Celebrating over 1 Million Downloads and 50,000 Free CEUs on the Sound Bites® Podcast | NEW: Get 1 years’ worth of CEUs with the new 15-CEU Podcast Course
When you hear the words “eating disorder” most people get an image in their mind of what that means and what that “looks” like. Unfortunately, that can lead to many missed opportunities to help people. If we use different terminology, such as disordered eating or dysfunctional eating behaviors, we can appreciate the fact that anyone who eats can have problematic eating behaviors. They don’t even have to rise to the level of an eating disorder to be an issue. There’s no reason that someone couldn’t or shouldn’t get help just because they don’t meet certain criteria or fit a certain stereotype.
In addition, this approach can feed into some outdated treatment for eating disorders if the treatment is based solely on the outward symptoms. There are many different origins of disordered eating that can and should be taken into consideration during evaluation and treatment.
It is unfortunate that eating disorder nutrition is considered a specialty when really any dietitian who interacts with humans is going to encounter clients who have issues with eating.” – Jessica Setnick
Tune in to this episode to learn about:
The differences between eating disorders, disordered eating and dysfunctional eating behaviors
Jessica’s 4 “origins” of disordered eating
Food “fairytales” – how events earlier in life may still be making an impact today
A new survey of dietitians about their education and training in eating disorders and future implications for clinical practice
The pros, cons and realities of dietitians working in conjunction with therapists
Why ALL dietitians are encouraged to have some basic working knowledge of eating disorders, not just those who specialize in ED treatment
What Eating Disorder Bootcamp entails
The influence of our external environment and “diet culture”
How racism and bias is “baked” into the field of dietetics
Helpful resources and takeaways for the general public, dietitians and other healthcare professionals
Nutrition is so much more than what you eat. It’s also why you make the choices you make, how you feel about them before and after, how your early life experiences are still affecting your eating, and so much more than you might think.” – Jessica Setnick
Jessica Setnick MS, RDN, CEDRD-S
Jessica Setnick is best known to dietitians around the world as the eating disorder nutrition expert behind Eating Disorders Boot Camp and the Eating Disorders Clinical Pocket Guide. In her nearly 25 years as a dietitian, Jessica has worked in all levels of eating disorder care, all the way from solo private practice to consulting for large facilities. She shares her expertise with nutrition counselors around the world in phone and video consultations about the challenges of trying to help individuals with eating disorders in a world that isn’t helping at all.
You don’t burn a Picasso just because it’s not the Mona Lisa. You can admire both of them and think they’re both beautiful. And so it’s really about expanding our minds to accept that even if we all ate the same foods and exercised the same amount and got the same haircut, we would still all look different and that’s normal and that’s okay.” – Jessica Setnick
Special Offer! for the first time ever, Jessica is offering a Discount Code for Eating Disorders Boot Camp! Use code “SoundBites” and get $30 off this amazing program.
You can get help for your eating dilemmas. The best person to help is likely an eating disorder specialist dietitian. If you need help finding one, email Jessica’s assistant Bianca at admin@IFEDD.com with your zip code and she can tell you who’s in your area.
[00:00:00] Melissa: Hello and welcome to the sound bites podcast. Today’s
episode is about eating disorders and disordered eating or dysfunctional eating
behaviors. What they are, how to understand them and their origins better and
how to better manage and treat them. This episode is for anyone who is
interested in the topic for themselves, for a friend or a family member, or as a
healthcare professional, who wants to be a better practitioner.
Now I do want to let you know that if you have had or have any kind of
struggles with body image dieting or the like, I would like you to consider that
the topic we’re covering might not be in your best interest, if it leads to anxiety
or other triggering emotions, we are trying not to share anything too specific or
triggering today, but we aren’t able to predict how different people will react to
some of the information we discuss.
So just know that it’s important for you to do what you need to do in order to
take care of yourself. I also want to let you know that we are submitting this
episode for free continuing education credits for registered dieticians, diet
technicians, and diabetes educators. So be sure to check back at
soundbitesrd.com/freeceus for updates on all of my free continuing education
activities.
