reduction in blood pressure over six months as compared to those who have normal or average blood pressures.
It’s called a Hawthorne effect in academic research. Even just the idea of exposing the people to their own data allows them to be empowered to say, “Let me go to my doctor, let me look up what can I do to really improve my blood pressure.” Then empowers them to really go and be proactive themselves. That is really where we really have seen a remarkable effect, even just people just using the device overall have managed to lower their blood pressure just from that alone.
[00:32:30] Melissa: I meant to ask also, can you address how accurate is it? I know that when CGMs first started in diabetes and also just even the monitors that were anything other than finger stick, different parts of the body. There’s a lot of questions and concerns about figuring out the accuracy. Talk to us about that.
[00:32:50] Jay: Accuracy is always going to be a question. We publish all our data. It’s all on our website. We’re very open about it. There are standard validation protocols for all blood pressure cuffs. We put our device through that same slightly modified, because it works in a different way, through that same validation protocol, we meet the standard criteria for accuracy as a cuff does. Now, the thing is, is that that standard criteria for accuracy for a cuff only exists in one position in environment only. That is the seated, relaxed body position.
Not only that, it’s seated, relaxed feet against the floor back against the chair. Should not have eaten for 30 minutes, no alcohol for 30 minutes, no smoking. You should not have exercised. There should be no noise. You should not speak. No one should speak to you. Your arm should be free of clothing. Your stomach should be empty, and you needed to have gone to the bathroom before you sat down. That is the one and only environment that all cuffs are validated in. Just think about that for a minute.
[00:33:53] Melissa: I know. Whenever I see my husband taking his blood pressure laying down, I’m like, what are you doing?
[00:33:58] Jay: There’s no validation for that. Is that a real-world situation for valid– Is that our real-world environment? No. The thing is that our device takes blood pressure measurements in different body positions. When you’re standing, when you’re lying down, if your arms over your head, if your arm’s down by your side. We have validation data for all those positions. We compare, there’s no cuff data you can compare to because never been done before.
We compare to a very rigorous protocol that we call double auscultation, which is a person listening to the arm with the stethoscope, the traditional way to check blood pressure. Two people at the exact same time with a bifurcated stethoscope and a mercury column. It’s the most accurate way that we can possibly measure a noninvasive blood pressure. That’s our benchmark. That’s what we compare to.
[00:34:47] Melissa: Interesting. I was reading some of the materials and it’s kind of interesting if you want to explain how the sensor analyzes the arteries below the skin surface. Does that just count pulses? Can you just address that?
[00:35:00] Jay: Correct, yes. It uses LED lights to shine light into your capillary bed. It’s not sitting on your artery, it’s not compressing your arm, and there’s no sensation to it. It’s just light shining into the skin. You won’t feel it. It gets a reflection back to the optical sensor. That reflection tracks the capillary blush or the waveform with every heartbeat, the capillaries or the tiny arteries in our skin fill with blood and then get smaller.
It tracks that and then creates these waveforms and each measurement takes into account many, many tens of those waveforms and that’s sent to our server where the algorithm really works on it. That’s what’s proprietary. There’s nothing in the sensor that’s proprietary. It’s just standard optical sensors and lights. Our algorithm, that’s what our founders really developed over two decades. It works mathematically computes the blood pressure based on those optical signals.
[00:35:58] Melissa: Interesting.
[00:35:59] Jay: Then it delivers the blood pressure back.
[00:36:01] Melissa: I understand it even works while sleeping.
[00:36:03] Jay: For sure.
[00:36:03] Melissa: You already addressed it’s much more than just one point in time just like with checking blood glucose, but is there anything in particular about sleeping that’s important, like why would need to measure then?
[00:36:13] Jay: Yes. We typically don’t measure it while we’re sleeping. Sometimes people do, very rarely people do something called an ambulatory blood pressure monitor, which is a giant cuff and a bulky setup that someone takes home for 24 hours, and every 15 minutes, it squeezes your arm. Anyway, that’s the only realistic way to get nighttime blood pressure at this point in time. With our device, there’s no sensation. It’ll go off while you’re sleeping and it’ll take measurements while you’re sleeping. The patterns while you’re sleeping have been shown to correlate significantly to overall blood pressure-driven risk, cardiovascular risk.
Getting those nighttime patterns can be very helpful. Even with the data that we currently have, there’s a lot of data that we’re getting that we don’t really know what it means yet. Because there’s never been this kind of data set. Now we have almost 100 million blood pressure data points in our data set. We don’t really know a lot of what is hiding, what sort of nuggets or really insights yet. We’re starting to delve into the research to try to pick out those insights. For example, what parts of nighttime patterns are important and nighttime patterns change over time. Your nighttime pattern one year might be different than the next year, one month might be different than the next month.
