Celebrating over 1 Million Downloads and 50,000 Free CEUs on the Sound Bites® Podcast | NEW: Get 1 years’ worth of CEUs with the new 15-CEU Podcast Course
Disclosure: This podcast episode is a paid collaboration between Sound Bites® and Potatoes USA, the nation’s potato marketing and research organization, representing more than 2,500 potato farming families. Potatoes USA is committed to providing the nutrition science community with evidence-based information about the role of potatoes in healthy lifestyles.
Carbohydrates: Consumer Confusion, Current Guidance & Future Recommendations
The physiological impacts of eating carbohydrate-containing foods are much more complex and individualized compared to dietary protein and fat; yet, there is still no globally accepted way to define ‘carbohydrate quality’. While some researchers often rely on the Glycemic Index as a leading marker for the quality of carbohydrate-containing foods, the research does not align with this approach. In fact, published studies continue to question the variability, reliability, and utility of the Glycemic Index, especially among the general population.
During this episode, you will hear from cardiovascular physiologist Sid Angadi, PhD, FACSM, and food and nutrition scientist Julie Miller Jones, PhD, CNS, CFS, as they take a deep dive into the latest science and recommendations surrounding carbohydrate-containing foods. Tune in to learn about the limitations with using glycemic index as a marker of carbohydrate quality and get up-to-speed on the research that’s currently underway to develop a new definition for quality carbohydrate-containing foods.
Tune in to this episode to learn about:
Consumer confusion about carbohydrates and their role in a healthy diet
What the current nutrition guidance says about carbohydrates
The complexities of carbohydrate-containing foods
How the nutrition science community currently defines carbohydrate quality
Resistant starch, fiber and other nutrients in carbohydrate-containing foods
The evolving scientific literature on the Glycemic Index as a marker for carbohydrate quality
Insights on how to best define quality carbohydrates moving forward
The strengths and limitations of epidemiological research versus randomized controlled trials and the appropriate way to relay findings from both types of research
Takeaways for the public, health professionals and the research community regarding carbohydrate-containing foods
Resources and research on carbohydrates
Most people using the glycemic index table – it’s really a dart board whether the value that you picked had anything to do with what you ate.” -Julie Miller Jones
Siddhartha Angadi, PhD, FACSM
Dr. Angadi is an assistant professor and cardiovascular physiologist at the University of Virginia. His research examines the intersection of diet, exercise and drugs in the setting of severe illnesses such as heart failure, cardio-renal syndrome and breast cancer (specifically in the setting of cardiotoxic chemotherapy). Some of his recent work in the nutrition realm has examined the vascular effects of high-fat diets in adolescents and the impact of glycemic index and cereal fiber on vascular function and cardiometabolic markers in adults. Dr. Angadi received his PhD at Arizona State University and was a post-doctoral scholar at the University of California, Los Angeles.
There is huge variability in people’s responses to carbohydrate consumption. The thing to understand here is that to some extent these responses are driven by the food you consume, but on the flipside, these responses are also driven by things such as your age, genetics (which is your family history) whether you exercise or not…and it makes drawing conclusions from these sorts of markers particularly difficult.” – Sid Angadi
Julie Miller Jones, PhD, CNS, CFS
Dr. Jones, a Certified Nutrition Scientist and Certified Food Scientist, is a professor emerita from St. Catherine University in St. Paul, MN where she taught for over 40 years. She received her BS from Iowa State University (ISU) and her PhD from the University of Minnesota. She was named as St. Catherine’s outstanding professor twice and was awarded the Myser Award by the alumnae as a “professor who made a difference in people’s lives.” She also received the Alumni Impact Award from the Department of Food Science and Nutrition at ISU at her 50th Homecoming.
She has written many papers and is a frequent speaker for many professional conferences and consumer organizations, locally, nationally and internationally on carbohydrates, grains and whole grains, diets and food safety. She was active in many professional organizations and was president of American Association of Cereal Chemists International (AACCI). She has received numerous awards and is a fellow of the IFT, AACCI and ICC.
We were concerned that [the] foods important on people’s tables, that are culturally important and have nourished us for millennia were being not considered as quality… We really wanted to be able to define what is a quality carbohydrate food.” – Julie Miller Jones
Resources:
Sign up on the Potato Goodness website to receive the latest potato nutrition research, education resources and other valuable materials.
In fact many years ago there was a very interesting study that looked at the
diets of World-class Kenyan marathoners. And the reason why they looked at
Kenyan marathoners was because the top 95 or so, or top out at the top 100
marathon times are from Kenyan marathoners specifically they’re from one tribe
called the .
And about 70% of the daily calories came from carbohydrates. So carbs are
really the fuel of choice for high intensity activity as well. And that’s largely
because you just get more ATP or more energy per liter oxygen compared to all the other fields. If you want to be fast, carbs are the way to go, but yeah,
carbohydrates are fuel for your brain.
And the other thing to keep in mind is we are not particularly good at storing
carbohydrate, which is why we keep needing to consume them
[00:13:26] Melissa: frequently. Yeah. We can only store so much glycogen in
the muscle versus our fat stores kind of unlimited there. I did a recent episode
with a sports nutritionist, Nancy Clark, and we talk about exercise and diet and
weight.
So back to carbohydrates, I, as I mentioned as a dietitian and a certified diabetes
educator, From firsthand experience that carbohydrates are diverse. And we’ve
talked about that, but from a nutrition science perspective, let’s talk more about
these complexities of carbohydrate containing foods.
[00:15:03] Julie: I agree it’s really very, very complex, not just in the simple
versus complex, but they are really difficult to often explain to people why they
are so important. For instance, we have high fiber foods and some of the fibers
that are in carbohydrates are only in carbohydrate foods and they’re not found in
fruits and vegetables.
So when people say, well, you don’t need to eat those grains or those potatoes
because you can get what you need in something else. That’s simply not true.
The fibers are in fact different and they have different physiological functions.
We want different kinds of fiber. And in fact, we know that cereal fibers do
some things and vegetable fibers do other things.
And those fibers let’s say maybe in a potato are doing a different thing and
trapping the starch in a different way. We get different glycemic and other
impacts by how big the carbohydrate molecule is, what its particle size is. For
instance, let’s just take oatmeal. If you want the most cholesterol lowering from
your oatmeal, you’d like to buy quick oats, not instant, because by opening the
structure of the grain, you actually release the beta glucan it’s more available at
the gut level. And the beta glucan then can actually impede cholesterol
absorption from the gut. Whereas if you want more laxation, would like to eat a
steel cut out or an old fashioned oat.
Or if you want more glucose control, it will leave more slowly from a particle
that slow to digest like an old fashioned oat or a steel cut oat. They’re all great
foods. They all contain fiber, the beta glucan, which can control glucose
passage into the bloodstream, how quickly it goes. They all are.Fermented in the large bowel to short chain fatty acids, but you just get that
little nuance of difference from different kinds of processing now, because I
don’t have any particular problem. I try to use a variety is a good way to go for
any kind of nutrition thing. And so pick a variety of kinds of things and
different ways of eating a food, just such as oats.
Just as an example, the matrix makes a big difference in terms of the bioactives,
as some carbohydrates of lots of things. They come in with some come in,
pretty clean. So you need the phytonutrients and the nutrients, and that’s all a
package to
[00:17:50] Melissa: look at. You mentioned the food matrix. Can you explain
that a little bit for our listeners?
It sounds like that’s the package, like everything that comes with it.
[00:17:59] Julie: Well, for instance, there’s something called resistant starch
and resistant starch comes in five different forms. But one kind of resistant
starch is simply the fact that in the time that the food is in the digestive track,
the enzymes can’t penetrate the wheat kernel or the corn kernel, the starch that’s
held inside.
The kernel actually doesn’t get digested. It doesn’t yield calories that are
absorbed. It only can produce a few calories when it moves to the large bowel
and is subsequently fermented to short chain fatty acids. And to be a little bit
non dinnertime talk, if you’ve ever in corn season to happen to look at the
output, which you have, you might see kernels of corn in the stool.
And that just as an indication that some of the starch that was in that corn didn’t
get attacked by the end of. That’s one kind of resistant starch. So there’s a lot of
kinds of, and that’s held in the matrix of the food. So that’s an example of
something being held in the matrix. Some people feel that all fibers should be
natural fibers because they think that the natural matrix makes the fiber more
physiologically.