My guest today is Jessica Setnick. You may know her as the eating disorder
nutrition expert behind eating disorders bootcamp, or as the author of the eating
disorders clinical pocket guide. For nearly 25 years as a dietician, Jessica has
worked in all levels of eating disorders.
From private practice to large facilities. Welcome to the show, Jessica.
[00:01:43] Jessica: Thank you. Excited to be here,
[00:01:45] Melissa: You know, I actually interviewed you for my blog. You’ll
remember back in 2014 after we met I believe it was a dieticians in business and
communications panel that we were on together. I remember! It was a long time
ago though.
You’re very memorable! So are you! I really enjoyed connecting. And we
haven’t really, our paths haven’t crossed much since then. But that blog that I
did, where I interviewed a lot of dieticians, it turns out it was the precursor to
my podcast. That was unbeknownst to me at the time.But, you know, we just kind of got reconnected recently through a mutual friend
Neva Cochran. And I would love for you to tell us more about yourself and your
background and the work that you do. Sure.
[00:02:34] Jessica: I’d be happy to. And thanks for having me. And, you know,
I always tell Neva that technically she’s a dietician, but her real job is
connecting people.
So she did a great job this time. Always. So my path as a dietician is. Very
accidental one. I took nutrition as an elective in college because a friend told me
that it was an easy “A” which, by the way, it wasn’t. But nevertheless, taking
that nutrition class made me fall in love with nutrition, the idea of what happens
to food pnce it goes inside your body, why you make the food choices you
make, how the food gets to you in the first place.
All of it was so fascinating to me. And I was actually an anthropology major at
the time. And couldn’t quite figure out how it was going to make anthropology
into a career. But if you’re not familiar with anthropology, it’s the study of
human development on a macro scale, human cultures, human physiology.
And to me, nutrition was more of Human development on a micro scale, how
we develop throughout life, how we develop the culture of eating in our own
homes and in how we reflect the bigger culture with our eating, it was all just
amazing to me. So I changed course there and went to get a master’s degree in
nutrition.
Even though I think that the whole psychology of eating or the anthropology of
eating, or whatever you want to call it about the pieces of the puzzle, that aren’t
just the nutrition process inside your body. I felt like that should be important in
every area of nutrition and dietetics. But at the time when I was at school in the
1990s, really the only area where it was kind of kosher to talk about that stuff
was in the eating disorder field.
And so that became really my fascination, because it was where we were really
looking into those things. And it took a while for me to realize that I was
actually in recovery from my own eating disorder. I was one of those people that
sort of looks at the diagnostic criteria and says, well, it wasn’t that bad.
So I guess I didn’t really have a problem. And it took me a long time to really
accept that Yes, I had had an eating disorder. And even though I was able to get
into somewhat of a recovery without professional help, I really needed a lot ofcounseling and eventually medication to really actually get into what I consider
remission, which is not having Not as many thoughts, and definitely no
behaviors. And it just gave me such an important insight. Having gone through
that process, myself, into what I brought into the field. So my work is now
mostly educating other health professionals because I was in private practice.
As you mentioned for a lot of years, I started in the hospital in an eating
disorder program, went into private practice and then realized that there was so
little education and this is going to make me sound really, really old, but you’re
going to remember this too. But when I started working in an eating disorder,
Program at a hospital. This was sort of the Dawn of the internet. There was no
Google. There was nowhere to look things up.
And so if you needed information, you had to get in touch with another
dietician. And so for dieticians, who weren’t specializing in eating disorder, It
was really challenging because they would literally have to call information,
asked for the phone number of a different hospital call a different hospital, ask
for the nutrition department, ask if they had a dietician who specialized in eating
disorders or who could advise them if the answer was no, they’d have to hang up
the phone, call information, get the phone number for another hospital.