We don’t really know. There isn’t a data set that exists out there that can guide us. We have many research partners across the world and we’re starting to do that research on really what else can we gain from this data set. It’s very similar to when CGMs came on the market for diabetes. This created this immense new data set that no one had ever seen before. Really, you’d been getting glimpses of it with snapshots of the finger sticks, but really never seeing the full picture. Now you have a world in diabetes where time and target range has become a primary metric of treatment that only can exist with the advent of CGMs. We’ll see some of these other metrics come out in the blood pressure space similar to that.
[00:38:18] Melissa: Interesting. Anything that promotes and encourages conversation with the healthcare team and the patient is really important. As we’re heading towards wrapping up, I should share this, my short story since I’ve mentioned it a couple of times. Then I would love to talk more about what can people really do today with or without this technology and of course, we’ll let people know how to stay connected with you and up to date on things. With diet, it’s not just about the salt. We can’t not mention the DASH diet, right, Angel?
Also referring to dietitians, we need to have this conversation as well. Just real quick, my story about a year ago, first of all, I should say I’ve always had beautiful blood pressure. Never a problem, ever. About a year ago, I went on the hormone replacement therapy patch, and my doctor mentioned a couple of times, make sure you get your blood pressure checked within two weeks. She didn’t say this could raise your blood pressure, but she said it enough times where I was like, “Oh, this is important.” I was busy. There’s a lot going on. I almost didn’t do it, but I’m a rule follower and I respect my doctor and she’s great.
I said, “Oh, I really need to get my blood pressure checked.” I had my brother-in-law come over because he’s a doctor. He said something that upset me before he checked my blood pressure. It was 150 over 90. I was like, “What?” My husband said, “She’s kind of mad. You might want to let her rest a bit and cool off and then check it again.” I’m like, “Yes.” We did. We rested and checked it again. It was 150 over 90. I’m like “What?” My brother-in-law, he’s not my doctor. I love him, but right away, he said, “You need to lose weight, you need to cut salt out of your diet. You need to stop drinking alcohol.”
I was like, “You need to leave my house now.” I love you, but oh, my gosh it really scared me. I thought, I’m going to go to the doctor tomorrow and get it checked. It was still 150 over 90. My gynecologist said, “What should we do?” I said, “Maybe we should try going off the patch and see what happens,” because of course I was 99% sure that that’s why it went up, but I know it can go up with age, with menopause, weight gain, all of these things, so I was freaking out. We went off the patch. I bought a monitor to have at home. She said it could take about a week.
It did, but within a week I was beautiful numbers, I’m okay. In the meantime, my husband started using the monitor that I bought and brought home and we found out his was way higher than 150 over 90. That’s about all I can share due to HIPAA. You have to get my husband to agree to that. When I mentioned medication side effects earlier, the side effect of my hormone replacement therapy patch was high blood pressure. That became a real thing for me. I went through all of the things that I’m sure patients go through as like, “Did I do this to myself? What have I done?”
I will say with regard to sodium the thought of cutting sodium and salt out of my diet was just devastating, [laughs] because I know how hard it is and I don’t want to do that. That’s my real life experience with having that scare. I’m lucky that I went off the patch, everything was fine, I went back to normal, beautiful blood pressure. I share that just to say medications can raise blood pressure. A lot of things can raise blood pressure and it’s important to catch it early and to know and to intervene.
I know we talked about half the population is not salt sensitive or half the people with high blood pressure are not salt sensitive.
I mentioned the DASH diet, dietary approaches to stop hypertension. One of the big things that we’ve learned that I always say on this podcast is the best kept secret or worst kept secret is there’s a lot of things that impact blood pressure beyond sodium in the diet and that’s potassium. Angel, you talked about getting more fruits and vegetables, that’s always good for everybody, but a big piece of that is how much potassium are we getting into our diets? Because that’s good for our blood pressure and magnesium as well.
Angel, let’s talk more about what realistically people can do with diet, exercise, weight management. We know weight management is so difficult, but if you could share some really key takeaways for people, what are some tangible things they can do today to impact their diet in a positive way. Then we’ll also hear from Dr. Jay. How do we get more patients referred to dietitians?
[00:42:55] Angel: I’m a big believer in, like I mentioned earlier, meeting people where they’re at and we’d want to set smart goals in a way to get them to try to resonate. For example, what is the ultimate goal here? It might be a grandmother wants to see the granddaughter get married, so we got to try to tie something, so there’s a bit of a reward component to it.
[00:43:27] Melissa: Quality of life and personal– what their priorities are, what’s important to them.
[00:43:32] Angel: Exactly. What’s the priority. If we go there and we got to set smart goals and sometimes we become dietitians or anyone in any type of health related field we throw the gauntlet down and say do, you got all these things and you could do it. Of course we all struggle with all these different things that it’s eating behaviors, as I mentioned. If it took you 20 years to develop high blood pressure it’s not going to change overnight, so it’s like, can we pick a couple of things and start to focus on those? It might be, for example, oh, I only eat one serving of fruit per day.