I don’t adhere to that policy. I just talked about the effect of processing oats. So
you can get some advantages by opening the structure up and letting the fiber
function in the upper gut. And sometimes you want it to function in the lower
gut. So then something that isn’t necessarily in the matrix may be more helpful
so that you need both.[00:19:41] Melissa: Yeah. I mean, when we’re talking about the different kinds
of fiber, we’re going way beyond soluble versus insoluble you mentioned cereal
versus vegetable. There’s so many different types of fiber. I should do an
episode on that. Maybe you can come and talk about that and resistant starch,
which we really don’t hear about much.
I didn’t know that there were different kinds of resistant starch. So this is all
very interesting and just speaks to the complexity.
[00:20:03] Sid: Yes, you’re right. That carbohydrates are incredibly complex,
but it’s also important. Remember that different macronutrients and consumed
in different contexts along with sometimes different.
And they can favorably interact for instance. So a number of years ago, we
carried out an interesting little study in which we brought in a bunch of
adolescents and we fed them a high fat meal and examined their vascular
function at the end following the high fat meal. And sure enough, you consume
a high fat meal, your triglycerides go up, your vascular function goes down.
But when we send these individuals the exact same meal, but then we tacked on
all bran cereal with that, which had a lot of insoluble fiber. What we saw was a
lot of these abnormalities and vascular function largely were ameliorated. And
this was largely driven by the suppression of postprandial triglycerides post
meal increases in triglycerides.
And so again getting back to what I originally said, it’s important to view. Food
within the context of what it’s consumed as well and how they interact with each
other, I think is an often ignored part of the whole equation as well.
[00:21:12] Melissa: Yes. Great point. And we do tend to talk about nutrients,
and even if we’re talking about a specific food and we’re going to get into this
with a glycemic index in a little bit, but, yeah.
What about the diet, the diet pattern, and, and I’m sure I know that there’s
limitations and research to study all of this, but the closer we can get to what
happens in real life, the more applicable the results and outcomes can be. So
you’re both carbohydrate experts and part of the Scientific Advisory Council of
the Quality Carbohydrate Coalition
So I’d love to hear each of you tell a little bit more about this work that you’re
doing.[00:21:50] Sid: I got involved primarily as a physiologist to sort of help parse
the data in terms of the body’s physiological responses in the post-meal period.
Following the consumption of different nutrients in this case, it was
carbohydrate.
And one of the things that we’ve noticed across the board as someone that’s
been running clinical trials that have looked at acute studies with the food and
diet per se, is that you see substantial heterogeneity in responses to foods. And
when you see these largely heterogeneous responses, it becomes really difficult
then to go back and look at markers, for example the glycemic index, which are
sort of almost sold as being written in stone, but then when you start examining
them in physiological context, you see that they’ve got such huge variability.
That’s obviously a problem when you started talking about that. And that’s part
of the reason why I got involved in this process.
[00:22:48] Melissa: Interesting. You said the word heterogeneity and I’ll admit
like, this is kind of a newer word for me in the last year or so. So that just means
like there’s a lot of variety and a lot of variability, right?
It’s a
[00:23:02] Sid: huge variability in people’s responses to carbohydrate
consumption. The thing to understand here is that. To some extent, these
responses are driven by food you consume, but on the flip side, these responses
are also driven by things such as your age, your genetics, which is your family
history, whether you exercise or not and so on.
And so there are these markers that are thought to be driven primarily by the
food that you consume. But in reality, what you find out is that it is a massive
interaction between the food, the person and the environment, and it makes
drawing conclusions from these sorts of markers, particularly difficult.
[00:23:48] Melissa: Excellent. Thank you. Yes. And of course we see this with
patients all the time. One person can have white rice and they’re fine. The other
person, they might need to switch over to the brown rice and then they’re fine.
So that’s really interesting. Julie, was there anything you wanted to add
[00:24:03] Julie: to that?
Yeah, well, I started the scientific advisory council was really outshoot from a
group of scientists were called to talk about carbohydrate quality. After there was an international paper, said there was a consensus. On carbohydrate quality.
And the consensus was that glycemic index define carbohydrate quality.
But the problem with the consensus is that it was a little, like what I call the
coalition of the willing in that they only invited scientists who were in favor of
the glycemic index. So it was their consensus, but it wasn’t a universal
consensus. And so we, it really bothered us that if the glycemic index is an
indication of carbohydrate quality, that a Mars bar would get a good score and a
whole grain bread or a potato will get a terrible score.
Yeah. And so there were a number of reasons why we thought this was just
wrong. And then that led to the current council, which has more scientists on it.
And we’re trying to put together. An algorithm, which will help consumers
decide what is a quality carbohydrate, and it will be based on what nutrients
does it deliver, what fiber does it deliver?
Is it a whole grain or not all kinds of characteristics, not just one simple variable
measure, which is the glycemic response. And so we know that rice is important
in Asian and Latin American cultures. We know that these carbohydrates really
are meaningful. And so we wanted to also look at various diets and cultural
eating patterns so that when we make a nutrition recommendation, it can fit for
all different kinds of individuals and their traditions.
[00:26:02] Melissa: Yeah, absolutely. Absolutely. And we’re going to talk more
about that and I, I really appreciate. The cultural inclusivity aspect. It’s just so
important for just real world, real life, real people. And then application. Yeah, I
[00:26:16] Sid: was going to say just a quick little add on to what Julie was
saying is that there’s a really high prevalence of binary thinking that goes on
when it comes to nutrition.
And I think that that is something we really, we really, as a field sort of need to
step away from. And to some extent is not particularly helpful. And more
importantly, as we’ve talked about with this variability, that really creates
problems. And so when we talk about the generation of this algorithm, as Julie
was indicating we go beyond just the usual suspects, but looking at things like
whole grain intake looking at fiber content and so on, the goal is there to
holistic view.
What makes a quality carbohydrate rather than it being based off Just one [00:27:05] Melissa: thing. Right. Thank you. Yeah. So before we talk a little bit
more about glycemic index, I would like to focus more on what you’re saying
here, about how we know that the carbohydrate category is diverse and this
work that you’re doing on the scientific advisory council is hopefully going to
help us understand that or how to choose quality carbohydrate containing foods
and what they are.
So, can you share how the nutrition science community currently defines
carbohydrate quality? We have alluded to it here and there, but I want to make
sure that we don’t miss anything important with where things are right now with
the current definition
[00:27:44] Julie: or two things. We already talked about that some people
believe it is the glycemic index, which is problematic for many reasons.
In that, for instance, the Sydney glycemic index table, the university of Sydney
in Australia has 117 different. Glycemic indices for different kinds of white
rights based on its variety, based on the amount of amylose, which is a
resistance starch based on not even just whether it’s white or brown, this is just
white rice, how much water it was cooked with how long it was cooked.
And so most people using a glycemic index table, it’s really, really a dartboard,
whether the value that you picked had anything to do with what you ate. And
then if I buttered the bread, the glycemic index goes way down. In fact, most
people don’t even know that the glycemic index is based on 50 grams of
available carbohydrate.
What that means is that to get 50 grams of available carbohydrate. A refined,
enriched white bread. You need about three slices to get 50 grams of available
carbohydrate from whole grain bread. You need almost four slices because of
the fiber present in the bread. That carbohydrate is not available. So you look at
the table and whole grain bread and white bread have a very similar glycemic
index, but the amount eaten is different to get the 50 grams of available
carbohydrate.
Most. People do not understand that. And that’s the reason the Mars bar, it’s a
little tiny Mars bar compared to almost four slices of whole grain bread having
it makes no sense in a way, so that’s one problem with it. It’s way too simplistic.
And it even on the same person, the variability, when we do just a single
standard food within a person is great, much less among people.
And so that’s really, really problematic, Before we talk a little bit more about glycemic index, I do want to make sure
that we cover where the scientific dialogue around carbohydrate quality is right
now, because I know that we’ve touched on a few things, but what is this current
conversation including and not including
[00:31:27] Sid: and keep in mind is that the current science, the conversation is
largely being driven by a fair amount of epidemiological research, which is fine
as a hypothesis building enterprise.
