Celebrating over 1 Million Downloads and 50,000 Free CEUs on the Sound Bites® Podcast | NEW: Get 1 years’ worth of CEUs with the new 15-CEU Podcast Course
Reading and Translating Research: Skills That Can Be Up-Leveled
More and more, people are inundated with information and surrounded by often-conflicting information, especially when it comes to nutrition in the news. Nutrition research is moving at a rapid pace yet the scientific method of testing and verifying results is important. Translating research findings requires understanding food science, food composition, and the ability to individualize strategies and approach to behavior change.
Dietitians have the necessary background and can grow their skills – without burning through all their time and mental energy. And like learning to cook or speak a foreign language, the fastest way to build skills and confidence is to jump in and practice – ideally with some support.
When we take nutrition from daunting to doable, we transform people’s lives.” – Karen Collins
Tune into this episode to learn about:
Getting beyond the headlines
Determining the source or type of article
Checking into who/what is being studied and what is being asked/tested
Different aspects of a research study that are important to consider
If the results are statistically significant and/or clinically meaningful
Accessing research papers
Factors related to measurement including dose-response
Meta-analyses and challenges they may pose
Some common challenges in understanding, interpreting and translating nutrition research today
Practical tips and takeaways for both the public and health professionals
Karen’s research reviews, resources (cheat sheets and client tip sheets), dietitian-only membership program
Karen Collins, MS, RDN, CDN, FAND
Karen is a registered dietitian nutritionist whose tagline – “Taking Nutrition from Daunting to Doable” – highlights her focus on helping people cut through the confusion of nutrition headlines and put complex information in perspective within the “big picture” of overall research. Karen is a consultant, speaker and writer who focuses on translating current nutrition science related to cardiovascular health, cancer prevention and survivorship, and their intersection in cardio-oncology.
Among her most visible consultant roles, Karen has served as Nutrition Advisor to the American Institute for Cancer Research (AICR) for almost all of its 40 years. Karen has authored and co-authored multiple peer-reviewed book chapters and research summaries for health professionals and she’s written over 2,000 nutrition-related articles for the public. In 2019, Karen received AICR’s first Distinguished Service Award, noting her expertise in translating nutrition research into empowering, evidence-based messages. She is a Fellow of the Academy of Nutrition and Dietetics, and just announced, Karen will be a 2024 recipient of the Academy’s prestigious Medallion Award.
Karen’s website – KarenCollinsNutrition.com – features her reviews that put cancer and cardiovascular nutrition research in perspective. And, in yet another way of helping dietitians focused on accurately translating research, Karen has created a dietitians-only membership program, the Daunting to Doable Nutrition Pro Circle.
Dietitians have the necessary background and can up-level their skills at reading and interpreting research. You don’t need to tackle this alone, because you have resources and support.” – Karen Collins
Resources
Some links may be affiliate links. As an Amazon Associate, I earn from qualifying purchases.
Karen Collins: Nutrition website, to access reviews with analysis and application of important nutrition research topics
Welcome to Sound Bites, hosted by registered dietitian nutritionist Melissa Joy Dobbins. Let’s delve into the science, the psychology, and the strategies behind good food and nutrition.
Melissa (00:22):
Hello and welcome to the Sound Bites Podcast. Today’s episode is about why it’s so important to better understand nutrition research and build confidence reviewing studies, and also why research translation is so challenging.
Much of our conversation today will be geared towards registered dietitian nutritionists and other healthcare professionals, but really anyone who’s listening can gain a better understanding of and appreciation for nutrition research.
My guest today is registered dietitian nutritionist Karen Collins. She’s a consultant, writer and speaker who focuses on translating nutrition research related to heart health, cancer and their intersection.
Karen is a nutrition advisor to the American Institute for Cancer Research and authors research summaries for health professionals, as well as nutrition related articles for the public.
Karen also writes research reviews that run on her website, which is karencollinsnutrition.com. And I am so excited that I just learned recently that she is receiving a medallion award from the Academy of Nutrition and Dietetics. Welcome to the show, Karen.
Karen Collins (01:40):
Thank you. I’m delighted to be here.
Melissa (01:43):
I am looking forward to this. I’ve been wanting to have you on the podcast for a long time. This is your first time on the show, but we’ve known each other for years, and I just love the work that you do. I want everybody to know that this episode is not sponsored, and I would love for you to share more about your background, the work you do, and of course, this exciting award.
Karen Collins (02:05):
Well, thank you. Yeah. The medallion award is truly the honor of a lifetime for me. It is an award given by the Academy of Nutrition and Dietetics to recognize high standards of the profession through accomplishments, leadership and service to the profession and to others.
And interestingly, the process of my nomination for this medallion award has actually prompted me to do a lot of retrospective thinking about my career. And I realized that my tagline, which is taking nutrition from daunting to doable, which I developed intending to convey how I help others become less daunted by nutrition, could really apply to how I see nutrition research translation, how it’s been for my career.
I got my bachelor’s in dietetics at Purdue University where I did honors research in dietary fiber, which is a full circle bit to the work I do now. I completed a dietetic internship at Barnes Hospital in St. Louis.
Then after a few years as a hospital clinical dietitian, I left for Cornell University where I earned my master’s in human nutrition. And there my experiences as a teaching assistant and research assistant now seem like more pieces in this jigsaw puzzle that was being built.
And as I thought back to it, one of our graduate seminars involved analyzing a research study, breaking up individually each week and presenting it to the seminar. And the funny thing is, when you think about it, in contrast to our career, our work as dietitians, we’d take weeks digging into one single study that we had to present.
And still the professor would usually manage to find multiple things that we’d overlooked and end up leaving us feeling pretty humble. And we all basically dreaded that seminar.
But it turns out that it was a truly formative part of my professional development. My early career included both in and outpatient hospital care. And then I had a private practice in nutrition counseling for many years.
Like all dietitians, I always aimed to provide information and strategies that were based on the best available scientific evidence.
But I think the first time I really thought of my work as translating nutrition science was when I began working as nutrition advisor to the American Institute for Cancer Research, which is 40 years ago now.
Communicating about the strength of evidence behind recommendations and translating them into practical nutrition and lifestyle strategies was always a key part of my role with AICR. And over time I realized that this need to identify and accurately translate sound research exists regardless of the area of nutrition that we practice in. I see it in my work in cardiovascular health, and it’s true for all of us.
So, initially this was really daunting to me, that digging into research and needing to talk about it in a more in-depth way. But I kept working at polishing my skills and gradually following the research became less overwhelming and actually quite stimulating.
And now I love writing in professional forums, breaking down complexities of the research and translating it into concrete action steps.
And then it comes full circle when I heard from colleagues that many of them find reviewing and translating research as daunting as I once did. So, I believe so much in the power of nutrition to transform lives that a few years ago I made a pivot in my career.
And now the majority of my work focuses on helping my dietitian colleagues accurately and confidently translate nutrition science.
Melissa (05:50):
When I saw that you were doing that, I’m like, “Genius, oh my gosh.” We need so much help in this area. And the public needs to have information that they can grasp and apply to their daily lives. And there’s so much involved in this process, and again, when I saw that you were helping other dietitians, I’m like, “Oh my gosh, this is wonderful. I just had to talk with you about this.”
Karen Collins (06:16):
Aw, thanks.
Melissa (06:17):
Clearly you are very passionate and committed to helping dietitians build those skills. And as we’ve talked, build that confidence.
And it’s interesting because when I work with dietitians on communication skills in general, a big, huge part of that is building the confidence and what each individual practitioner might need to do might be different, and oftentimes is different.
Some people find that they need more practice. Other people find that they need to dig more into a specific topic so that they have a deeper understanding of it, and that builds the confidence.
So, I think we kind of have a parallel here with how we help dietitians and boosting that confidence is so important because once you have more confidence, you are more likely to get out there and do the communications and it’s so needed.
Karen Collins (07:09):
And speak as clearly as the people who don’t know what they’re talking about do. Because that’s one of the frustrating things is we are a science-based profession, so we do frame things as it looks as though emerging evidence suggests versus the strong evidence of this.
But the people who have no scientific background are just right out there making these very strong statements. And just because of the way they say it, I think it can make some people trust what they’re saying more than when we’re trying to be cautious and accurate.
So, we still want to be accurate. But we need to be able to have some confidence in our translation that it’s science-based.
Melissa (07:56):
Absolutely. And I talk about that all the time when I help other dietitians with their communications, is we have to be accurate and science-based, but we have to be compelling because these people who are saying they can easily be compelling because they can say whatever they want.
And so, there’s a huge challenge there for sure. And when we don’t have that confidence or that deeper skillset, I think we do kind of hedge our bets or we’re afraid to be more specific. Things can get lost in translation or oversimplified. And it does require that deeper conversation.
Karen Collins (08:39):
And I think we owe it to people when there is doubt, when there’s two sides to something, when there are questions that have not been resolved yet, that shouldn’t come across as lack of confidence or hesitancy.