If we’re talking five and they’re getting one, that five is going to be too big of a leap, so maybe we shoot for two or three. We make it a little more manageable, we modify it and then we can improve from there. Maybe we like to eat out a lot. If we’re going to deal with somebody who eats out all the time, maybe we review some menus and we say, “Hey, here’s some good options that we can choose, that might be better.”
If three o’clock, they have a crash every afternoon and they want to go get a vending machine, or maybe let’s bring some snacks with you.
Let’s start reading food labels. if you get a meal at the store, I can’t talk about brands here. [chuckles] We’re looking at one of these- [crosstalk]
[00:45:35] Melissa: A frozen meal,
[00:45:36] Angel: -frozen meals, yes. That meal might come in at 750 milligrams per serving. Can we try to find something 350, 300 or lower? It’s going to be hard, but there are options out there. Then you’re looking at what is reduced sodium or low sodium very low sodium or what is considered salt sodium free. You got to try to take it back. One of the struggles a lot of people is that if we take people and they’re used to very high salt, it’s hard to come back. My children sometimes, you make eggs or whatever and they just start salting without even tasting,
then if we’re going to make any changes, we got to try to make it measurable. We can’t just throw out there and be like, “Oh, we’re going to eat better.” That’s not really going to work. If for example, it’s going to be fruit consumption, let’s make it, I’m going to eat two servings of fruit per day, make it measurable.
If I’m going to be active, it can’t just be, I’m going to do 30 minutes of activity, because some people might count. When I lived in New York City I had to walk 10 minutes to the subway and then walk 10 minutes to work. That’s 20 minutes of activity. Some people may not count that as 20 minutes of activity, because it’s not in a gym. If we redefine things, make it measurable. We also have to make it attainable because if we aren’t making things attainable, we’re more likely to quit. We’re going to throw in the towel. For example the two servings of fruit per day is pretty easy.
, but then can we get some diversity in there? It can’t just be the same thing over and over. Maybe we try to say, today you’re going to do strawberries or banana. Maybe tomorrow you do orange and peaches.
We try to incorporate a little variety in there. Sometimes canned or frozen might get a bad rap. They’re actually picked fresh and it’s actually wonderful. We can look at the labels and see what the items preserved in. If we had a choice between sugar or water based, I’d go for the water based. It’s not going to be loaded with sugar, but you can read the can and see what’s on there. We got to do that.
[00:47:57] Melissa: A lot of label reading and just-
[00:47:58] Angel: Label reading.
[00:47:59] Melissa: -being realistic. I think people appreciate what to add versus what to subtract, and those small goals. Also, I don’t think we’ve mentioned yet, and I’d love to get your take on this, Dr. Jay is like, what about stress management? I mean that’s what I always talk to people about – stress can obviously raise your blood pressure, but does that really contribute to chronic high blood pressure-
[00:48:21] Jay: It can.
[00:48:22] Melissa: -or chronic stress I guess, if you’re–
[00:48:24] Jay: It’s one of those things that is intensely personal. Listening to how Angel thinks about working with his patient is that we just have to understand their own life. Everyone comes to us, different background, different culture, different lifestyle, different socioeconomic class. For some people I’ve noticed are intensely stressed but for different reasons and some are not really modifiable. Like somebody has a high stress job. What are you going to do? Tell them not to work? A single mother supporting two children and has two jobs.
I’m not sure that I’m going to be able to help that situation by telling them I have any advice to really give them other than, you’re doing a great job. Here are the things you can change in your life. Let’s talk about that. It’s a difficult thing just because everybody comes from a different background, different cultural, and you can’t really assume. That’s why the laundry list just doesn’t work, it just never has.
It’s not defined per individuals. It comes from an academic point of view where here’s what has worked in science, but the actual trick is how do you translate that to somebody’s real life, which is what we’re talking about. What works for them in their life, that they can actually continue. That’s the real trick. To answer your question, yes, stress is definitely a part of it for a lot of people, but how do you measure that? In what capacity does that person have to really modify that source of stress?
[00:49:56] Melissa: This is so exciting because I feel like the whole aspect of figuring out what works for you. That’s one of the reasons I love diabetes education is because people can try something and see how it impacts their blood sugar. Then they can make choices. This is really exciting. Dr. Jay, how can we get more people to see dietitians? How can we fix the healthcare system with regard to that?
[00:50:23] Jay: That’s a tough– It always seemed to me medicine in general still, for the large majority of organizations, is still highly siloed. Cardiology just stays in cardiology’s lanes, internal medicine stays in this lane. Some have broadened a bit especially for endocrinology internal medicine they’ve broadened to more team-based approach and taking in multidisciplinary approach to care. I think that’s the right way.
The only realistic way with the current structure of the medical systems is that within primary care goes broaden much beyond just the physician themselves, but mental health, behavioral health, dietitians, exercise, coaches, and physiologists. All should come together and that’s possible and it happens not as much as we would like, and there’s probably lots of opportunity for improvement there. That’s the general direction that I could see really some progress being made with the health systems as they currently are structured.