I mean, it was really a labor intensive process to try to find someone that could
help you. And when the Dawn of the internet, happened there was one listserv
for all of the academy. I don’t know if you remember that – it was called the
ADA at the time, but there was one lisstserv for every dietician. And so what
would happen is the dietician could look on their census in the morning, see that
there was someone with an eating disorder type into the list serve “Can anyone
help me with this patient?” And by the time they came back down for lunch
someone like me would have answered and said, Hey, give me a call. I can talk
you through it type of thing. And so through that process, I became known as an
expert in eating disorders. And so that’s really where everything in my mind
kind of began.
I don’t know if it was right place right time, but also that willingness to help a
colleague. And so over time, I was then asked to give talks on eating disorders. I
came up with my own workshop, eating disorders bootcamp. And so that aspect
of my career started to overwhelm the patient care aspect where I couldn’t be
traveling and presenting and also be there for my patients when they needed me.
So over time, I ended up closing my private practice and just doing the
education piece, which is what I do now.[00:06:57] Melissa: Okay. Excellent. Yes, I do remember all of that you know,
before the internet, before we used email at work and, and things like that I
think we’re, we’re pretty much contemporaries
[00:07:07] Jessica: there. We had email but pe printed out all the emails I don’t
know what we thought we were going to do with.
Well,
[00:07:17] Melissa: that is funny. I do remember doing that. Yeah. Or if you’re
going to a website, you would just print out the information because of course
you didn’t have a mobile device to look it up on the go. And, oh my gosh, you
know, you, you called a restaurant and got directions on how to get there. You
didn’t, you know, use Google maps or anything.
But I digress and I’ve told this story on the podcast before I think, My very first
TV segment was the first day of my second job, which was my outpatient
dietician job, which was my favorite job. I loved it. And that first day on the
job, my boss came to us at lunch and there was about 10, 12. I was the only
outpatient dietician, everybody else was inpatient.
And she said, the TV stations coming, who’s going to do the TV interview.
Everybody said, I’m not doing that. I’m not doing that. And I was mortified that
everybody was being so insubordinate. And I thought, well, I guess I’ll do it.
And it was on men’s health. And of course like, well, I didn’t know that much
about men’s health.
You know, it, wasn’t my area of expertise. But we actually called the academy
based here in Chicago. And I said, you know, I need some information and they
faxed it to me. So that was in 1995. So yes, a lot has changed since then. And
yeah, the good news is that the world has opened up in order for dieticians to be
able to connect with each other and find resources like you.
But that’s still, we’re going to get into this. That’s still a little bit of an issue.
With dieticians in our field, not necessarily, you know, specializing in eating
disorders or disordered eating and perhaps not feeling comfortable, you’re still
serving this wonderful role to help educate them and give them confidence and
insight.
So we’re going to talk about that today. So this topic, eating disorders, it can
really be taboo. Yes. It can feel very daunting. It can be anxiety provoking. Sowhere should we start? You know, keeping in mind that we have a mixed
audience, we have the general public, we have dietitians and other healthcare
practitioners.
You know, where should we start? What do we need to know to set the stage
for eating disorders and disordered eating.
[00:09:25] Jessica: Gotcha. Great question. And the place I would start is with a
term that you used in your introduction, which is dysfunctional eating
behaviors. I feel like when we say the words, eating disorders, everyone gets
sort of a persona or an avatar in their mind of what that means the same way
that I, who had had an eating disorder thought that I didn’t have an eating
disorder because I didn’t meet XYZ picture that I had in my mind of what an
eating disorder was or the diagnostic criteria.
I think all of that, we need to kind of set aside because what it has led to
unfortunately, is a lot of missed opportunities to help people. And the diagnostic
criteria, the research in our field so much is based on these biased ideas of who
gets eating disorders that really, I feel like we need to use different terminology
that sort of takes us away from that this is a very small group of people who
have these very specific behaviors and enlarge it to everyone who eats can have
dysfunctional eating behaviors. And there’s no reason that someone couldn’t or
shouldn’t get help just because they don’t meet some criteria.