But it’s also important to recognize that that’s the first step in developing the
hierarchy of science and the hierarchy of evidence, which eventually the highest
level of evidence would be the randomized control trial or a clinical trial. And
so what you have is fairly lower quality evidence that’s coming through.
From these epidemiological studies. The other thing also to keep in mind is, as
I’ve alluded to previously, is that foods are, or nutrients are not consumed in
isolation. They’re consumed as parts of a larger meal and that complicates
things considerably. And so a lot of this reductive conversation around single
nutrients or single indices really ignores that.
And I think causes a lot of confusion from the perspectives of a patient or a
consumer.
[00:32:30] Julie: Absolutely. Another problem is that much of the
epidemiological research is done with some kind of food intake data, often a
food frequency, which asks you how many times did you eat broccoli this
week? Or how many times did you eat potatoes this week?
Well, first of all, we’re not very good at actually remembering that and data
show that we eat more broccoli and drink less gin than we actually do . We do
that on a food frequency, but in addition, the food frequency might just say
white bread. I already told you that there are hundreds of different glycemic
indexes for different kinds of white bread.
So the number that is used in some of this epidemiological research can be very
flawed because it doesn’t tell you how it was cooked. And as Sid mentioned,
what’s eaten with it. So that’s a really big problem.
So, I mean, I, I’ve already mentioned this as a certified diabetes educator and
working with carbohydrates all the time, I find the glycemic index confusing for
patients and just generally not helpful.So I never really used it. I didn’t feel that it had real life applications. When you
talk about glycemic index, even versus glycemic load, you’ve said quite a bit
about glycemic index, but I wanted to know if there’s anything else that you
wanted to point out regarding the limitations of it.
And maybe specifically regarding potatoes and how we don’t consume potatoes
just by themselves. They’re not bananas. We don’t just sit there and eat a potato.
So what else would you like to add regarding the glycemic index?
Julie: It may be useful in a laboratory setting. It’s applicability to a person eating
a meal may be very limited.
I absolutely
[00:35:12] Sid: agree. In fact, one of the issues with, with the way in which we
assess GI is if you look at the standards that are used to establish the glycemic
index of a food.
You take only about 10 people, you feed them a portion of the food would
contain 50 grams of digestible carbohydrate. You measure the glucose area
under the curve and they didn’t give them a reference code, which is the glucose
or white bread. And that’s how you get the glycemic index. This is a really
limited sample when you do things like that.
The interesting thing is what happens when you then try and extrapolate this to
really large population. So know, in 2015, there was this really excellent study
in which they had about 800 people in whom they said about 47,000 different
meals. They essentially looked to see what was going on with glycemic
responses in these individuals, when you look at the data there, I think it is very
telling.
And the reason why I say that is because if you just look at the variability of
glycemic responses to things like glucose and bread, you had almost a five fold
variation between the one on 10th and the top 10%. So imagine if you had a
literal yard stick, but that yard stick, depending on the person that’s using it was
either one yard or five yards you would look and say, well, that’s not a
particularly useful yard stick now, is it?
But that’s part of the problem. And when you use something like GI, that’s
really tricky and [00:36:47] Melissa: I’m not the only health professional who seems to feel that
the glycemic index is confusing. There was a national survey in 2020 among
registered dietitians nearly 800 nutrition professionals that found nearly three
quarters do not use the glycemic index when counseling patients.
And three out of five, believe that the glycemic index is actually stopping
people from eating perfectly healthy foods. So I’m not alone, I guess, in that
opinion. We’re not trying to bash the glycemic index here, but we, we really
need to look at this more holistically. So we’ve talked about the problem and the
challenge and some of the ideas about how this conversation can, can be more
meaningful and holistic.
Is there anything else you wanted to say before We really kind of start sharing
some of the, the vision and the recommendations and the ideas moving
[00:37:42] Julie: forward? I just the result of one meta analysis, which looked
at really a large number of clinical trials and almost 5,000 adults. And there was
no consistent benefit of changing the glycemic index of a diet, even in a
randomized clinical trial in this large meta analysis.
So I think that shows that the. Randomized clinical trial, which is the gold
standard as Sid mentioned, kind of says that what we’re seeing in the
epidemiological study may be more about what was in the diets that were low
glycemic rather than the glycemic index itself. It may have to do with the
characteristics of the individual and the data quality of many of the epi studies,
which is probably the reasons that a lot of dietitians don’t use it is ranked low to
very low, only in the case of lowering hemoglobin A1C, and a couple other
glucose measures in an umbrella review.
Was given a moderate Quality, but mostly it’s the data quality when it’s graded
is very, very low, because there is so much variability that
[00:38:59] Melissa: makes sense. I’m
[00:39:00] Sid: not trying to bash epidemiological research, but one of the
things to keep in mind when you’re looking at nutrition epidemiology and Julie
alluded to this previously is that a lot of this is done based on food-based
recalls.
And these are memory-based. The problem is when you actually look at the
values you get out of these sort of instruments, you don’t get particularly useful
numbers and you get incredibly high degrees of variability. In fact studies have shown that when you look at nutrition recall information say from NHANES,
which is a national health and nutrition examination survey close to almost half
of the food recall information specifically with regard to caloric intake
Was compatible with someone that might be comatose, but definitely not
compatible with someone that’s leading a vertical, upright existence. And that’s
a big problem. And when you look at under and over reporting, almost three
fifths of the data are really, really problematic. And so when you look at these
epidemiological studies, just recognize that these are meant to generate
hypotheses that really should be tested in clinical trials, but you had to be really
careful drawing strong conclusions from epidemiological basis.
[00:40:18] Melissa: No, thank you for sharing that. We talk about that a lot on
the podcast the limitations inherent in nutrition research. How not everything
can be a randomized control trial and the role of epi studies. So I appreciate you
lending that perspective and reminder for us. because the outputs or the
outcomes are only as good as the inputs.
And like you said, a lot of variability there and of course just human nature,
memory issues with not being able to be very accurate with that. So thank you
for sharing that. I just like
[00:40:49] Julie: to add that there are some kinds of things. Glycemic index
categorizes as ones we should not choose.
When you do the epi studies, which we’ve just talked about, whole grains
lowers the risk of most diseases in episodic. But what is not reported is that
refined grains are neutral. So while they’re not as good in terms, they don’t
lower, it doesn’t make them bad. Like some people say, and I think potato
suffered from that a little bit too, and they don’t recognize that a potato is an
excellent source of vitamin C and has more potassium than a banana.
And these kinds of things get lost. When we talk about picking a food by its
glycemic response, and then it really, really depends on whether you eat it with
fat, which many people do an interesting study for you. And as a diabetes
educator is that you got a better overnight glycemic response.
Choosing a high glycemic index potato dish than a low-glycemic index, possum
Matti rice. These kinds of things are important to know. And for dietitians to
know, because that overnight change in glucose for diabetics must be managed
to have a successful person who is a very strict diabetic. [00:42:43] Melissa: I’ll just add to that.
When I worked in a high-risk OB clinic, I was shocked to find that it’s a pretty
unique population, whether it’s gestational diabetes or pregnant women with
type two or type one diabetes. But especially with gestational diabetes patients,
we found, and we encouraged the pregnant women to consume a half a cup of
ice cream, like regular ice cream.
At bedtime snack because that perfect mix of carbs and fat helped delay their
blood glucose rise. And we saw much better fasting glucose in the morningSo
we’ve talked about how there is a lack of a standardized definition for quality
carbohydrates and the glycemic index is flawed or very flawed, but I’d like to
hear your perspective in terms of how to best define quality carbohydrates and
what is the work that you’re currently doing in this area to define quality
carbohydrates.
[00:43:59] Julie: They were concerned that foods that are important on people’s
tables that are culturally important and have nourished us for millennia we’re
being not considered as quality. We realize that there are products, many
carbohydrates, snacks, and desserts that should be eaten infrequently, but we
really wanted to be able to define what is a quality carbohydrate food.
And we decided that there needed to be at least 40% of the energy coming from.
Carbohydrate and that it was a solid food, partly because we know most people
know that sugar sweetened beverages are not a quality carbohydrate. They also
know that broccoli while it has a little carbohydrate is a quality food.