[00:51:29] Melissa: Thank you. I know it’s a tough question and I appreciate you being willing to talk about that. Following up along the same veins, I know that not many clinicians or providers are in the digital tech space, so any thoughts that you’d like to share on that and why more should get involved?
[00:51:47] Jay: The clinician’s voice is so important in any new company, new venture startup, product development, all of that. They’re software engineers, they’re product people, they’re business people, they’ve good ideas. Again, translating those ideas to reality in healthcare, in a clinical world that makes sense and has scientific backing behind it, that interface is our job. That’s our job. That’s what we do.
Even if people haven’t had experience outside of traditional medical practice, your voice is important. Your experience is highly valued and is really needed in every facet of translating an idea and a technology or some system into reality of healthcare. I would just encourage people who are interested to not feel that they don’t have the background for it or they don’t have the experience for it. You have much more experience than you give yourself credit for generally, clinicians do, providers do. Just remembering that, and I think it’s a super important part of digital health of any real healthcare business at all.
[00:53:01] Melissa: Thank you. Well then as we’re wrapping up, I would love for both of you to share how people can connect with you, find more information, stay up to date on this topic. Angel, let’s start with you. I know that you have a podcast called The Hot Sauce. Where else can people connect with you?
[00:53:20] Angel: They can connect with me on social media. You can go on Twitter at ACP Nutrition or you can find me on Facebook, Instagram @acplanells. To mention about finding a dietitian, you can always go to eatright.org, you can find a dietitian near you. For many of your listeners or people that are not aware, they could probably relate to their provider, “Hey, can I also see the dietitian?” There’s potentially an opportunity for a referral source. In that 10 to 15-minute session, there’s a lot of things being covered that’s probably an oversight and afterward, it’s like, “Oh I should have probably seen the dietitian.” Ask your provider or you can go to eatright.org, check them out that way.
[00:53:57] Melissa: Great point. Thank you. Dr. Shah, tell us the Aktiia website and also how people can find you on LinkedIn and so on.
[00:54:10] Jay: You can sign on for the email notification list. That way we’ll just push updates and new information out. All the social media, the handles are all the same @Aktiiaglobal and then on LinkedIn as well, Jay Shah, and you can find me there.
[00:54:26] Melissa: Wonderful. Thank you so much. I’ll have all those links of course in the show notes @soundbitesrd.com, along with some DASH diet information. I have a fairly old podcast on it, but the information is still current that I’ll share. My friend Roseanne Rust wrote the DASH Diet for Dummies book. Angel knows her, so a shout out to her. Thank you both so much for coming on the show and talking about hypertension and this exciting new technology. I look forward to staying tuned and seeing how it evolves and hopefully, becoming more accessible, especially in the United States. Thank you again so much.
[00:55:01] Jay: Thanks very much for having us. Appreciate your time.
[00:55:04] Angel: Thank you very much.
[00:55:05] Melissa: For everybody listening, as always, enjoy your food with health in mind. Till next time.
[music]
[00:55:11] Melissa:
Hey everybody – I wanted to share some additional information with you about salt and sodium and encourage you to tune into the next episode with Amy Myrdal Miller as we discuss this topic as well.
So here are my top 10 things you should know about salt and sodium.
Most of the sodium in our diets comes from food itself – either through processing (because salt is an effective preservative to prevent spoilage and of course adds flavor.- or it’s naturally occurring. So most of the sodium in our diets is not the added salt from our salt shaker.
Therefore, reading labels can help you identify lower vs. higher sodium foods. I’ll put a chart in my shownotes for this episode at soundbitesrd.com that details out label reading tips such as sodium claims like “no salt added” or “low sodium” or “very low sodium” and how much sodium those actually mean and also words to look for on labels that can indicate added salt such as brined, marinated and even baking soda. So check out the details on my shownotes.
One teaspoon of table salt is about 2400 mg of sodium – but again that added salt in home cooking, baking and from the salt shaker is typically not where we are getting most of our sodium.
The AHA and DGAs rec no more than 2300 mg of sodium – and a lot of times you’ll see the additional phrase of “that’s about equal to 1 teaspoon of table salt” – which I feel is misleading because if I heard that and thought to myself that I don’t use much added salt then I would think I don’t consume much sodium which is just not true.
according to FDA/CDC the average sodium intake for Americans is 3400 mg but I can’t help but think it’s much higher in some cases.
According to the CDC more than 40% of the sodium we eat each day comes from 10 types of foods. These top 10 sources of sodium (in order) are breads and rolls, pizza, sandwiches, cold cuts and cured meats, soups, burritos and tacos, savory snacks (chips, popcorn, pretzels, crackers), chicken, cheese and eggs/omelets. I’m honestly not sure why chicken is on this list. Fresh chicken is not high in sodium. They didn’t specify if it was fried or processed chicken.
While canned beans are not on this top 10 list I often hear people don’t choose canned beans because of the sodium content but then they don’t choose dried beans because they’re not convenient since you have to soak them before preparation. The great thing is that rinsing canned beans (or other canned vegetables) can reduce the sodium content by up to 40% so I really encourage people to do that so they are getting more beans and veggies in their diet!