So part “A” is a lot of people don’t get help because the having a problem is not
recognized by the words, eating disorders. And another part of the problem is
that sort of outdated treatment for eating disorders. We’re really kind of thinking
of eating disorders as one thing, based on the symptoms, the outward symptoms.
And we need to start looking at that idea of anyone who eats can have
dysfunctional eating behaviors. They don’t even have to rise to the level of an
eating disorder to be an issue. And so I prefer the term dysfunctional eating
behaviors because I feel like it sort of opens up this continuum of, yeah, we all
have some, and my definition of dysfunctional eating behaviors is really, you
know, does eating support your goals or not support your goals?
You can’t really define it by someone’s individual behavior. There’s things we
can all agree are detrimental to health, but for many people it’s much more
individual than that. So for example, someone might be eating a Turkeysandwich for lunch and enjoying it. It’s delicious. And someone else might be
eating a Turkey sandwich for lunch because they’re scared to eat anything else.
And so the same food can be functional or dysfunctional for two different
people, or even for the same person in different situations. And so I felt like
dysfunctional eating behaviors really opens up the window for us to look
through and our own behaviors and include things like our motive for eating and
the results of our eating and whether we feel regret after eating and things like
that can sort of point to whether our behaviors are supportive to our lives or
destructive to our lives versus the specific behaviors that we all know and
associate with eating disorders.
[00:12:00] Melissa: Okay. Very good. And yes, this term dysfunctional eating
behaviors is a phrase or a term that you came up with and shared with me. So,
so that’s why I used it. And I’m so glad that you explained that to me and to our
listeners, you know, there there’s a stereotype and a stigma and there’s
symptoms and behaviors.
And it makes perfect sense that if we have this narrow view of it, like you said,
there’s a lot of missed opportunities. People falling through the cracks, even,
even in your situation, you thought, well, I don’t look like that. And when I say,
look, I mean, in my mind, like I’m not, I don’t identify with that. So that’s not, I
don’t have any detour because that’s not what I’m seeing.
Even for ourselves, there can be missed opportunities there. Yeah. Very good.
So then let’s build on that. You know, we’ve adjusted our lens, we’ve opened up
our minds and I’ll tell you as a dietician working in the hospital setting, whether
it was inpatients or outpatients, I worked with eating disorders and I found it
very challenging.
I felt frustrated and anxious that I couldn’t, I felt that I couldn’t help my patients
better, but also kind of had this epiphany leading back to this term,
dysfunctional eating behaviors where gosh, you know, eating disorders aside,
most people that I was seeing had some disordered eating. And like you said, it
didn’t necessarily rise to the level of, you know, like a formal diagnosis or
anything.
And this is just what people were telling me. Lord knows what they weren’t
telling me. It can be a lot. So let’s build on this. Is this a good spot for us to talk
about there’s four origins.[00:13:45] Jessica: Yes, but first let me say that I am totally with you and the
statistics support what you say. I think statistics about eating disorders are very
unhelpful in many, many cases.
Because again, as I said, they’re kind of based on this very biased thinking that’s
baked into the field, but one of the things I think we can trust, or it may be even
worse than the statistic is that only about one in 10 individuals with an eating
disorder is ever going to get specialty care. So that means nine out of 10 people
with eating disorders – and we’re not even talking about dysfunctional eating –
We’re just talking about truly diagnosable eating disorders. Nine out of 10 are
going to be in your care. They’re going to be in the diabetes clinic. They’re
going to be in the oncology service. They’re going to be on the med/surg floor.
And so obviously not, everyone’s going to see a dietician, but those that do are
not very likely to see an eating disorder dietician just there’s 30 million people
with an eating disorder and less than a thousand dieticians that identify as
specializing in the eating disorder world. So yes, if you’re a dietician that doesn’t
specialize in eating disorders, that’s not gonna shield you from having patients
in your care whenever your service is that also have eating disorders.