So we only wanted to focus on those foods. We’re solid foods and delivered a
significant part of their energy from carbohydrates. And that would be things
that often were, as you called them starchy, they would be potatoes, pastas, rices
breads and cereals. And then. What do we think is important here?
And we know that people who eat for instance, breakfast cereals have a better
nutritional profile than people who don’t eat ready to eat breakfast cereals.
Bring, how can we capture the nutrients and the fiber that potato brings?
And so we try to set up an algorithm that looked at the nutrients, the fiber, those
things that would really give quality, things that we gave negative scores to
were the added sugar or added salt so that people could evaluate, well, yes, a
cereal may have added sugar.It may have added salt, but when you look at the entire score, is it something
that could rank as quality? And we’re finding that a number of foods can have
some sugar and some salt and still be considered a quality carbohydrate. And so
that’s what we’re trying to do, and to look at other kinds of tubers and things that
are used in a variety of cultures and have always been basic staples in that
culture.
That sounds
[00:46:35] Melissa: like it makes a lot of sense. Yeah. And
[00:46:39] Sid: just to add to what Julie said, one of the main things there was
to make sure we considered all the other things that went into these
carbohydrate containing foods, fiber, food processing, and so on, because these
relate to physiological responses to meals.
They relate to biomarkers such as lipids, blood glucose, insulin, and so on blood
pressure, which are related to long-term cardio-metabolic risk. And so that
nutrient density that Julie alluded to was particularly important because it can
make a mark on these biomarkers, which can then alter a health in the long run
as well.
And that’s another reason for having a more extensive definition of what
constitutes a quality carbohydrate.
[00:47:26] Julie: We were even looking at things like phytochemicals and were,
were they considered a whole grain or a vegetable because those things would
be coming in with the nutrients. So we tried to really look at this in a very
globally.
[00:47:39] Melissa: Right. It’s like its nutrient density 2.0, like there’s even
more that you’re considering such as what the cultural and everything that that’s
going into this. Oh, by the
[00:47:48] Julie: way, protein and fat have degrees of quality already defined
and we talk about fats and that we want fats that are unsaturated or we want fats
that have omega-threes in them.
And so we’ve had some degree of differentiation on what we want the fat to
have, and we haven’t really done that in a organized way with carbohydrate. [00:48:11] Melissa: Right. That’s a really good point. And we have something
similar with, with protein as well, but we don’t have that with carbohydrate. So
let’s talk about any insights you can share about future nutrition science on
carbohydrate quality that we should be on the lookout for as we wrap up, I’ve
got some, some takeaway questions for you.
[00:48:30] Julie: I think Sid early on mentioned the dash diet. We know that
there are people who abuse carbohydrates. They eat more than the
recommended amount for the degree of calories. This contributes to problems
that can occur because of too many calories, but I think the carbs are being
blamed for it. So I think one of the things that people need to think about is that
when we’re looking at carbohydrate quality, we need to look at it is it’s role in
the.
Are people eating the right amount of those carbohydrates as part of the other
important balance components of the diet are too many servings of a
carbohydrate easing out or squeezing out the important fruits and vegetables so
that we can actually want to make sure that the carbohydrates that they’re
choosing are ones that deliver the nutrients and then help consumers choose the
right number of those in a day so that they are balancing it with the other foods
that they need.
[00:49:34] Sid: So we’re engaged in this long-term iterative process in terms of
developing this algorithm. And so we only published one manuscript on that,
which provided some rationale as to why we were trying to develop a new
algorithm for defining carbohydrate quality. We’re now in the process of
developing that algorithm, and as we’ve mentioned before, it takes a much more
expansive view of carbohydrate containing foods.
And I think our followup is going to be to use the algorithm that is generated
and apply in a different dietary patterns across cultures, potentially look at
health effects and so on and try to figure out how their turns out. So this is going
to be an ongoing process. We’re probably not going to get the right answer right
away, but hopefully it’s a step in the right
[00:50:21] Melissa: direction.
And I like that you’re bringing multiple parties to the table to kind of have this
brain trust. It’s not a simple answer. It’s complex. See, I did that. Did not mean
to do that. So as we’re wrapping up, I have a few questions about takeaways. So
what would you like the research community to take away from the science
around carbohydrates today?Sid maybe we’ll start with you.
[00:50:47] Sid: Well, I would primarily say it’s just that when you’re looking at
carbohydrates, avoid reductive binary thinking it depends on context. It depends
on the foods that you pair them with. It depends on you in a lot of ways, far too
often, the, that aspect is ignored just to use a really simple example.
A lot of people get hung up on the issue of carbohydrates and body, weight or
obesity. But what we know from about three or four decades of obesity
physiology research is that the majority of the variance in body weight comes
from genetics. In fact, the heritability of body weight is equivalent to that of
height.
So when we spend so much time talking about this one macronutrient and its
association with obesity, we are literally ignoring the forest for the trees,
ignoring the elephant in the room and going for a small potatoes. And I don’t
think it’s particularly helpful from a scientific perspective, not to say that don’t
do research, but I think it would be really careful when we present this research.
And specifically in the way that we talk about it to the consumer or patients or
[00:52:00] Melissa: Excellent. Thank you for sharing that.
[00:52:02] Julie: Well, I would like to see some of the epidemiological studies
redone. I would like them to look at the recommended carbohydrate ratio, First
of all, look at, are they eating the recommended number of servings?
Is that part of the problem and look at that in relationship to the fruits and
vegetables and things that are recommended. So I think we are labeling
carbohydrate as bad just as we believed Fat is bad in the hopes we would solve
our problems. I think that’s a dangerous strategy. I think we need to look at it
more in the amount of carbohydrate compared to the amount of other fruits and
vegetables, the amount of carbohydrate compared to the amount so that we’re
looking at more a pattern.
I really like to see a study I would like the grain data to have four buckets
instead of whole grains versus refined grains. I would like whole grain staple
foods recommended. Whole grain indulgent foods of which there are almost
none or were almost none when these studies were done.There are a few now refined grains recommended foods and refined grain
indulgent foods, because I think that will give a different perspective on what
we think of refined grains, because half the calories and half the foods, when we
look at those data in the refined grain category are non-recommended.
So what we’re saying is that those who eat the non-recommended foods have,
are at higher risk. And that’s what I’d really like people to look at in terms of, for
the research.
[00:53:48] Melissa: Thank you. And for our listeners, that was a big takeaway
from episode 94, that Julie explains in detail that the doodles, ding, dongs and
donuts were lumped into.
All refined grains and that has to influence the outcome. Or at least you need to
know that when you’re looking at what the outcomes are. So along those lines,
what advice would each of you share about how healthcare professionals can
provide nutrition, education to patients and clients about carbohydrates and
carbohydrate foods like potatoes?
My
[00:54:27] Julie: go-to paper is that Seidelmann paper where those people who
ate half their calories as carbohydrates, and let’s make those carbohydrates,
potatoes and whole grain breads and enriched, refined grains in the right amount
and legumes when they eat those as 50% of their calories. They lived longer
than people who did anything else.
And I think that we really need to really concentrate that we are supposed to eat
carbohydrates and we didn’t, as the paleo people say, we did evolve to eat
carbohydrates and there’s cave evidence that we did. And so if we look at diets
over time, carbohydrates are very important and they’re very popular.
So I just think we need. Tell consumers that it’s okay to eat carbohydrates. If
you, you need to count them if you have diabetes, but you need to include them
because they do important things for your diet.
[00:55:31] Sid
[00:55:36] Melissa: Okay, great. And, and this is pretty similar, so I’m not sure
if there would be a different answer to this, but just in general, how can we as a
nutrition community, make sure that consumers know which carbohydrate containing foods are the most nutritious in the highest quality. And that’s the
work that you’re doing now, but any advice there
[00:55:56] Sid: that’s sort of TBD,
[00:55:58] Julie: okay.
The short answer is what are the things The dietary guidelines committee say
that we’re missing. We don’t get enough fiber. And we get over half of our fiber
in the diet from grains and potatoes. What are we getting enough of potassium?
A potato is a good source of potassium, better than the well-known banana.