It’s not just about sodium (the mineral sodium) – it’s about other minerals that are good for blood pressure that we often don’t get enough of like potassium, magnesium and calcium – that’s where the DASH diet comes in (Dietary approaches to stop hypertension) which promotes fruits, vegs, whole grains, lean proteins, nuts, seeds, legumes and lowfat dairy (because these foods provide potassium, magnesium and calcium) as well as LESS overly processed and low in nutrient foods, sugars, high fat foods, high sodium foods, and alcohol. I have a podcast episode with my colleague and friend Rosanne Rust who authored the DASH Diet for Dummies book so I’ll link to that in these shownotes as well.
Using herbs and spices in cooking in place of some or all of the salt is a great way to add flavor without increasing the amount of sodium. But if you’re like me – you may not be quite sure how to do this. My colleague and friend Jill Weisenberger has a great spice guide that I will be including in my Do MORE with Dinner Resource Kit that is still being updated so keep an eye out for that – hopefully in the next month or so.
MSG or monosodium glutamate is a great way to enhance flavor and reduce sodium in your cooking. Amy and I discuss this in the next episode but I also have a 3 part series on MSG that I’ll link to in the shownotes. These three episodes are absolutely some of my favorite episodes out of the nearly 250 that I’ve done since the podcast launched 8 years ago. And – fun fact – NPR’s This American Life podcast released an MSG related episode the SAME WEEK I released this series and it is very interesting and entertaining. I highly recommend listening to it and will link to it in my shownotes, too.
Ok that’s my top 10 things you should know about salt and sodium.
Thanks again for listening and stay tuned to the next episode with Amy Myrdal Miller for more information!
For more information, visit sound bites rd.com. This podcast does not provide medical advice – it is for informational purposes only. Please see a registered dietitian for individualized advice. Music by Dave Birk. Produced by JAG in Detroit podcasts. Copyright Sound Bites Inc. All Rights Reserved.
[music]
anscript here…
LISTEN, LEARN AND EARN
Listen to select Sound Bites Podcasts and earn free CEU credits approved by the Commission on Dietetic Registration (CDR) for registered dietitian nutritionists and dietetic technicians, registered. Get started!
Get Melissa’s Sound Science Toolkit here!
Partnerships:
Sound Bites is partnering with the Association of Diabetes Care and Education Specialists (formerly the American Association of Diabetes Educators)! Stay tuned for updates on the podcast, blog and newsletter!
Sound Bites is partnering with the International Food Information Council! Stay tuned for updates on the podcast, blog and newsletter!
Lynn Munson. MS, RD, LDon September 9, 2023 at 12:47 pm
Hi Melissa,
I’ve enjoyed your podcasts for years and this was another good one! I just wanted to respond to your puzzlement about why chicken is considered one of the main sodium sources in our diet, As a long-time renal RD, I can explain: it’s because so much chicken is injected with sodium phosphate. (We worry about the sodium AND the phosphate additives in renal patients’ diets.) Almost all the chicken that people eat in restaurants (especially chain restaurants) is injected, and plenty of the chicken in grocery stores is as well (primarily chicken breast, because it can be dry, and the sodium phosphate holds water in the meat). Natural chicken (uninjected) has no more than 50-70 mg sodium/serving and injected meats will have as much as 250 mg/serving.
Lynn,
Thank you so much for listening to the podcast and for sharing this helpful information! I appreciate you clearing up my confusion on this and also appreciate the work you do as a renal dietitian!
Melissa
Sign up for my monthly newsletter and episode eblasts so you never miss an update!
Listen on Stitcher (Android)
Install the Stitcher App
1. Search for “sound bites with melissa joy dobbins” 2. Choose Play Current Episode or Add to Playlist
Choose “Play Episode”
Subscribe & Review on iPhone
Open the “Podcast” app on your iPhone
Search for “Sound bites with melissa joy dobbins”
Open the podcast and click “Subscribe” and your done!
Write a Review
Click “Reviews”, then “Write a Review”.