And so, yeah, I think it’s really important to have a working knowledge of what
to do to help. And that’s why I actually came up with eating disorders bootcamp.
It wasn’t meant to be for specialists. It was meant to be for generalists or
dieticians in other areas to really help them when they encounter individuals
with eating disorders in those other areas.
So I agree. And when you look at the four different paths to eating disorders,
you can see how they can affect everyone. It’s not just this small sort of
subgroup that we’ve been led to believe. So there’s four major groupings of
paths toward eating disorders. There’s probably 30 million different paths to
eating disorders since there’s 30 million people.
Well, that’s just in the U S actually you may have listeners in other countries. So
there are millions of people with eating disorders, but I’ve tried to sort of narrow
down the origins of them into four major paths. So yes, we can go over those.
And I have a handout on this that we can put in the show notes if you’d like to.
Great! Because I’m going to say a lot of words and you won’t be able to write it
all down.
So the first grouping is the biologically based, dysfunctional eating behaviors.
And I use the word biology to describe this rather than genetic, because I think
genetic is one of those words that has very specific meanings, right. Inherited.And that’s not what I mean. Yes, there are probably some eating disorders that
are inherited, but there are also a lot of biological factors that are not inherited
that can influence an eating disorder.
A great example is concussions, right? Nothing inherited about that, but
someone could get a concussion and that can lead to the development of
dysfunctional eating behaviors because of the effects on the brain, right? It’s
traumatic brain injury. And even though it’s a closed head injury, you still have
effects on appetite effects on perception, all different kinds of things.
And so that’s just one example, other biologic behaviors or biologic factors that
affect eating behaviors are things like hyper or hypothyroidism, anything pretty
much that has a hormonal component. So any kind of diabetes, polycystic ovary
syndrome, and then you have the psychiatric illnesses like depression and
anxiety, obsessive compulsive disorder, all of these are biological conditions
that can influence eating behavior.
So it’s much more than just the genetic piece, which there probably is a genetic
piece to a lot of eating disorders, but that’s definitely not the whole picture. So
that’s type one. Type two of the path to eating disorders would be addiction
related. So there’s sort of a chicken and egg cycle that can happen with
addictions and by addictions I mean everything from substance abuse or
chemical dependency to behavior, process, addictions things like compulsive
gambling, et cetera, you have a situation where, you know, someone who’s
trying to recover from an addiction has, you know, the addiction is not to the
substance as much as to the chemical changes that the substance or the behavior
produces.
Right. And so food is a mood altering chemical. People don’t often identify it
that way, but if you’ve ever been hangry and you ate and you felt better – not as
cranky, you know, right. Food affects your mood. And so when someone is
dependent on a different substance and they’re trying to not use that substance or
abuse that substance, it can be really easy to turn to food.
You can also have a situation where someone develops an addiction because of
their dysfunctional eating behavior. So where someone turns to a certain type of
substance in order to let’s say, keep their weight down and prevent them from
eating or prevent them from having an appetite. So there’s a lot of connections
between addiction and eating and that’s another path.The third path is stress and trauma related dysfunctional eating behaviors. And
this is such a huge category. I’ll give a few examples, but basically it breaks
down into two major groups. I guess, to me, the difference between stress and
trauma is simply a traumatic event might happen one or more times.
Stress is something that could be low lying and may not even be identified as
traumatic, but it is traumatic because it occurs over time. So something like food
insecurity to me is stress that becomes a trauma because it keeps occurring over
time. And so you’ve got two major groups here. You’ve got traumatic events that
have nothing to do with food, but that are just a shock to the system.
They exceed someone’s ability to cope, probably anyone’s ability to cope. This
is things like, you know, and here’s where I hate to trigger someone, but
something like a death, a divorce, your house burning down – things that are just
so shocking that they affect your body chemistry and that can then affect all the
things I mentioned when we were talking about concussions. That can affect
your appetite. It can affect your mood. It can affect your ability to procure food
for yourself, your desire to eat. So many different things can be affected by a
single traumatic incident. And if someone has multiple traumatic incidents even
more so. Then there’s a group of stressful, traumatic incidents and events that
are related to food.