We owe it to people to say, “Here’s what the recommendations are, or here’s where the questions are, here’s where the steps evidence is strong, here’s what we still need to know or how it might apply to different people.”
The problem is translating that to people who don’t have scientific knowledge, but everyone can understand that there’s uncertainties.
Melissa (09:14):
Right. I think that’s so important because, we think, and maybe it’s true that the people just want a black and white answer. They just want a bottom line. And that’s just not the nature of science and nutrition.
So, communicating those uncertainties in a way that explains this is normal. This is where the science is to date. Like you said, these are the questions this research has showed us, now we need to look into this.
And I did an episode with Dr. David Allison where he articulated quite a bit of that, that we need to be more truthful in our communications, which isn’t that we’re trying to maybe necessarily tie everything up in a pretty bow.
But if we start having more of those conversations about the uncertainties, then people will be more comfortable with that. It’s challenging and it’s maybe a little frustrating, but they’ll understand more that that’s just the nature of nutrition and science.
So, let’s talk more about all of the information and misinformation and disinformation out there. You may be articulating more about the nature of the rapid pace that we were seeing all of this stuff and also wanted to mention when we brought up the topic of accuracy, and yes, we have to be evidence-based and sound science and accurate.
And sometimes what I talk about in communications is we maybe don’t want to get so tied up with being accurate that we lose sight of maybe what’s meaningful. So, we can be accurate, but kind of frame it up in a way that is maybe more meaningful or helpful. And I think addressing some of those uncertainties can be a part of that.
Karen Collins (10:55):
Yeah. I mean, I think people are so inundated with information now that it’s very different from when you and I first began our work as dietitians. It’s a different world.
And for one thing, because of the internet information that’s outdated doesn’t just fade away anymore. It somehow keeps circulating around even when it’s been debunked by authoritative reviews of the evidence. So, it’s very confusing to people.
And I also see as part of the things that is providing some of the challenge for us is that there’s now really a blurring of the lines between education and entertainment.
An example of this dietitians I talked to, we’re getting a lot of questions from people about the Netflix docuseries getting huge views called You Are What You Eat: A Twin Experiment, which features insights from the Stanford Twin Study, which is a randomized control trial published in one of the JAMA peer reviewed journals comparing healthy vegan versus healthy omnivore diets.
I found both the series and the study very interesting, but the problem is dietitians were being asked about this docuseries. Of course, people hadn’t read the study, and the docuseries doesn’t mention that it actually diverges from the study in several key aspects and throws in some information that wasn’t at all part of the study.
So, it really became quite confusing. And honestly, it took quite a bit of time to review the whole series and redig into the study and all the supplemental data. So, I created a summary for subscribers to my email updates and then AICR, the American Institute for Cancer Research, asked me to write a brief about it for its blog.
Because these are the things that’s very challenging as a dietitian or a health professional to keep up with all of this stuff.
Melissa (12:51):
Yes. I love that because you have shown that you are a trusted resource, and if somebody is so inclined that now they can build their skills too.
But certainly not every dietitian can take the deep dive that you did on this docuseries. And don’t even get me started on all of these shock-umentaries out there. But yeah, it is very daunting. How are we supposed to stay up to date on all of these areas of nutrition?
And that’s one of the things that I tell people. You don’t have to know everything. You’re not possibly going to be able to know everything, but if you have an interest in cancer or diabetes or weight, take as deep of a dive as you’re interested in and know that there’s other people who are interested in other areas.
And then we can, as a collective, we can say, “Hey, if I get questions about cancer, I’m pointing them towards your blog and your resources. It’s not an area of expertise for me.” And I always say this, I’ve been a certified diabetes educator for 25 years, but there’s still a lot of things about diabetes that I’m not an expert in.
So, I think it makes sense when we say that, but I think it’s important for dietitians to hear that and to remind themselves, “I don’t have to know everything, but let me dive in where I am interested and take it as far as I can.”
Karen Collins (14:12):
And I think as dietitians part of how we respond to these questions from people, they’ll ask about a particular headline or a particular documentary or something like that. But when these things focus on individual studies, that’s what’s assaulting people all the time now.
It’s this new study and this new study and this new study, but that’s not the basis for advice or action. So, we really have to help them. I mean, people will say, “I see science just flip flops back and forth.”
No, it doesn’t flip flop back and forth because we don’t change recommendations on a dime based on one new study. We make advice and choices based on the body of research. It’s only the headlines that flip flop.
And part of the reason they flip flop, because that’s when you click on them more is when it’s something new and surprising. If it said, “Guess what? The advice that you heard yesterday is still true today,” who would click on it?
So, we really need to separate that science doesn’t flip flop. The headlines flip flop, and that’s why they’re so misleading. And that’s the kind of thing that I believe as dietitians, we need to sort of, giving the person a fish, but also teaching them how to fish.
We need to give people the answer they need, but also help them to understand why what we’re providing is worth listening to or acting on and what headlines they might have seen, which is really premature or out of alignment with what the overall body of research shows.
Melissa (15:45):
Yes. I know we’re going to dive into some specifics, but that concept of even just explaining to people that one study or one headline doesn’t change everything that’s come before it, even if they don’t know what the body of evidence shows or have access to read the study, just that concept that one study doesn’t change everything.
So, that’s like one of those really basic simple things that I have on my short list to share with dietitians and the public is like, okay, it helps us get perspective. And those headlines I long have kind of blamed the media for kind of stirring the pot on all of this.
But the more I found out about research and confirmation bias and research design it was illuminated to me that, oh, there’s a lot of different places where there can be misinterpretation or exaggeration.
And so, I had to realize, “Okay, I have to stop just blaming the media. It’s really more complex than that.” And that’s a lot of the work that you do.
Karen Collins (16:50):
Absolutely. It’s a lot of many pieces of this puzzle. Yeah.
Melissa (16:53):
Yes. Where can we look, and we’re going to talk about some of those, but before we jump into that, and we’re going to talk a little bit more at the end, of course, pointing people to where they can connect with you and find out more about what you offer.
But I think it makes a lot of sense now for you just kind of give an overview of what tools, resources, you have a membership, just kind of top line that, so that people can keep that in mind as we continue our conversation.
Karen Collins (17:16):
Sure. So, I kind of think of my efforts as a three-legged stool, each providing a different sort of support to dietitians, to health professionals and to everyone. First would be the in-depth research reviews that are published on my website.
So, for example, with all the attention to ultra-processed foods, there are really important nuances in the research that it’s not quite as simple as some of the blanket statements make it seem. So, I took a deep dive into the literature and summarized key take home points.
Hypertension is the number one modifiable risk factor heart disease, and yet only about one in four people with hypertension have it under control. And it can be a side effect of some types of cancer treatment, which when it occurs during a treatment, can cause delays or reduce doses of treatment.
So, it’s very important factor. So, I have several research reviews on different aspects of a diet to support a healthy blood pressure and factors to consider when it seems as though, “diet doesn’t work.”
With the popularity of supplements, many people are unaware that some supplements, even certain natural botanical products, can interfere with adjuvant hormone therapy for breast cancer. So, I have a video interview with our colleague, oncology research dietitian Maura Harrigan, sharing results of her research on this important topic. So, there’s the research reviews on my website.
Second, I created free resources, both dietitian cheat sheets and printable client-ready tip sheets. For example, research now shows that dietary fiber is not as simple as just soluble or insoluble. So, I created a toolkit for dietitians with a cheat sheet as well as a pantry checklist they can use with patients and clients to help people bolster a truly well-rounded intake of fiber.
Dietitians were telling me they found it challenging to communicate about the benefits of nitrate rich foods for healthy blood vessels amidst concerns over nitrates and processed meats, increasing risk of colorectal cancer. So, I created dietitian cheat sheet on that and on a whole range of topics.
And then I have client-ready tip sheets, for example, on an anti-inflammatory diet, a Mediterranean style diet on increasing magnesium consumption, all to help dietitians actively involve clients in identifying the choices that will work in their lives.
So, the research reviews the resources. And then third, the newest leg of the stool here is a few years ago I created a dietitians-only membership program, the Daunting to Doable Nutrition Pro Circle, which here again, actually has three elements. We focus on building understanding of current research.
So, we dive into topics that members want to know more about or are asked about and really want to understand the research. But as we do this with a goal of along those lines, we mentioned before of not only giving the fish, but teaching how to fish, really building skills in research translation.
And by going through this repeatedly on different topics, it’s like building muscle memory that can then be applied to other research. So, it might be understanding the difference between a hazard and a risk when there’s things in the headlines.
So, we’re understanding the research, then we talk about communicating the science accurately and confidently. For example, one of the cardiac rehab dietitians in the membership had a patient completely disavow oatmeal and any oat cereal when headlines came out about the pesticide chlormequat.