So to really think how do we address the dietary disparities that we have? We
can do it with inexpensive foods that people really enjoy. And so we, I think
need to like reframe that this isn’t a bad food. It’s one we need to include and we
need to include it in the right amount.
[00:56:45] Melissa: Absolutely. Thank you.
And then one more nuance to that. Cause I talk about sensational headlines and
how they’re not the bottom line takeaways that people really need to make
meaningful changes in their diets. So whether you’re a health professional or a
consumer, how can we look past some of these headlines and dig a little deeper
when we’re trying to figure out this nutrition science or this nutrition research
information
[00:57:13] Sid: always read the primary source.
One of the biggest problems when you’re talking about nutrition research or for
that matter, actually that the reporting of science far too often, it’s heavily
sensationalized. It’s not uncommon to read an article that says drinking a glass
of red wine. It’s just like exercise. And then you, there was actually an article
that came out years ago about that, but then when you read it, it was in mice,
the, the reserveratrol was the equivalent of drinking, 12 bottles of wine a day.
The problem is that far too often, people are looking for a macronutrient or
micronutrient of the day, which is going to quote unquote, change your life or
save your life, or what have you. And real life real physiology is a lot more
complex than that. And anytime you see a headline that essentially says that
pause, read the primary source and more often than not, what you’re going to
find is that the primary source doesn’t quite support the breathless claims that
are made in the, in the news report.[00:58:15] Melissa: Thank you. I appreciate how he put all that. I love asking
my guests these questions because you get a unique answer with consensus. It’s.
It’s interesting. Julie, anything to add about those pesky
[00:58:26] Julie: headlines? Everyone can’t always have access the primary
source. Just some simple things to be wary of.
Epidemiological data shows association. It is frequently in headlines and in
articles as causation, no, that it’s an association. The sale of, of running shoes is
associated with the rise of obesity. And we know that silly, but both of them
happened to climb at the same time. That’s what an association is. They just
happen to vary together.
So look for that. We know that nutrition like any science is evolutionary, not
revolutionary. So if something completely sounds like it doesn’t fit the rest of
the data, be very careful to evaluate that and try to find other sources. And try to
look for sources that are quality sources, ask your dietitian because she or he
will be able to help
[00:59:32] Melissa: you touched on two or three of the points that I like to
make.
And one study is not going to change the existing body of evidence. And you
talk about the association as, so the way I like to explain that is the association
is a correlation. It’s not that cause and effect you use the example of running
shoes and obesity. And this is one that I like to use is that sales of ice cream or
ice cream consumption and drownings both go up in the summertime in warm
weather.
But certainly that’s an association that is not a cause and effect. That would be
terrible if it was up, but there’s a third variable, the warm weather that impacts
both of those. So that’s something that I like to share when I do my media
trainings with health professionals or to encourage them like this is a simple
example or analogy that you can share with your patients.
So thank you both for weighing in on the pesky headlines, where can people go
for more information related to the latest science on quality carbohydrates? Is
there a website that
[01:00:32] Julie: you can share? APRE is a good site. The Alliance for potato
research and education, and [01:00:38] Melissa: that’s apre APR e.org,
[01:00:41] Julie: right? And the grains food foundation will have articles about
a whole grains and refined grains.
Those are just a couple of a number of websites and I can get you more if you
want. Thank
[01:00:53] Melissa: you, Julie, Oh and of course there’s the Potato Goodness
website – PotatoGoodness.com – Potatoes USA’s main resource for health
professionals. There’s recipes, nutrition information, you can sign up for their
newsletter and there’s a professionals section with materials, research, handouts
and news so I’ll be sure to have these links and other resources in my shownotes
at soundbitesrd.com. And also Sid, you mentioned the first manuscript that is
published in nutrients.
And I have a link to that as well as some other articles from the apre site. And I
also have some related episodes. In addition to episode 94, with Dr. Julie Miller
Jones. I have several grain related episodes some related to diabetes. And I
recently did an episode on processed foods. And Julie, when you mentioned that
interesting example with oatmeal, how the quick oatmeal versus the steel cut
and what was the other one that the old fashioned oatmeal, that’s an example of
a benefit of processing.
So I encourage people to listen to that episode as well.
[01:01:49] Sid: The resource that you might want to add is my former
colleague, Glenn Gaesser, Julie, and I wrote another paper which looked at the
relationship between. Glycemic index and body weight. That might be
something that your listeners might go in and take a look at.
And I’ll send you the link to the paper as well.
[01:02:07] Melissa: Sid, I actually had Glenn on the show a couple of times, so
it might be something that we’ve touched on, but I definitely want to add that to
the show notes.
[01:02:15] Julie: And they also might be interested in the university of Sydney
international glycemic index table.
And the reason that people might be interested is that it points out so
dramatically that if you boil the rice for 12 minutes versus 10 minutes if they, you get a different amount that basmati rice is tend to be lower glycemic index,
but there’s some that aren’t converted or parboiled rice tend to be lower, but
there’s some that aren’t.
And so I think that really points out quite dramatically, how variable this index
is and why using it for advising consumers is really, really, yeah. So not
[01:03:02] Melissa: a resource to use, but a resource to illustrate the point that,
that we’ve been making. Thank you both so much for coming on the show and
talking all things carbohydrate.
I have learned so much and I hope my listeners have as well. It’s been an
absolute pleasure. Thank you again for your time. Thanks
[01:03:18] Julie: for having always a pleasure and may be happy to talk about
fiber and resistant starch sometime. Yeah, we’ll have
[01:03:25] Melissa: to have you back on for sure. And for everybody listening
as always enjoy your food with health in mind and a side of potatoes till next
time.
So as you’re talking and you’re the physiologist kind of a random site, What do
you think about fasting cardio? Is that something that you think is
Sid: The interesting thing is for some reason, and I don’t know why it’s gotten
popular, but the important thing to recognize is that when you’re fast, really
what you’re doing is your hepatic, glycogen is depleting or close to depleted, but
you still have plenty of carbohydrates stored in your muscle, which is then
going to get used up when you exercise.
And so if you track people as they exercise, even after they come in from an
overnight quote, unquote fast, you can make them exercise at a higher intensity,
their respiratory exchange ratio. Right away and they’re oxidizing
carbohydrates. So for this idea that somehow this is going to allow you to burn
more fat and controlling your body weight in some way, shape or form more so
than another form of exercise.
It’s probably not
Melissa: true. Okay. Thank you for that little side conversation. I appreciate
that.
LISTEN, LEARN AND EARN
Listen to select Sound Bites Podcasts and earn free CEU credits approved by the Commission on Dietetic Registration (CDR) for registered dietitian nutritionists and dietetic technicians, registered. Get started!
Get Melissa’s Sound Science Toolkit here!
Partnerships:
Sound Bites is partnering with the Association of Diabetes Care and Education Specialists (formerly the American Association of Diabetes Educators)! Stay tuned for updates on the podcast, blog and newsletter!
Sound Bites is partnering with the International Food Information Council! Stay tuned for updates on the podcast, blog and newsletter!
Diana Malkin-Washeim, PhD, MPH, RDN, CDCES, CD-Non June 1, 2022 at 1:50 pm
Melissa,
This was an exceptional pod-cast! Both speakers spoke to the value of cultural inclusivity, that is significant and I really valued Dr. Sid’s point regarding the “binary thinking” about carbs (me included). I forwarded this episode onto my staff and will forward to others. I also did not know there were 5 different forms of resistant starch – interesting. Good job!
This podcast was outstanding, I was fortunate enough to actually have Julie as a professor at St. Kates. She is an amazing professional and all of this content will be used and shared personally and professionally !
Thank you Melissa
Sign up for my monthly newsletter and episode eblasts so you never miss an update!