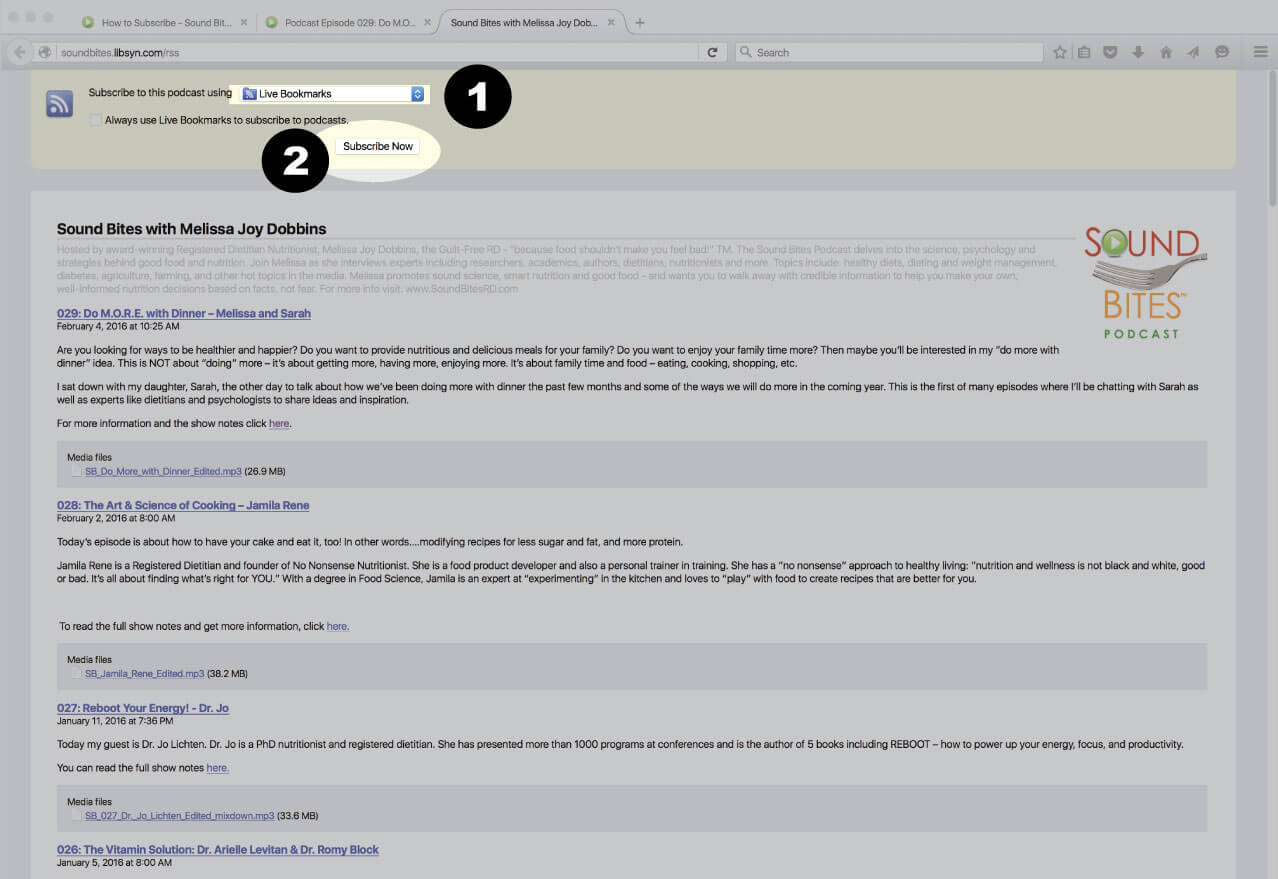
Subscribe via RSS Feed
Navigate to any podcast player . Click on the RSS feed icon.
Click on the RSS feed icon.
Click on RSS Feed
Choose which application you would like to use to receive the RSS feed
Click “Subscribe Now”
Confirm settings and subscribe.
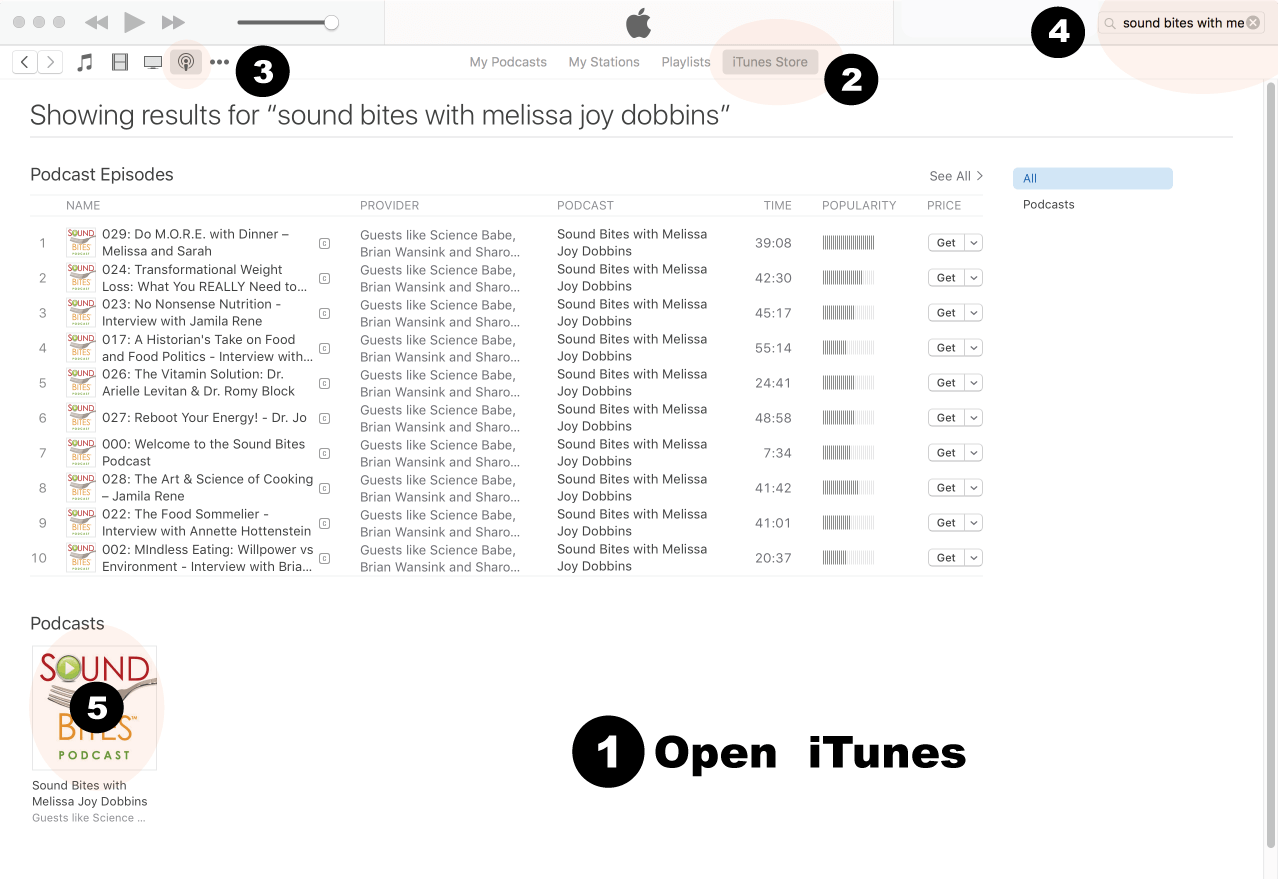