So, we worked on talking points about how to communicate that removing this very valuable source of viscous fiber would not be an accurate translation of the science.
And then third, we talk about how the same strategy or same message, same goal, would be applied differently to different people that we work with. So, we address very practical questions that come up, for example, about processed meats where people ask, well, what about the bacon that says no nitrate added?
Or what about other deli meat? Is that a processed meat? Or someone’s going to use a fiber supplement for LDL cholesterol lowering, are they all the same? Well, no, they’re not. And you have to choose the fiber supplement that’s appropriate for that use.
So, those very practical things that we cover, in other words, from understanding the research to really putting it into practice with individual clients.
Melissa (21:47):
I have to say, I was on your site recently and I saw the hypertension piece. And just as an example for our listeners, if we know that not everybody is salt sensitive, there’s no way to find out really, I mean, in a practical sense.
So, should we just not worry about salt? And you really get into the nuances of how do we still approach this in a healthful, practical way? So, I found that really interesting and all of the topics that you mentioned, I’m like, “Oh gosh, yeah, there’s so much there with fiber, ultra processed foods, supplements, nitrates, nitrates.”
I mean, yeah, these are some really big hot topics. So, thank you for sharing all of that and the work that you do. And I look forward as we continue this conversation to call out some more takeaways for our listeners.
And you mentioned the hazard versus risk. I mean, that’s something that I always have to go back to and remind myself, okay, what’s the difference here? And I know with cancer research, as with other research, but cancer in particular, that can be a complete game changer in how you’re understanding what the research is saying. It can be very confusing.
Karen Collins (22:51):
Absolutely.
Melissa (22:52):
Great. So, I know it seems like every day we already talked about these headlines that catch our attention. And I feel like whether they’re compelling or sensational or somewhere in between, I feel like the headline is just that tip of the iceberg. There’s so much more beneath that.
So, let’s walk through, where do we begin? What should we be looking for when we see these headlines? How do we take it to the next level?
Karen Collins (23:18):
Well, first of all, although it’s very hard to do don’t go by the headline. That is what draws our attention. That might even be all you see.
But we need to recognize that they’re often the most hyped. They often are not even written by the person who wrote the article. They’re written by someone else who doesn’t necessarily know the topic at all. And so, they may not be an accurate summary of the results and certainly not of the takeaway points at all.
Melissa (23:44):
So, just acknowledging this headline is just to get your attention.
Karen Collins (23:48):
Yes. Then the very next things I would do is to check, first of all, what is this coming from? Is it a conference summary, which would be presenting research that was not peer reviewed yet? And conference research is very valuable.
I love going to research conferences, but the purpose of those presentations is to collaborate with other researchers to identify, someone else will say, did you look at this? Did you analyze for this?
So, it helps them to polish up or look at their research before they submitted for publication. It’s not a takeaway message. Or is what you’re seeing from a peer reviewed journal or is what you’re seeing a blog or article post from someone with a personal point of view, maybe even with a goal of selling something.
Those are three really different categories. Then the next thing, once you just at least have that and that should influence how you view everything that follows is by where it falls in those three categories is to then check the basics, who or what is studied. Is this a human study? Is it a study of lab animals? Is it a cell culture?
For example, some of the headlines about a supposedly anti-inflammatory food may add a compound that’s found in whatever food it is to isolated cell cultures in a lab. But that doesn’t tell you anything in reality as you eat and digest that food, the compound would be broken down to other compounds and the original compound would never reach most of your body cells.
So, the study doesn’t reflect what eating that food would do and certainly doesn’t necessarily reflect the concentration that you’d be exposed to from eating that food in your diet.
Then I would look at what the study question is, and this is really important. Researchers need to identify one specific outcome as the primary result of a study. And the design of the study is based on that. Multiple testing where they report on a whole raft of outcomes can lead to identifying an association that’s merely found by chance. In common terms, we might call it phishing.
So, a study can report multiple outcomes, but it needs to be really clear which is the primary outcome that should be considered and is really most strongly supported by the data, and then be really clear on what is actually being compared or tested to answer that question.
So, for example, with all the interest in intermittent fasting, it’s important to clarify whether a study kept calorie consumption equal between a fasting and a non-fasting group, or if the fasting group tended to decrease calorie consumption, if that was allowed to happen and not statistically adjusted for.
So, in other words, would the results be really due to intermittent fasting, or would it be due actually to the calorie reduction that occurred and could then be replicated in any other way of reducing calories.
Or in a study of ultra-processed foods and associations with health. When we look at ultra-processed food as it occurs in a whole population as a population, a diet high in ultra-processed foods, we know is from the analysis of those people’s diets, it’s tied to high consumption of sugar sweetened beverages, sweet bakery and fast food. Those are the major contributors.
So, in a study like that, if there are findings related to health, you can’t try to use logic to say, so unsweetened soy milk or veggie burgers must be dangerous, because that’s not what those people were eating.
So, you really have to look very carefully at exactly what is being tested and how they’re defining it, what the confounding factors are that they’re adjusting for.
Melissa (27:42):
Yeah. A few things I want to follow up on and with the ultra-processed food. I recently did an episode with Joanne Slavin about ultra processed foods and the lack of the definition. So, to your point, how are they defining it in that particular study?
A different study might define it differently. So, then you’re comparing apples and oranges or soy milk and soy burgers. Clearly, I think we can all agree that unflavored soy milk is not the same as sugar sweetened beverages.
So, I would love for you to address briefly, you talked about human studies, animal studies, cell cultures. There’s a reason for these different types of we can’t have every research be humans.
And so, I would love for you to address that because I mean, at a basic level what I think like, oh, well animal studies don’t matter at all. Cell culture studies don’t matter. Mean they, they have a purpose. So, if you could address that.
Karen Collins (28:38):
Absolutely. And understanding that allows you to say, so what does that kind of study tell me? So, for example, to really understand metabolic pathways, some of those we can’t measure in a human, some, now they’ve got markers that can do that, but some can’t.
And first of all, human studies are very expensive, and you have to be able to document safety and concerns and all of that. So, you don’t just pop in with a human study without having backup data from laboratory studies that would never get approval, never get funding, never get approved.
So, the cell studies give us very valuable information about mechanisms and things like that. Then it’s like a building, like a staircase building a house at various levels. When you have some things that are turned up that are important in those cell studies, then you can look at lab and animal studies.
And again, there are things that we can look at in animals that we can’t look at in humans. And so, that provides another level of information in a living being in a whole body, not just an isolated cell. And there are controls we can tightly control what food an animal’s given no matter how hard we try, it is very hard in a human study to actually control every morsel they eat.
Melissa (30:05):
And other things.
Karen Collins (30:06):
Yeah. And other things. Absolutely. So, there’s much more control that allows us to define things in an animal study that we can’t get in a human study.
And then human studies are not all the same either. We have cross-sectional studies, which give you some general information about tendencies in a population associations, they don’t prove causation. They just show things that are typical or common or associated.
This is one of the challenges, and we can circle back to this later if you want, but what’s considered the strongest evidence in a human study is from a randomized control trial where we control all the other variables and people are randomly assigned by chance to these two different groups and so forth. That makes the evidence very strong.
But for many of the health concerns we have today, they develop over many years, over decades when we’re talking about cardiovascular disease, or cancer, dementia, many of our biggest health concerns.
And you really can’t do a randomized control trial that tightly controls what people eat and how much physical activity they have and all the other aspects of lifestyle for 30 years.
So, a good quality prospective cohort study, it’s observational, but if it’s done in a thoughtful manner with appropriate adjustments and controls and methodology and analyzed appropriately can also give us very strong evidence.
But so that’s why no single type of study, the randomized control trial, will generally be smaller. You might get more blood work and things like that than in a population observational study of thousands of people.
So, each of these, it’s like we’re putting a jigsaw puzzle together and each kind of study adds an important piece of that puzzle. And it’s only when we put all the pieces together that we have the best available answer for people.
Melissa (32:08):
Thank you. And you address the association or correlation versus causation, I was also going to address that as well. And that’s also when I say my short list, one study doesn’t change, everything is explaining to people just the difference between the correlation and causation.
And correct me if I’m wrong, because I say this all the time, but I would say the majority of nutrition research is observational just by the nature of nutrition research. Just because it is so difficult to do randomized control trials.
I mean, maybe that’s not how you would say it, but I feel like a lot of the data that we have is correlational. I suppose it depends.
Karen Collins (32:47):
Well, when we look at whole diet, I would agree with you. The thing is that often when we look at the laboratory research, it’s not looking at a raspberry or tea or fish or whatever. It’s looking at components, of the nutrients, of Omega-3 or calcium or vitamin D or protein or fiber or all these different things.
So yeah, I think when you’re looking at food based or diet-based research, a lot of our evidence comes from observational studies that then when we see something and the evidence is consistent, then there’s a basis to do an intervention trial, which would be a randomized controlled clinical trial where we can test.