Listen on Stitcher (Android)
Install the Stitcher App
1. Search for “sound bites with melissa joy dobbins” 2. Choose Play Current Episode or Add to Playlist
Choose “Play Episode”
Subscribe & Review on iPhone
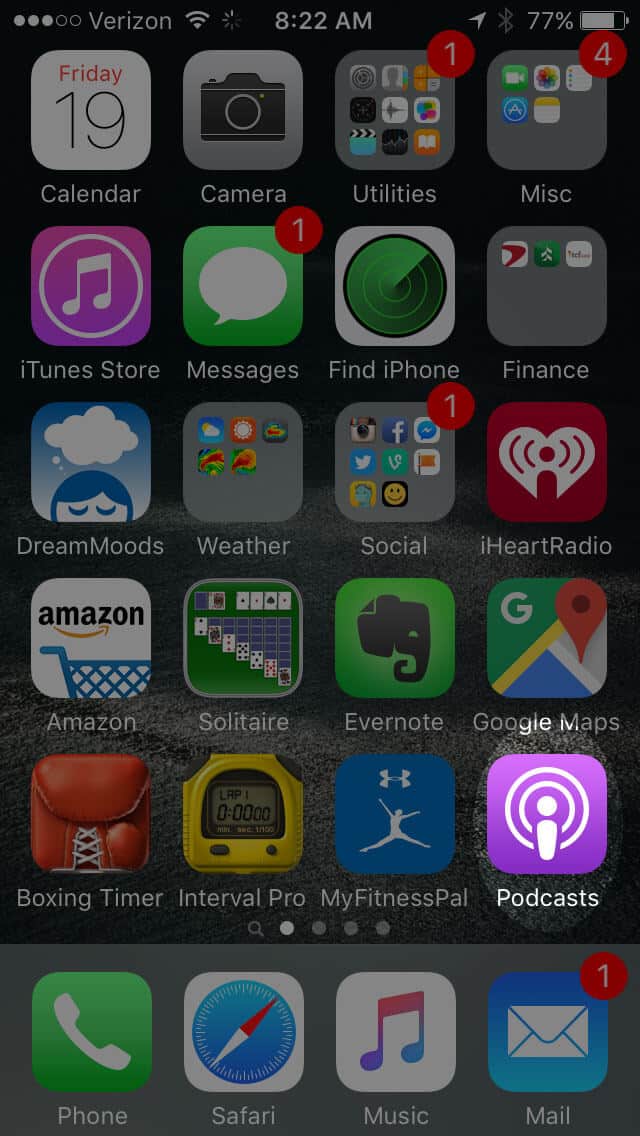
Open the “Podcast” app on your iPhone
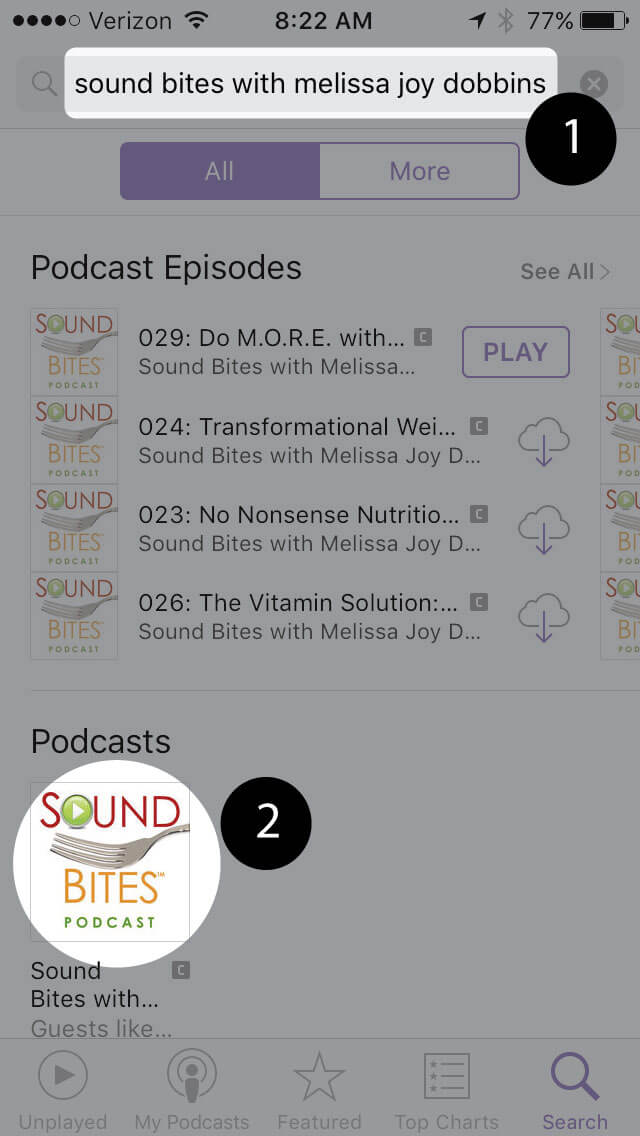
Search for “Sound bites with melissa joy dobbins”
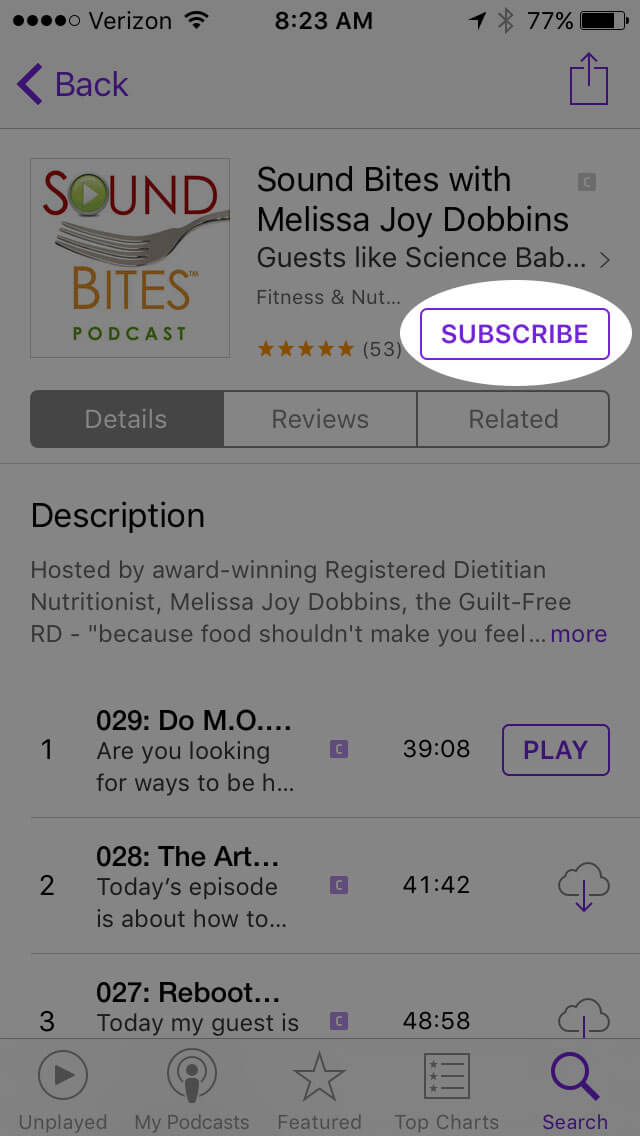
Open the podcast and click “Subscribe” and your done!
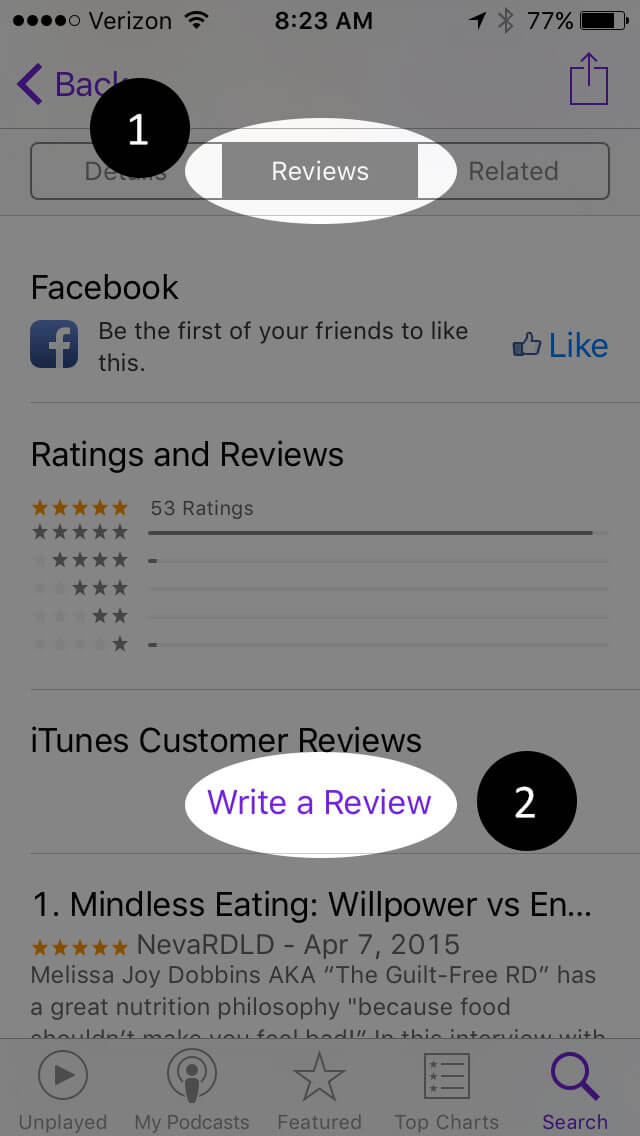
Write a Review
Click “Reviews”, then “Write a Review”.