How to Review in iTunes
Open iTunes desktop application
Click iTunes Store
Click on Podcasts
Search for “Sound bites with Melissa Joy Dobbins”
Click on podcast image
Search for Sound Bites podcast in iTunes
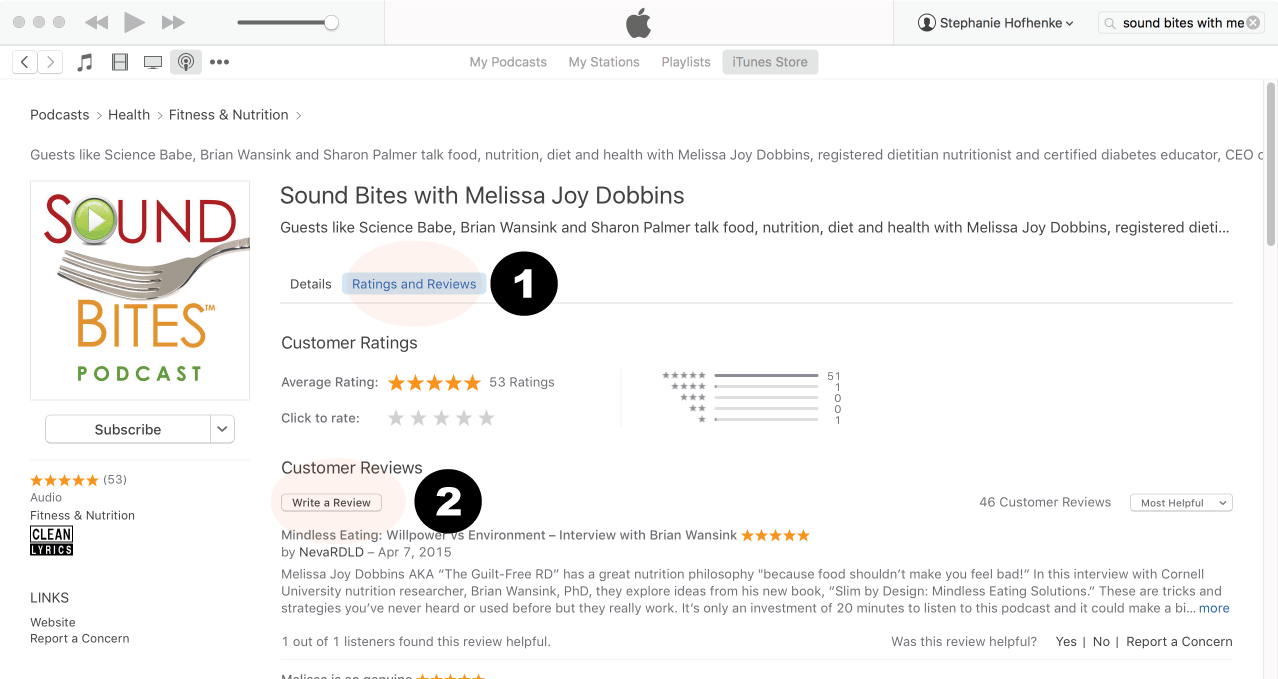
Click Ratings & Reivews
Click Write a Review
View reviews and write your own review.