So, it looks like in this population we consistently see eating more of this produces this result or eating less of this produces this result. How about if we do an intervention and have people eat more or eat less or do this or do that, will it change the outcome?
And that’s a different question. That’s the causation you’re talking about as opposed to, did it turn out that the people who ate this way actually had a whole lifestyle of healthier habits?
They also were different in physical activity or income or education or community support relationships, the environment in which they lived. Was it an environment that made it easy to have healthy habits or not so healthy? I mean, so many factors.
Melissa (34:10):
So many factors, yes. Thank you. Okay. So, once we get past some of those basics that you walked us through, checking some of these basics, what’s the next step to actually dig into the research study?
I’d love for you to comment on even getting access to the study, like open access versus if it’s not available, if it’s behind a paywall or, and this is another layer is just research that doesn’t even get published probably beyond the scope of our conversation, but what are those next steps to get that study and dig in?
Karen Collins (34:45):
Well, as far as getting the paper I think, the first place I always start is PubMed because it will often show if it’s published in a research journal that would have a paywall, there might be another access that is a government website that would be free of charge.
If I don’t see it there, then I’ll go to Google Scholar, which tends to turn up other places that a research paper might have been published or shared, for example, on a researcher’s website or something like that.
Every now and then, if I can’t get it through Google Scholar, I might check my preferred web browser with a topic, the study name, the author’s name, and every now and then it turns up. Depending if you’re in any dietetic practice group, some DPGs may offer access to a, a research database on certain topics.
If you really want the study and you can’t get any of those places, you can email the corresponding author. If you’re not familiar with doing this, you don’t just randomly pick an author or pick the first one listed.
In the author listing, they’ll indicate sometimes with a little envelope or with an asterisk or whatever who is the corresponding author. And you can email them and ask if they would be willing to share a copy of the study with you. Oftentimes they are.
And if you still can’t get it, then I think it’s really time to decide, is having that single study really going to change your advice or choices given that it’s really the overall body of research that’s most important.
You might decide it’s not worth it. And if it really is, then I would consider paying. Sometimes they’re very expensive and as soon as you see the price, it’s like, “Well, it’s not that important to me.”
But other times it’s not that expensive and it’s supporting good research. And then, however you get the study. I think as you were asking about next steps, Melissa, as far as we went through kind of what are the basic things that you would check through then to really dig in, I would look more at the results and differentiate just as we differentiate association versus causation.
Is it statistically significant or not? Because it would often be stated as a trend or something, but if it’s not statistically significant, it is possible that the results occurred by chance. And so, they could be an indicator, but you shouldn’t bank on it. And then beyond, is it statistically significant, is it clinically meaningful?
So, a difference could be statistically significant, especially if it’s in a very large study and they have a whole lot of data.
But sometimes, is a 0.1 difference in CRP, a marker of inflammation, is that clinically meaningful? There might be a certain difference in hemoglobin A1C, is every single difference clinically meaningful?
On the other hand, sometimes it might seem like a very small difference. For example, with weight loss, we know that even a 3 to 5% weight loss, to some people that would be like, “Are you kidding me? That can’t possibly be meaningful.” But we know that indeed it can be, especially for people with say visceral adiposity and so forth.
So, it is really important to ask both of those questions. Is it statistically significant and is it clinically meaningful?
Oftentimes, if it’s a small pilot study, it might not be statistically significant, even though it seems to have a strong association shown, and that just tells you, okay, this is something to keep an eye on because now that will probably beat the foundation for a larger study that will enable the researchers to find if it is indeed a true association to find it statistically significant.
Melissa (38:35):
So, the smaller pilot study, because it’s like just a numbers thing at that point, because if they don’t have many people in the study, a larger group who studied it changes the … I don’t know how to say it, you explain it. You know what I’m trying to say.
Karen Collins (38:50):
Well, first of all, they would often do a small pilot study as groundwork to be able to do a large study. These human studies are very, very expensive. And so, you don’t just go plopping down money until you have refined, does this method of testing show what it should? Does this intervention work? Do people actually follow it?
All the things, it allows you to iron out problems in a small group before you are spending all that money on a big study. And secondly, it’s important because if you’re looking for grant support, you need to show sort of proof of concept. I mean, build your case for why this is a reasonable study to do. So, those pilot studies help enable that.
And we can still learn from those pilot studies. It’s just that in a small group, if you’ve only got 12 people to have a statistically significant difference, it’s going to have to be a huge difference.
When you’ve got a massive population of thousands of people or even 500 people, even a smaller difference can become statistically significant. It’s a danger on both sides because it could be significant just because it’s a massive group of people or it could seem like it’s not significant. But in part that is because it’s a pilot study and so that next study becomes really important.
Melissa (40:17):
Okay. Very good. And then I kind of got us off track a little bit, but what are the other things when we’re digging into this article beyond looking at the results?
Karen Collins (40:27):
Well, I think it’s important to see how a study fits in the context of overall research. We’ve touched on that. For example, while across a whole population, reducing sodium consumption will always reduce blood pressure, the decrease will be smaller if people in the study did not have elevated blood pressure to begin with at baseline than for people who do have hypertension.
So, you have to look at who’s in the study. And likewise, if people in a study don’t have elevations in lipids or biomarkers of inflammation, a study that finds no difference or no change doesn’t mean that there wouldn’t be a difference or a change in people who do have higher levels of that baseline risk.
And there can be a variety of reasons why any individual study is kind of an outlier from the overall body of research. So, it’s important to always try to put in context.
And that’s where I think turning back to what you said earlier, Melissa, about nobody can read all of the studies and that’s where when you run across a study, I recommend that you turn then to where there are some strong evidence-based reviews from major organizations or authoritative sources that have looked at the big picture. And say, “How does this finding fit with this statement of overall research?”
It’s not that you need to read every single study to be able to do that but put it in context of what our strongest statements of evidence are.
Melissa (41:57):
Yeah. I’m glad you addressed that because we do say “How does it fit into the overall body of evidence?” And that concept in and of itself is helpful, but then how do we see what the body of evidence says? So, these reviews that you’re recommending by reputable organizations.
Karen Collins (42:14):
Yeah. And that is the beauty of as much as we’ve got crazy information available to us today, there are very solid reviews that the authors spend huge amounts of time collectively analyzing the data, grading it for quality, thinking about its implications, and they know the field, so they know which measurement tool is strong and things like that.
It doesn’t have to all come from our knowledge base. Those things are there and that’s the place to look.
Also think about what is the purpose that you’re looking at this study for. If you’re looking at it in terms of population recommendations, then you do care about what it means overall to people. But if you’re talking about it for a given individual, patient or client, then it matters how the people in that study or the conditions in that study, are they the same as the person you’re talking to or not.
So, for example, changes in carbohydrate or time-restricted eating may show significant results for people with insulin resistance that aren’t seen in others.
It might be a whole host of different dietary factors based on age, on how physically active someone is, and whether they have a baseline health condition. And a study in healthy 20-year-old college people, because that’s who’s handy at the university, doesn’t necessarily reflect the population of sedentary 60-year-olds. That is the person you’re talking to right now.
So, you really do have to look at regardless of whether the results are statistically significant and clinically meaningful in the people in that study, are they clinically meaningful for your purpose? That’s really a separate question.
Melissa (44:07):
Yeah. And we hear this a lot, what are the limitations and does this or can this apply to a different population and the population studied?
Karen Collins (44:17):
Exactly. And sometimes it does, but you can’t assume that it does. You can only assume that it’s covered by the people in the study. And again, sometimes it might be an overall population, but if only 20% of them have the health condition you’re interested in, well then, it may not be as representative of what you can expect as a study in a different group.
And sometimes that explains why are these two different studies showing different things? Well, this one was in this group of people, this one was in this group of people, and it could be a whole host of differences between them.
Melissa (44:55):
Right. Very good. I think you touched on this a little bit, but if you maybe give us an overview of like, the different aspects of a research study that are important to consider. We talked about the results a little bit, but are there other things that you wanted to share regarding that?
Karen Collins (45:11):
Sure. So, the results and the subjects who were in the study, first, are they even people? Or if we talked about animals or cells, and then if it is people who are the people.
Then I think, one of the hardest obstacles for me as I kind of began this journey into building research translation skills was, it’s a little embarrassing to say, but I used to prefer to read the abstract, the introduction, and then skip to the results and the discussion, and basically skipped the methods because that seemed overwhelming to me.
But that is where really critical information is. And even if we don’t understand every test or every measurement, it is important for us as dietitians, as health professionals to look at that. And if you don’t, that’s the kind of thing to look for in those larger evidence-based reviews of that, because they’ll call it out.
So, for example, there are some studies looking at sodium and blood pressure. And in a population study they would, for convenience and cost, use just a spot test, a urinary sodium test, and then put it in this algorithm that was supposed to represent sodium consumption.