So that is something like if you were in hurricane Katrina, sitting on your roof
for three days, not knowing if anyone was going to rescue you and you had no
food. Or someone who was in a refugee situation, someone who went through
the great depression. And we’re all descended from individuals who experienced
some kind of food-related insecurity at some point.
And so we have this kind of food related trauma that then becomes even more
difficult to untangle because we have to deal with the food related rules and
thoughts and feelings that we develop based on that. And also whatever the
traumatic stressful incident was as well. So, you know, almost everyone has
something in their life that they remember or recall that happened related to
food.
For me, it’s that I ate life cereal and I threw it up and I can’t even stand to look at
the, those colorful letters of the word life. When I walk in the store, all I can
think of is how I threw it up. For my husband at the time, he had to sit overnight
with the mashed potatoes on the table that he didn’t want to eat.And he fell asleep on the table. So, you know, those are in the grand scheme of
life. It’s so easy to say, like that’s no big deal that happened so long ago that
wasn’t really that bad. It didn’t affect me, but Melissa, I’m telling you that stuff
that happens when you’re young, it really does continue to affect you throughout
life.
So we can’t just discount those things, even if they don’t rise to the level of what
the therapist call a big T trauma. They still were less than nurturing, let’s say.
And so they felt traumatic to us as children and, and can definitely be still
affecting us. So that’s a third path. And then the fourth path is, is learned
behavior.
And this is caused by the environment, by society, whatever names you want to
call it by, you know, everything from diet culture to the thin Ideal is what it used
to be called. You know, appearance culture, consumer culture. This is caused by,
you know, filters and the fact that we never see celebrities looking like humans,
we only see them all glammed up.
There’s so many factors this can come from just learned behavior in a family. I
remember seeing on TV, a woman talking about her eating disorder
development and that her whole family would eat dinner and then they would
go move into the room with the television and order pizzas. And everyone in the
family would get their own pizza to eat while they watch TV.
And this was after dinner. So, you know, to me, some of these behaviors that are
learned are not perceived as dysfunctional at the time, but if we’re still doing
them later in our lives, they may now have become dysfunctional behaviors.
Another example would be something like sort of food rules, like a lady doesn’t
eat blank or doesn’t weigh blank or, you know, different kinds of messages that
we get that, you know, the solution is not necessarily an easy solution just
because it’s not biological. It might be very difficult to untangle these messages,
but it’s important to sort of try to find the source of dysfunctional eating
behaviors because that’s going to lead to the appropriate treatment.
[00:22:38] Melissa: Right? So each of these four different types in and of
themselves there’s a variety, like you said, there’s millions of reasons. Cause
there’s millions of unique individuals. Yes. But to your point, the goal is to try to
find the right treatment for the right person. And if you’re trying to treat
somebody with addiction related behaviors.And you’re just talking about diet culture, you kind of missing the point and
vice versa. Right?
[00:23:07] Jessica: Exactly. Exactly. And I do feel like that’s the dilemma that a
lot of people who have tried to find treatment for their eating disorder have
encountered that people are grouped together based on their outward symptoms.
So here’s three people who don’t eat enough to sustain life. They’re going to get
the same treatment. Here’s three people who use compensatory behaviors after
they eat. They’re going to get the same treatment. But if you put someone who
had a concussion in a group with someone who has had food insecurity in their
life.
I’m not saying they don’t have lots of things in common, but they don’t
necessarily have the same condition. And so therein lies the story of three bears
that I often tell the three bears and Goldilocks, which is that the three bears were
all coughing and Goldilocks came along and gave them each a cough drop.
And Papa bear said, oh, thanks, Goldilocks. I feel much better. And mama bear
said in between coughs, Well, that didn’t do anything for me and baby bear,
didn’t say anything and just started turning blue and passed out and they had to
call 9 1 1. Well, they were all coughing. They all got the same treatment. Well,
Papa bear, he had a sore throat.