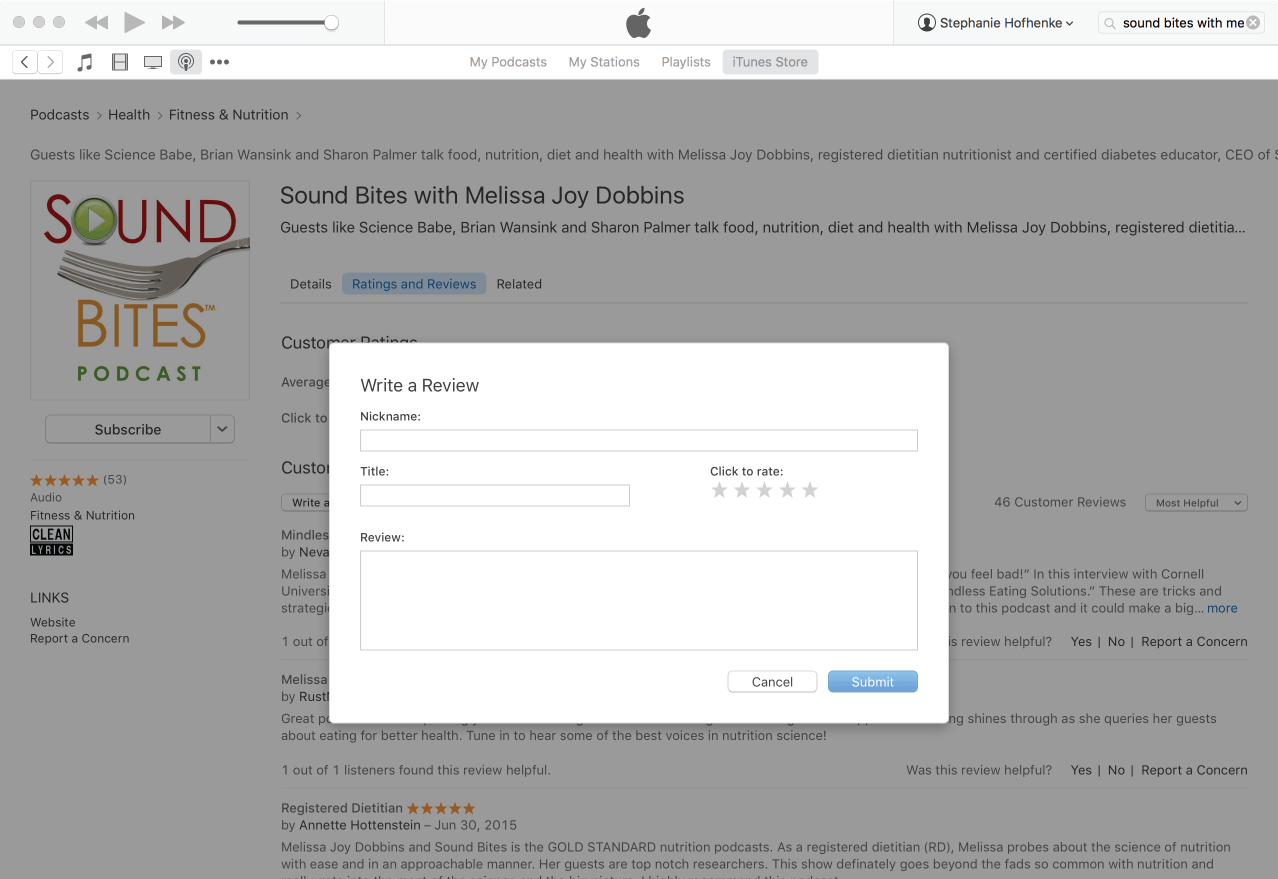
Write your review…. Thank you!
Write your review!
How to subscribe via iTunes
Click here to view the Sound Bites Podcastin iTunes, then click the blue “View in iTunes” button. This will open your iTunes application directly to Sound Bites Podcast. Click the “Subscribe” button, and your done!














Hi Melissa,
I’ve enjoyed your podcasts for years and this was another good one! I just wanted to respond to your puzzlement about why chicken is considered one of the main sodium sources in our diet, As a long-time renal RD, I can explain: it’s because so much chicken is injected with sodium phosphate. (We worry about the sodium AND the phosphate additives in renal patients’ diets.) Almost all the chicken that people eat in restaurants (especially chain restaurants) is injected, and plenty of the chicken in grocery stores is as well (primarily chicken breast, because it can be dry, and the sodium phosphate holds water in the meat). Natural chicken (uninjected) has no more than 50-70 mg sodium/serving and injected meats will have as much as 250 mg/serving.
Lynn,
Thank you so much for listening to the podcast and for sharing this helpful information! I appreciate you clearing up my confusion on this and also appreciate the work you do as a renal dietitian!
Melissa