But research has very clearly found that to accurately estimate somebody’s sodium consumption through a diet recall, we can do that clinically in our counseling with someone by asking them about the foods they consume and so forth.
But we all know that that’s a rough estimate that will guide your counseling. But if you need a clear, strong data for a research study to test it against certain outcomes, you need a much more solid or specific number than that dietary assessment.
So, they would use urinary levels, but as I said, these spot urines that have been used in some studies and then concluded that urinary sodium doesn’t matter. Unless you are above 5,000 milligrams a day, it doesn’t make a difference.
It was the methodology, because the recommendations are very clear that it needs multiple 24-hour urinary sodium to accurately assess sodium intake. In the studies that use that, there we see a very clear relationship. So, that’s an example.
Or a lot of people are interested in magnesium right now. People need to know that a serum magnesium level does not reflect dietary intake. We have body pools that in order to maintain homeostasis and maintain those levels, we can take it in and out of bones, which is where actually the majority of the magnesium in our body is.
But people will look at a urinary serum level; but no, that’s not a sign about how your diet is. You have to look at how things are measured.
Secondly, one of the things that we’ve done a lot of work with as we look at research in my membership program is talking about dose-response. So, often in an observational study, they’ll compare high consumption versus low consumption of something, whether it’s to be beneficial or as a risk.
But that doesn’t tell us anything about the people in the middle. And we can’t assume that it’s a linear relationship where high is more of this, that every step along the way is going to have a linear relationship.
So, an analysis that test for what’s called a non-linear relationship and a dose-response. They look at whether it’s risk like say, related to alcohol or meat or benefit from a specific nutrient or a food. Is there a threshold below which the risk for the benefit really isn’t significant?
Or is there a plateau above which increasing more and more and more doesn’t continue to show a stronger association? And this is true for intervention studies too, because just putting someone in a certain dietary intervention group, call it whatever it is, diet that is not the same if you can’t assume that everyone in that group ate exactly the same way.
So, you really need to look at how much, what is the dose of whatever it is and what is the relationship there.
And then a third thing I wanted to mention is that we’re more and more seeing meta-analyses, which adds a terrific great value by combining different studies and analyzing them together. But it also poses challenges.
So, one example would be that you’ll see in a meta-analysis, this combines data from a bunch of studies and analyzes them together. There’ll be a summary statistic of an association.
But we want to know, did all the studies in that analysis basically show a similar thing or was that the score when they’re all put together, but actually very inconsistent results in the studies, which is very important. Because any of the recommendations, the major recommendations that we look at, that’s a big part of what they look at.
And if the results are very different in different studies, it doesn’t matter what the one summary is, that will be graded as very limited evidence because that needs to be looked at further then was it because the studies did an intervention differently?
They analyzed it differently, they had different people in them, or did some studies adjust for certain confounders and others didn’t. There’s a whole host of reasons these studies could be different.
But before we assume something just based on that one summary analysis, and this is shown in those meta-analysis, you don’t have to guess at it. It might be shown in a forest plot or there are different statistical tests that identify how much … it’s called heterogeneity, how consistent or how much difference is there.
And so, as important as this meta-analysis are becoming, that is something I would encourage people to look at.
Melissa (51:09):
Great. As we’re heading towards wrapping up, I have several more questions for you, but I was just curious if you could just address some of the most common challenges that you’ve seen, maybe with your membership group or just among colleagues or even with the general public, if that applies. Just some common challenges that you see in understanding interpreting and translating just nutrition research in general.
Karen Collins (51:36):
Sure. So, a lot of this we covered, so I’ll be kind of bulleting these things together. But another concept that comes a lot is we’re talking more and more about dietary patterns. That it’s not individual foods and nutrients as much as a whole overall dietary pattern.
But see, how do we define that or how do we measure it? So, just because I call it a Mediterranean diet or all of these diets called Mediterranean the same, are they implemented the same by different people? There are scoring systems that are usually used to identify high or low alignment with a certain name the dietary pattern.
But we have to recognize that, especially in these observational studies, that those scores are generally comparing people not to a certain standard, this is what an ultimate Mediterranean diet is. So, how are you compared to that?
No, they’re comparing to different people in the study. So, for example, if my study group, if the people in a study were people like when my son was 16-years-old, all his friends, a high Mediterranean diet score would not be a very high bar to reach for in terms of say, amount of vegetables consumed or something like that.
Whereas if you’re talking about a Mediterranean population, especially formerly not current, or in the Adventist health population that is largely vegetarian, high vegetable consumption is a whole different amount of vegetables than in some other populations.
And so, you have to recognize, look with consideration. I mean, ideally you see a dietary pattern score associated, look at the data and it should be there. So, exactly how many vegetables were those people eating or exactly how much whole grains were they eating? Or how much fish, whatever it is, because that changes how you would interpret that in the advice that you would give. So, I think that’s important.
We talked about making sure you think about who’s in the study and what their baseline level is. When you’re looking at effects or changes or associations, really thinking about the quality, the strength of evidence, which there are now scoring systems that some researchers will use, especially for example, in meta-analyses.
You have to remember, and this is one of the other things about meta-analysis that I think has made it harder for us as we try to read these studies, is the quality of the data of a meta-analysis is only as strong as the quality of the studies in the study.
And when you’re reading a single study, you can look at those methods and you can see who is included, who was excluded, how did they measure things.
When you’re seeing this meta-analysis of multiple studies, that’s not so easy. I mean, if you really wanted to do it, you’d have to backtrack to each study in the meta-analysis. But there are often grades where they have criteria for the strength of evidence.
And one of the tricky things is just that some of the grading systems particularly emphasize randomized control trials as the strongest evidence in downgrade prospective observational studies.
But as we said earlier, you have to be aware that for some research, the strongest evidence when you’re talking about a long-term condition is going to have to come from a prospective observational study.
So, look at the grade, but then think about what the grade is based on. We talked about thinking about dose, how important that is. And then I think the other thing is beyond understanding and interpreting the study that a whole another dimension comes into when we translate that into advice and strategies where different individuals can work toward the same goals, but in different ways.
We know that food culture, family culture, all these things are so important, or people may be concerned about one health risk, but have other health conditions that you also need to consider.
And so, the most important thing is to find a strategy that will work for an individual in their context, in their health. And that means we have to know the research, but then think about what we as dietitians know about food composition and other food sources of a nutrient, or what we know about behavior change and how you can gradually work toward something rather than throwing down a list of 45 rules to follow.
So, I think all of those pieces, understanding the science, interpreting what the research showed and look at what’s behind their conclusions, and then thinking about how you would translate it. And that is a strength that dietitians bring to the table, by the way, that even the researchers definitely have a leg up in terms of understanding the statistical analysis and all that.
But most of them recognize that when it comes to actually implementing it, it does require this additional body of knowledge that is what dietitians bring to the table.
Melissa (56:45):
Absolutely. I think we touched on this a little bit, and we’ve covered so much information. I don’t want to go down another tangent here, but it is something that I often ask my guests when we’re talking about research and the quality of the research or the strength of a study. A lot of times industry funded research gets criticized.
So, I would just love to hear your thoughts on that. Good, bad, the ugly, whatever. When you think about industry funded research, what do you think of it and what do you recommend when you’re working with your membership group?
Karen Collins (57:24):
Well, I think we have to recognize, again, we’ve talked many times today about how expensive research is. And federal grant support is getting harder and harder to obtain from what I understand.
So, to some degree, without industry support, this research wouldn’t happen. So, the important questions really are not, I don’t think where the money is coming from, but what that money has bought.
So, at the end of a research paper, it should say both what the funding was and what role any source of funding had. For example, did they get to have control over whether a study was published based on its results, or is that going to be at the discretion of the researchers? Did they have control over study design or was there control there? That’s what’s important to me. And then I would look at that in context.
So, if the only studies that show support for something, for a certain finding are coming from industry funded research, and there is other research that’s been funded, say by NIH or other grants, and that shows, no, it wasn’t significant at all. Well then, I wouldn’t know why, but that would certainly prompt me to question.
Melissa (58:39):
Look further. Right.
Karen Collins (58:40):
But just like the people we work with, we all want easy, black and white, simple either-or answers on industry-funded research. That’s just not as simple as that, I don’t think, as far as the defining research quality.
Melissa (58:55):
Thank you. So, now that your membership group, I believe it’s been running for almost three years now, right?
Karen Collins (59:00):
Yeah.
Melissa (59:01):
So, what are you hearing from your members about why they join, why they stay or what they’re valuing from it?
Karen Collins (59:09):
Well, I think one of the things that I’m hearing and part of why I designed it the way I did, is that we do have a range of expertise and a range of practice settings among the members. So, it’s a dietitians-only membership, and it is within the areas that I generally feel comfortable talking about the research.