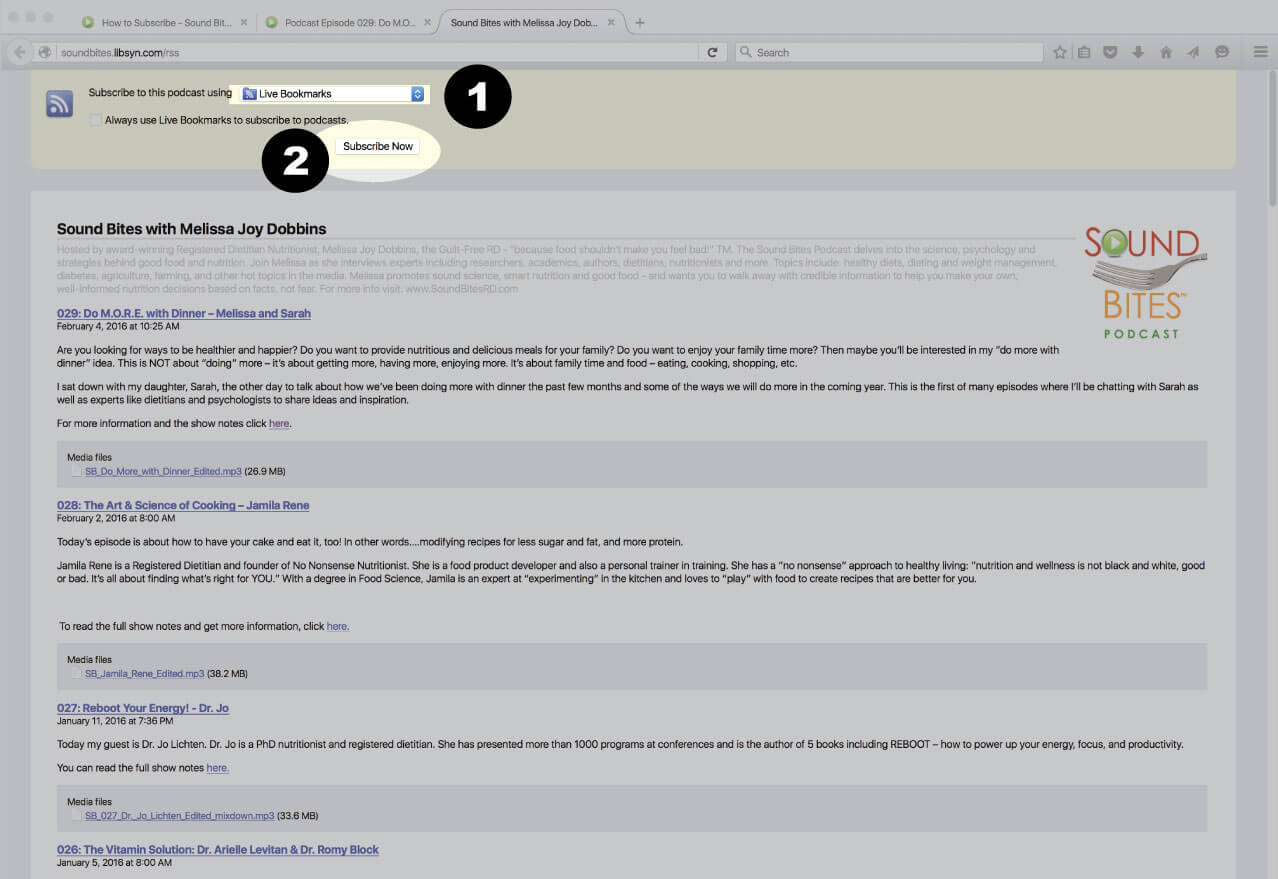
Subscribe via RSS Feed
Navigate to any podcast player . Click on the RSS feed icon.
Click on the RSS feed icon.
Click on RSS Feed
Choose which application you would like to use to receive the RSS feed
Click “Subscribe Now”
Confirm settings and subscribe.
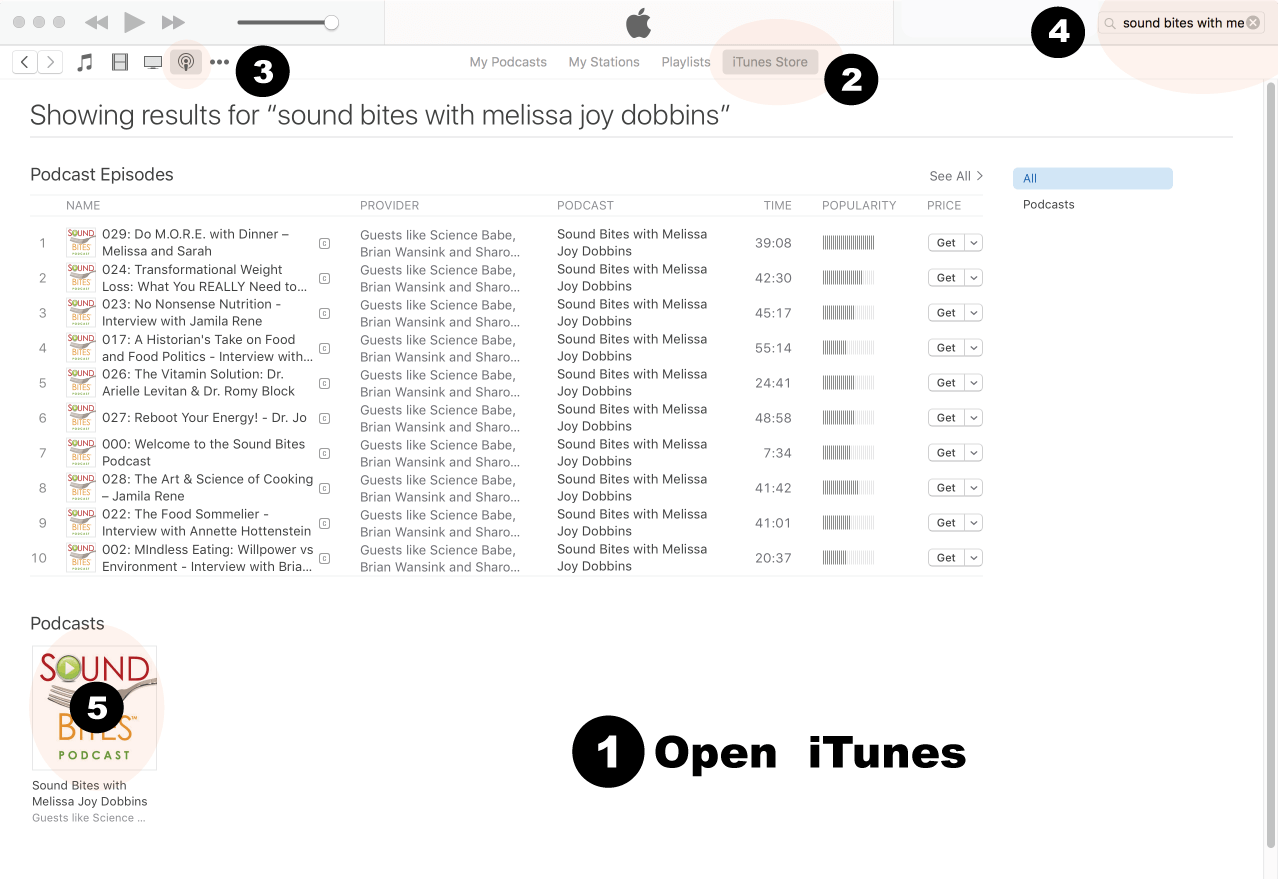
How to Review in iTunes
Open iTunes desktop application
Click iTunes Store
Click on Podcasts
Search for “Sound bites with Melissa Joy Dobbins”
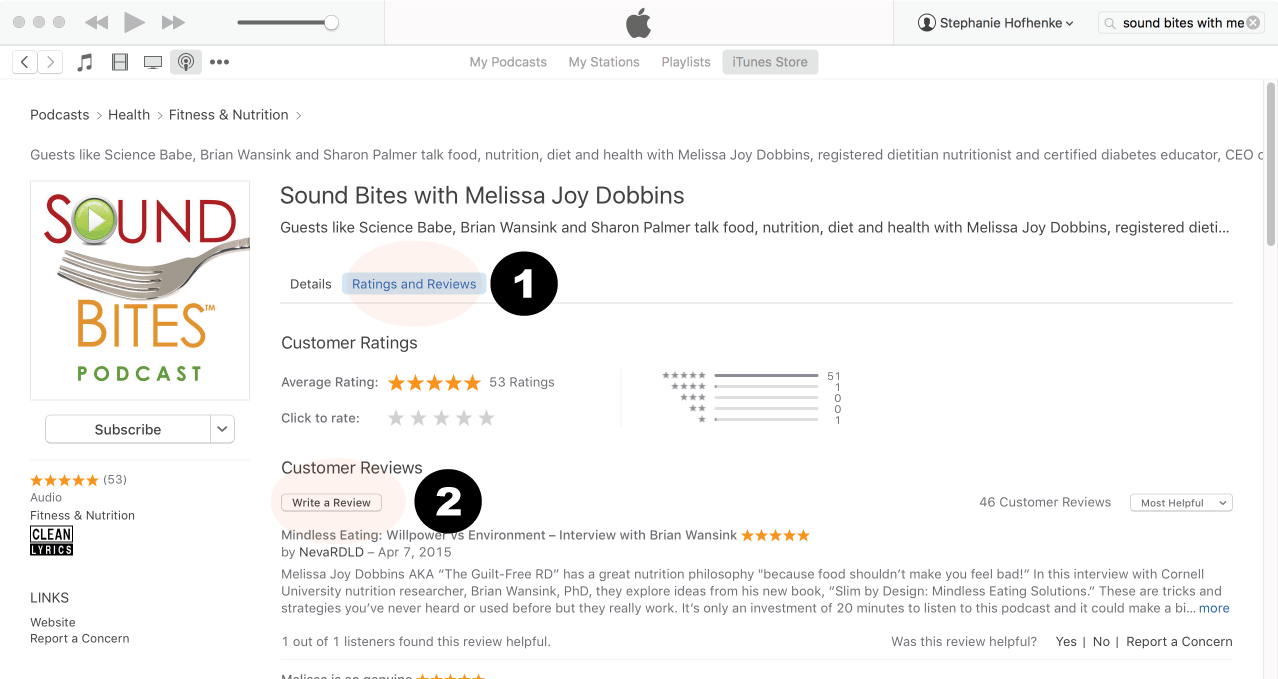
Click on podcast image
Search for Sound Bites podcast in iTunes
Click Ratings & Reivews
Click Write a Review
View reviews and write your own review.
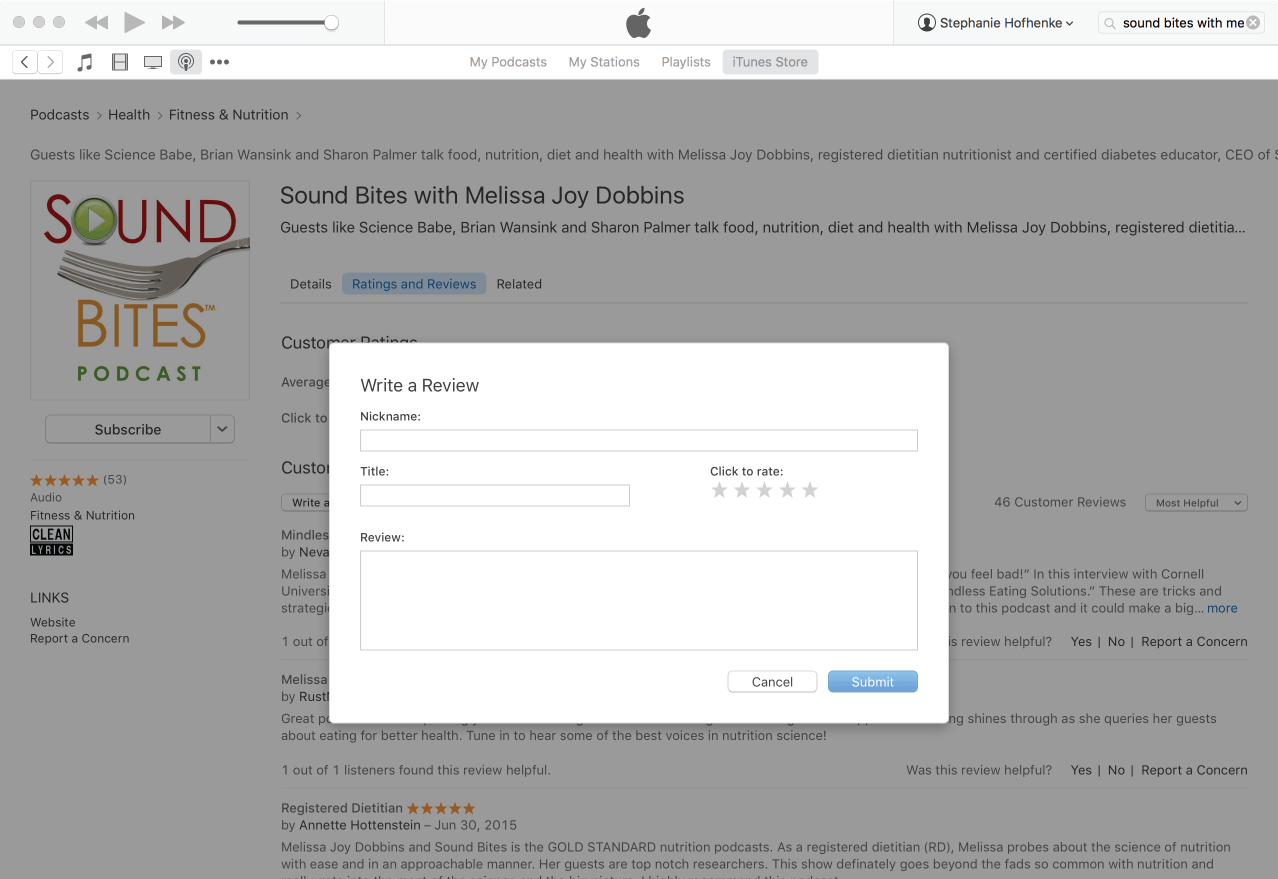
Write your review…. Thank you!
Write your review!
How to subscribe via iTunes
Click here to view the Sound Bites Podcastin iTunes, then click the blue “View in iTunes” button. This will open your iTunes application directly to Sound Bites Podcast. Click the “Subscribe” button, and your done!














Melissa,
This was an exceptional pod-cast! Both speakers spoke to the value of cultural inclusivity, that is significant and I really valued Dr. Sid’s point regarding the “binary thinking” about carbs (me included). I forwarded this episode onto my staff and will forward to others. I also did not know there were 5 different forms of resistant starch – interesting. Good job!
Diana,
Thank you so much for listening and sharing your thoughts here – I really appreciate it!
Melissa
This podcast was outstanding, I was fortunate enough to actually have Julie as a professor at St. Kates. She is an amazing professional and all of this content will be used and shared personally and professionally !
Thank you Melissa
Excellent podcast.