But we’ve got people in cardiac rehab or outpatient cardiovascular counseling, preventive cardiovascular health, as well as people in cancer survivorship groups, community cancer organizations, oncology, clinical dietitians, dietitians and private practice diabetes educators.
And the thing is that even though they’re in different practice settings, or we tend to be sort of siloed in our specialty practice, in reality, the people that we see are not siloed, so someone who’s in cardiac rehab may have had a cancer diagnosis in the past. And you better believe she’s listening to what you say through a lens of her concern about cancer recurrence.
Same thing, you might be having a cancer patient or somebody who wants to lose weight, but they have cardiovascular issues and that you need to be thinking about how you’re making recommendations in the context of that, or you want to have resources for those interests, and they wouldn’t normally be in your kind of toolbox. And so, this interaction is something that people really value.
Our three focus areas, as I said before, are understanding the science. So, understanding differences in sodium-sensitivity of blood pressure, or how emerging evidence suggests that the optimal diet during cancer treatment may actually turn out to be different with different types of cancer treatment.
That’s really kind of emerging stuff on the horizon. And we talk about communicating the science accurately and confidently. So, there’s a lot of questions dietitians are getting asked in certain environments about the rise in early-onset colorectal cancer.
So, I had an interview with one of the researchers in early-onset colorectal cancer who helped us both understand the, the research, but also, what are they the real talking points that we need to be sharing.
And dietitians love the dietitian cheat sheets, some of which I do provide. I mentioned those earlier. And some of those I do provide to my email subscribers, but many more are inside the membership. And they use those for presentations, for blog posts, for social media.
And we have a membership app, which means that they can quickly look stuff up right in the middle of on the spot with a client. Click to the dietitian cheat sheet on X, Y, Z and be able to address their questions.
And then the third piece is the community, which is a huge part of what the members value. Kind of one of the growing realizations I’ve had even since I opened the membership is how many dietitians today are practicing really in relative isolation and without a lot of opportunity to strategize with colleagues about how to answer questions.
So, one dietitian in the Circle was asked to give a presentation to physicians in her area about nutrition and breast cancer, and she asked for input from the group on what do you think I should cover?
Other people have been doing a cooking demo in the community or presentations to some specific community group and sort of crowdsourced what might they cover or what recipes would you use, things like that.
And even hearing in the way information moves at such fast pace today, as we have been talking about throughout our time together, you might know I’ve not gotten a question about something yet, but if a dietician in another area has gotten a question about some hot topic, you better believe you probably are going to be getting question on that.
And so, people really value like, heads up. Okay, I’m going to be ready with an answer on this because you can kind of predict that it’s coming.
So, those three pieces seem to be what people are loving. And overall, some people that joined have known me for decades and so joined with no doubt or no question, other people have said, “I really thought I was just going to join for like a month or two, check it out and probably not stay, but there’s no way I’m leaving this.” And overall the vast majority of people, as they join, almost everybody stays.
Melissa (01:03:31):
Yeah. I’m sure some people just kind of want to dip their toe in and say like, what is this all about?
Karen Collins (01:03:35):
Yeah. Well, and it’s scary. I mean, it seems like what, it’s very satisfying to find that.
Melissa (01:03:40):
It seems daunting, but it’s very doable.
Karen Collins (01:03:43):
Yes. Doable.
Melissa (01:03:44):
Wonderful. Well, I would love to just hear maybe a few bottom-line takeaways, at least one for the general public. And then, one for dietitians or other healthcare professionals. And then of course we want to reiterate your website and how people can get ahold of you.
And you had mentioned there’s information that’s available to anybody on your site, but then there’s your newsletter where people get a little bit more that they won’t just find on the website, and then there’s the membership. So, it’s kind of like three inner circles there.
Karen Collins (01:04:15):
That’s right. A lot of threes today. A lot of threes.
Melissa (01:04:17):
I love it. It’s the whole media, number three.
Karen Collins (01:04:19):
So, for the public, I think really the bottom line out of all this, it’s maybe not as specific as some of the examples we’ve talked through today, but it’s really that if you are interested in nutrition and you believe, you know that it’s significant, you need to be as selective about the media you consume as the food you consume.
It’s easy in today’s world to just scroll and scrolling is entertainment. That’s great. Find new recipes, new decorating ideas, new books you want to read. That’s what scrolling is.
If you recognize that nutrition information is important, it’s not just something to scroll through, read a headline and think you’ve got facts. What I suggest for people that that’s kind of how you get your nutrition information is create a folder, whether it’s in your email or in your saved files on whatever social media channel you have.
And that way when you see something as you’re skimming, but you’re really not in the mindset to critically think about it and look at these points that we’ve identified, put it in that folder, that saved group.
And then when you have time and you’re ready to actually look with a critical eye at these points that we’ve talked through today, then you can actually go through and consider if this is something worth even paying any attention to. Or if you’re just going to say, “Okay, I don’t need to think further about that idea.”
And so, I want to mention that in your Sound Science Toolkit, Melissa, one of the first things I think at the top of that is a guide from IFIC, the International Food Information Council that actually talks through and there are some red flags and some errors and reasoning that would be great to just have people …
When you have that in your mind and you can just mentally run through, “Oh boy, because this piece sounded really interesting, but it actually has a whole lot of little red flags that are identified there.”
Then that’s something maybe you then delete from that file that you were going to look at or whatever. So, I think that’s really my main message for the public is we need to be selective.
And for dietitians and other healthcare professionals, I guess it’s a plea is my main message is that just like I was feeling earlier in my career, research translation can seem like something too sciencey for us, too challenging, daunting, but we need to lean into this.
If we don’t do it, who is going to do it? And think about who is, and that should be enough motivation to you to do it.
People are confronted with so much information today. We need to help them put it in perspective, help them set priorities based on the strength of evidence. And so, if this seems daunting, one of the things I would suggest is to build sort of this mental framework.
We talked about a number of the factors that you can sort of use in that. And the checklist that I created for you to access from today’s show notes is a great starting point. The way I created it is so that it could be used with a patient or in a class to talk through, “Okay, you ask this thing, let’s look through this.” It’s a very simplistic framework, but it’s a starting point.
And then as you learn more about things to look at, like say the heterogeneity in a meta-analysis or some of these other factors we talked, you can build that in and with time, the more you work through that framework, you do become more skilled. It takes less time and you become more confident.
Melissa (01:07:49):
And more familiar. It becomes more familiar.
Karen Collins (01:07:53):
Yeah. And I think just like we tell our patients and clients, we need to choose our sources wisely too. It’s not possible for most dietitians or healthcare professionals to do, as we said earlier, to do a thorough dig into every study that comes up and the overall body of research.
So, you need to have trusted resources, but dietitians can uplevel their skills. That’s, to me the important thing. We have the background, we have the science background, and we don’t have to burn through all our time and mental energy.
Just like learning to cook or learning to speak a foreign language, it doesn’t come by just sitting on it. The fastest way to build those skills and your confidence is to jump in and practice do it, and ideally do it in a place that gives you some support.
So, maybe you join a journal club, maybe you really actively participate in a DPG. Maybe you are really intentional about the type and content of the CPE that you select to intentionally bolster those skills.
Or in a program like my Daunting to Doable Nutrition Pro Circle that with support, you have the background, and these are skills we can build. And I think we really need to accept that call.
Melissa (01:09:06):
I agree. Thank you so much. So, your website is karencollinsnutrition.com. We want people to subscribe and receive your nutrition research updates by email. There’s the dietitians only membership, I have links for all of these in the show notes at soundbitesrd.com.
And thank you for creating the special tip sheet, how to make sense of nutrition headlines, for this podcast. That will be in the show notes as well. And thank you for mentioning my Sound Science Toolkit.
I mention it from time to time on the podcast, but if you’re listening and you’re not familiar with it is just a curation of different articles, books, videos, tip sheets and so on, that would help you think more critically about nutrition in the news. Look for those red flags, understand hazard versus risk, understand correlation versus causation.
And it was really created for my dietitian peers, but anybody can access it. So, you can subscribe with your email, and they’ll get a login password for that as well on my website at soundbitesrd.com.
Is there anything else that you wanted to mention about how people can connect with you? I know you’re on Instagram and Facebook at Karen Collins Nutrition. I’ll also have your LinkedIn link in my show notes as well. But is there anything else I didn’t mention?
Karen Collins (01:10:28):
I think you really hit the highlights. So, depending on your preference, there’s multiple different ways to connect with me and different levels of engagement. The big thing is that I’m working on a bunch of new things that will be coming both as new benefits in the membership and also other ways outside of the membership to serve my fellow dietitians.
So, I’d love for you to subscribe to my news list and that way you’ll start receiving the research reviews now, and then you’ll be the first to hear when these additional things become available.
Melissa (01:10:59):
Exciting news. But wait, there’s more. Wonderful. Well, thank you so much, Karen, for coming on the show and all of the awesome work you do. Congratulations on your medallion award.
That is so wonderful. You are so deserving, and I’m just honored to call you a colleague and friend, and I’m just excited for everything that you’re doing.
Karen Collins (01:11:17):
Thank you, Melissa. My pleasure being with you today.
Melissa (01:11:20):
Wonderful. And for everybody listening, as always, if you like this episode, share it with a friend. Listen to another episode, follow the podcast on Apple or Spotify or wherever you consume podcasts.
But most importantly, as always, enjoy your food with health in mind. Until next time.
[Music Playing]
Voiceover (01:11:41):
For more information, visit soundbitesrd.com. This podcast does not provide medical advice. It is for informational purposes only. Please see a registered dietician for individualized advice. Music by Dave Birk, produced by JAG in Detroit Podcasts, copyright sound bites, Inc. All rights reserved.
LISTEN, LEARN AND EARN
Listen to select Sound Bites Podcasts and earn free CEU credits approved by the Commission on Dietetic Registration (CDR) for registered dietitian nutritionists and dietetic technicians, registered. Get started!
Get Melissa’s Sound Science Toolkit here!
Partnerships:
Sound Bites is partnering with the Association of Diabetes Care and Education Specialists (formerly the American Association of Diabetes Educators)! Stay tuned for updates on the podcast, blog and newsletter!
Sound Bites is partnering with the International Food Information Council! Stay tuned for updates on the podcast, blog and newsletter!
8.5.24 – Thank you both so much! The “nature of science” is not bottom line or black and white. We learn so much more when we ask questions, see the data points and think critically. Such a well done and informative podcast!
Sign up for my monthly newsletter and episode eblasts so you never miss an update!
Listen on Stitcher (Android)
Install the Stitcher App
1. Search for “sound bites with melissa joy dobbins” 2. Choose Play Current Episode or Add to Playlist
Choose “Play Episode”
Subscribe & Review on iPhone
Open the “Podcast” app on your iPhone
Search for “Sound bites with melissa joy dobbins”
Open the podcast and click “Subscribe” and your done!
Write a Review
Click “Reviews”, then “Write a Review”.
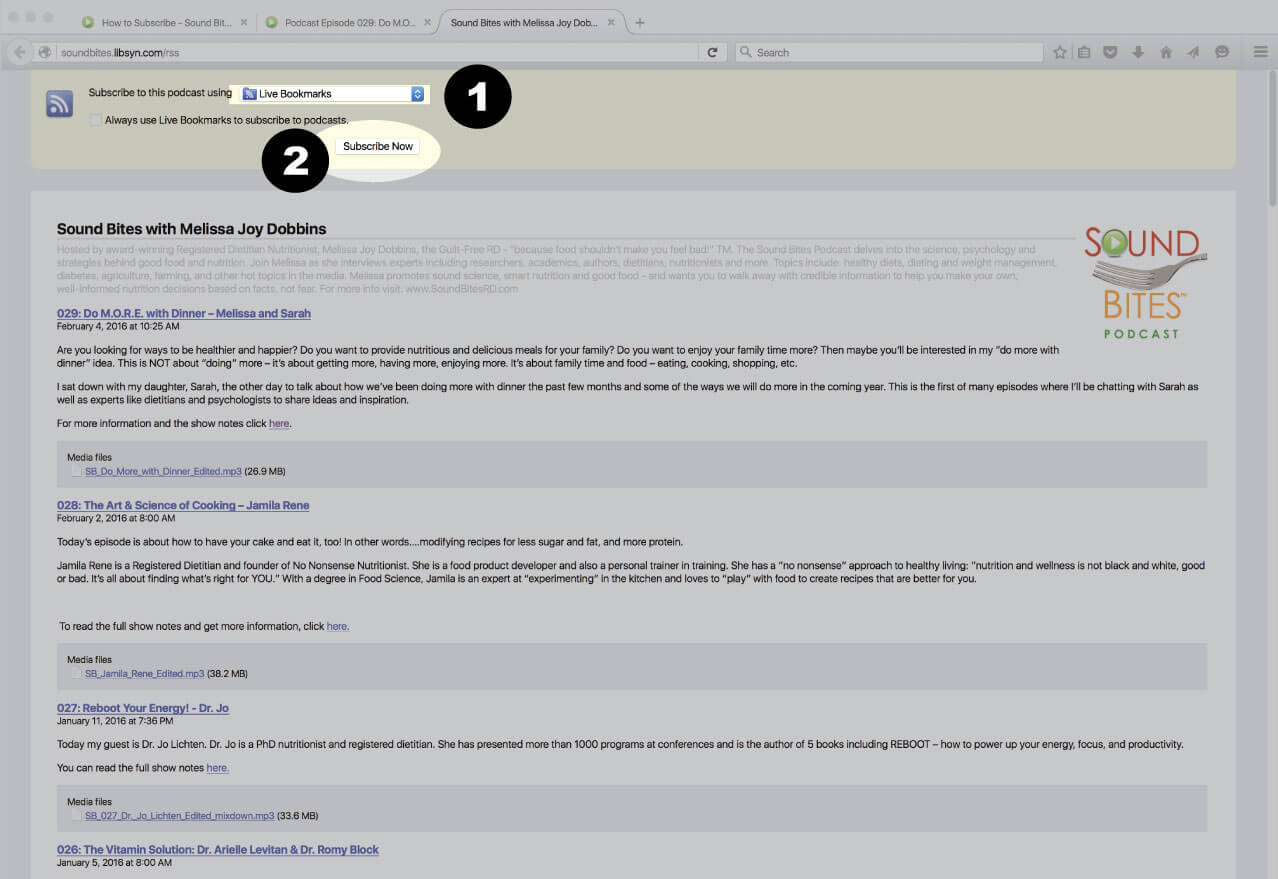
Subscribe via RSS Feed
Navigate to any podcast player . Click on the RSS feed icon.
Click on the RSS feed icon.
Click on RSS Feed
Choose which application you would like to use to receive the RSS feed
Click “Subscribe Now”
Confirm settings and subscribe.
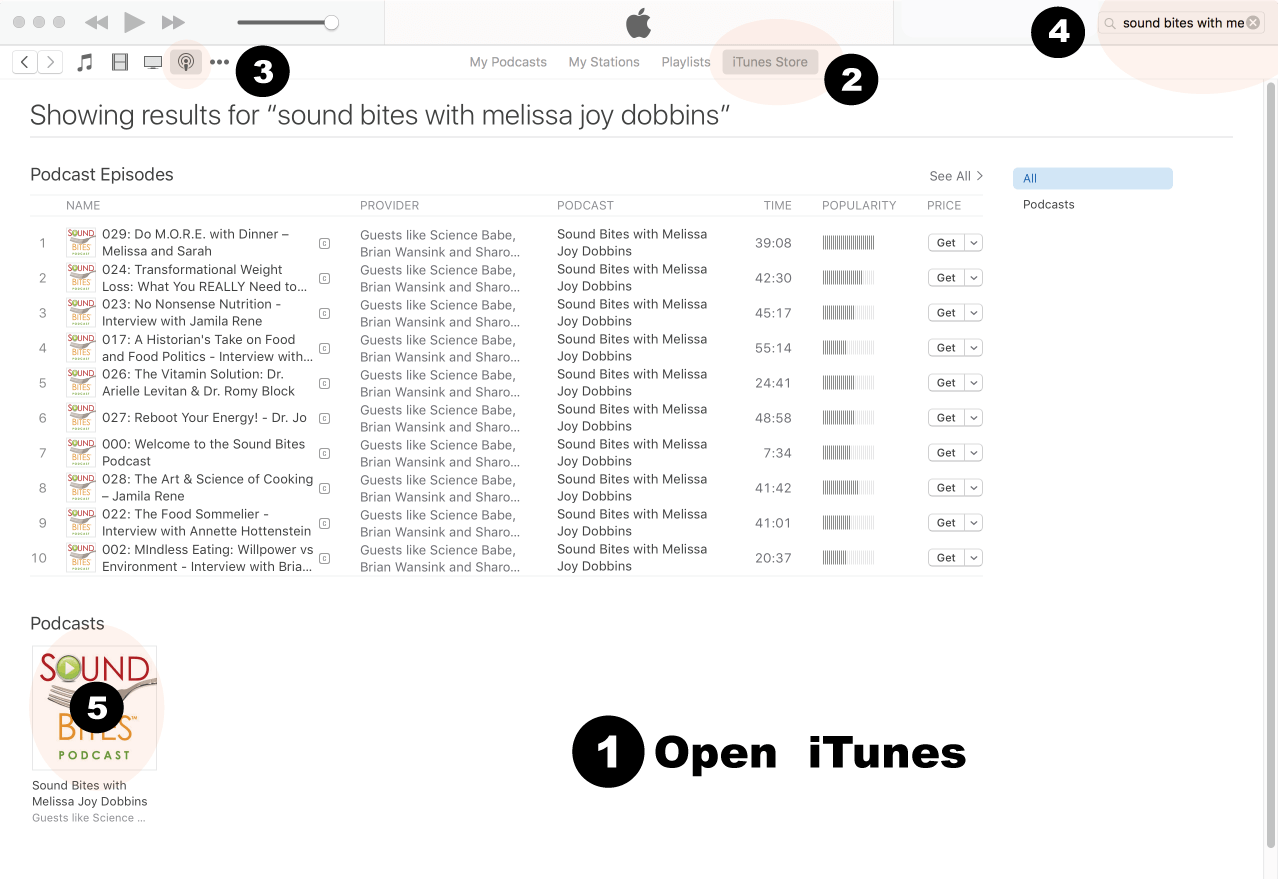
How to Review in iTunes
Open iTunes desktop application
Click iTunes Store
Click on Podcasts
Search for “Sound bites with Melissa Joy Dobbins”
Click on podcast image
Search for Sound Bites podcast in iTunes
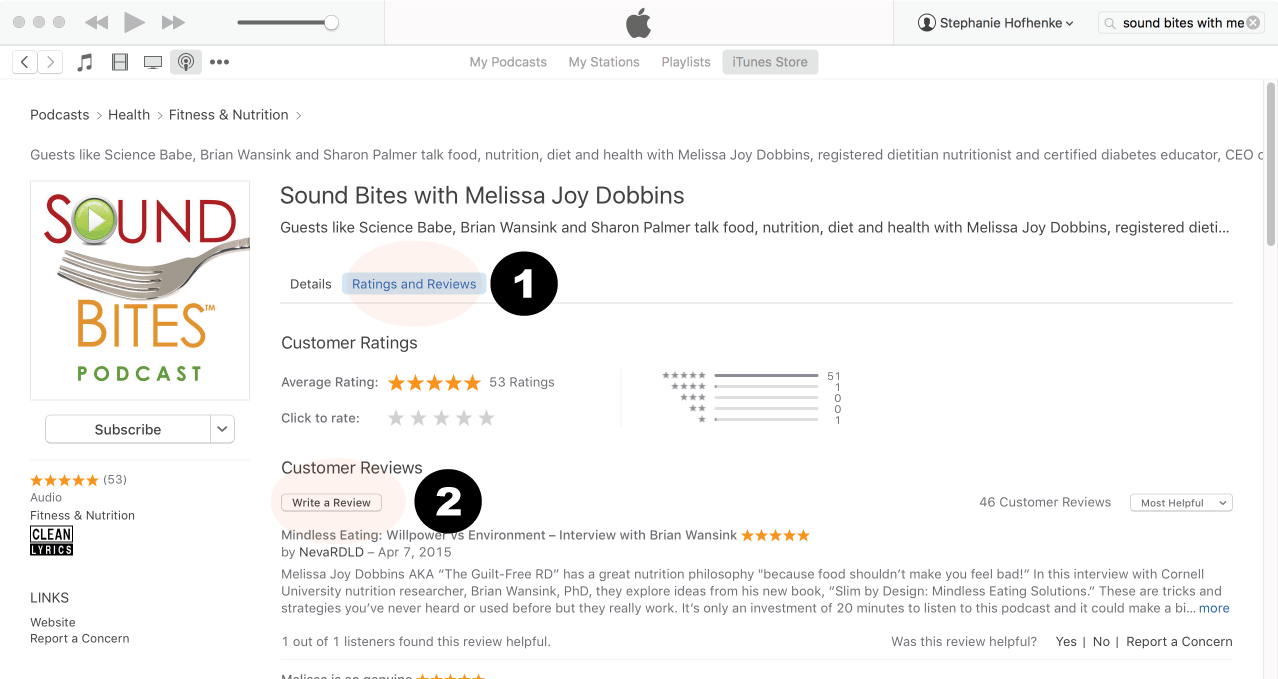
Click Ratings & Reivews
Click Write a Review
View reviews and write your own review.
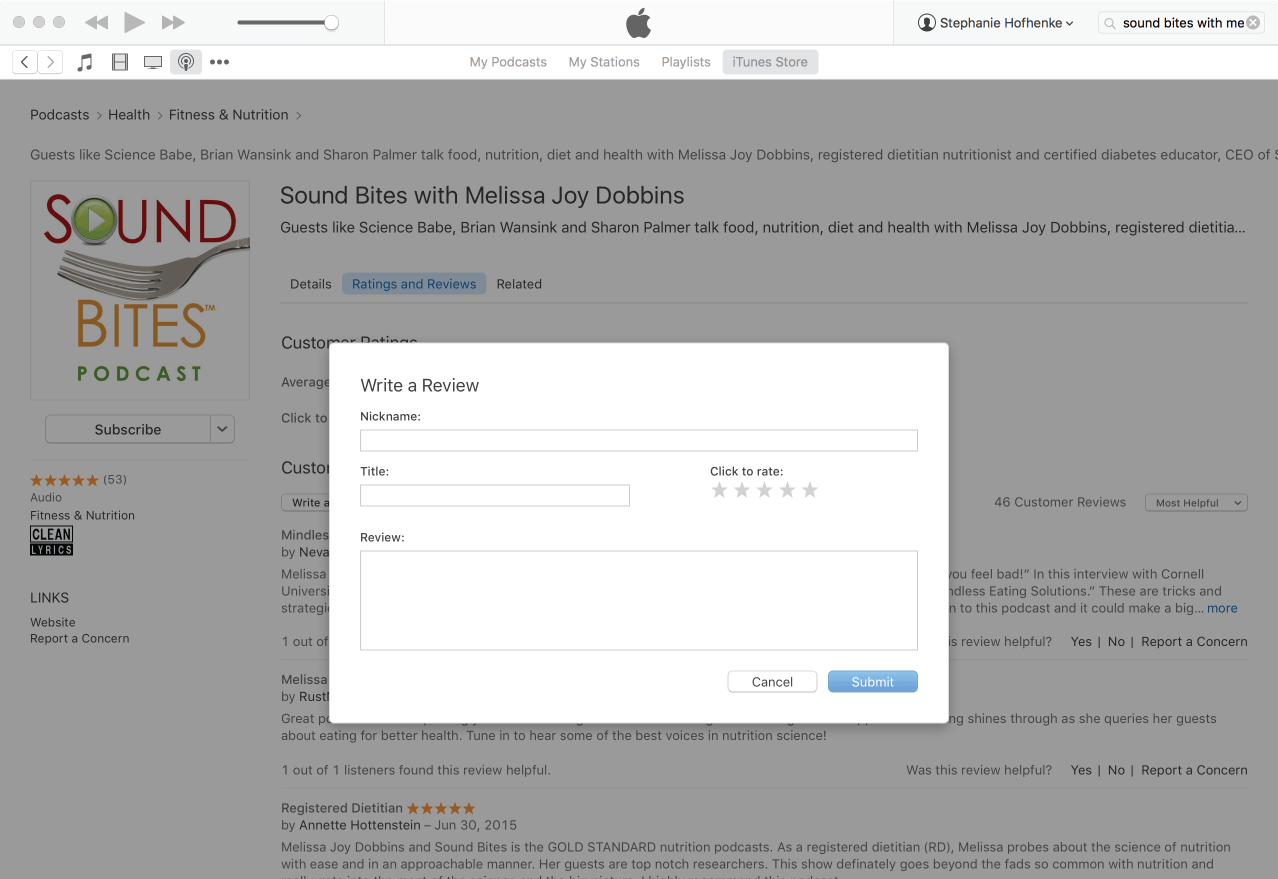
Write your review…. Thank you!
Write your review!
How to subscribe via iTunes
Click here to view the Sound Bites Podcastin iTunes, then click the blue “View in iTunes” button. This will open your iTunes application directly to Sound Bites Podcast. Click the “Subscribe” button, and your done!
 Karen is a registered dietitian nutritionist whose tagline – “Taking Nutrition from Daunting to Doable” – highlights her focus on helping people cut through the confusion of nutrition headlines and put complex information in perspective within the “big picture” of overall research. Karen is a consultant, speaker and writer who focuses on translating current nutrition science related to cardiovascular health, cancer prevention and survivorship, and their intersection in cardio-oncology.
Karen is a registered dietitian nutritionist whose tagline – “Taking Nutrition from Daunting to Doable” – highlights her focus on helping people cut through the confusion of nutrition headlines and put complex information in perspective within the “big picture” of overall research. Karen is a consultant, speaker and writer who focuses on translating current nutrition science related to cardiovascular health, cancer prevention and survivorship, and their intersection in cardio-oncology.











8.5.24 – Thank you both so much! The “nature of science” is not bottom line or black and white. We learn so much more when we ask questions, see the data points and think critically. Such a well done and informative podcast!
Thank you, Nancy! So glad you liked it. Karen does amazing work and I was so happy to have her on the show!
Melissa