So a cough drop was great – solved his problem. Mama bear had tuberculosis,
so a cough drop isn’t going to do anything for her. It’s just going to cough it right
out. Probably. And baby bear was already sucking on a cough drop. And two
cough drops was just too much for his little trachea. And so he actually started
choking because it blocked his airway.
So if you don’t look at what is the root of someone’s outward behavior, then,
how do you know you’re giving them the right treatment? And unfortunately, in
a lot of cases, not all, but in a lot of cases, that’s what traditional eating disorder
treatment is. It’s, let’s look at your outward sign of behavior and then let’s give
you a treatment based on that.
And some treatment is even based on what someone weighs, which has nothing
to do with the origin of their dysfunctional eating behavior. So a lot of missed
opportunities, as we said before.[00:24:59] Melissa: And you had mentioned, just because something might
have happened to you long ago, or it might seem just a long ago, memory
doesn’t mean it’s not affecting you today.
And I can appreciate the challenge here to kind of connect all the dots. And help
people do that for themselves as well. How, you know, I remember thinking
when I was working as an outpatient dietician that, gosh, you know, I can’t, I
need a degree in psychology to help these people, or I need to work closely with
a therapist.
Where are things at with that today regarding dieticians and therapists working
together? I mean, I know like tele-health has probably helped a lot of that
because you know, just the logistics involved. Where are things at with that?
[00:25:43] Jessica: Well, there’s a big difference between our training, right?
Dieticians are trained to work in a team approach. Therapists are often trained to
work very independently. Everything is confidential. So you can’t really make a
generalization about dieticians and therapists. I think there is a group of or, you
know, many therapists who really respect and value the input of dieticians and
are really good at working together.
I know I found that when I was working, there were, you know, certain
therapists that, you know, a patient would say to us, wow, did you talk to Suzy?
Because she said the same thing, you know, where we’re really kind of sharing a
wavelength. And then there are other therapists who don’t want anything to do
with the dietician, or they are sort of one modality therapist.
They really are very strongly into whatever that modality is, whether it’s FBT or
CBTE and those modalities don’t involve dieticians. So that’s fine, but it’s not
going to be a good working relationship if a patient wants to see a dietician and
one of those therapists. So I think it just depends. As far as what is the
dietician’s role there?
You know, first of all, let me just mention that I did do a workbook called Food
Fairytales, which is about delving in on your own for someone who isn’t really
ready to talk about it with a professional to just start delving in, on your own, on
what are those childhood messages and experiences that you had.
And so we can put a link to that in the show notes and even put a discount code
for people if they’re interested. Great. As far as what is the dietician’s role versusthe therapist role? I think it’s really easy to me to say what the difference is. And
I will say, this is the number one question that dieticians always ask during
eating disorders Boot camp is how do I know that I’m not being a therapist?
And the easy answer is if you didn’t sleep, walk to school and go become a
counselor, you’re not accidentally being a therapist.
Dieticians and therapists both use counseling skills. But to me, the biggest
difference is what the topic is. So we might all use motivational interviewing or
mirroring or active listening or unpacking or all these different things
redirecting, reframing, but what makes the difference is that a therapist is using
those tools on things that are separate from what the dietician does. So the
dietician’s scope of practice is anything related to food and eating. And then
there’s, you know, some aspects of body and body size and things like that.
And then the therapist is using those exact same tools sometimes but to delve
into things like adverse childhood experiences and future dreams and
aspirations and career goals and time management and family relationships.
And it becomes really easy when you think about it that way to realize that as a
dietician, I’m only talking about family relationships as far as they relate to
someone’s food and eating. Once I realize this isn’t about food and eating, then
it’s real easy to say, you know what? I’m a good listener, but I don’t think I’m the
right person to advise you on this. Do you have a counselor? Or a best friend or
who helps support you when you have this kind of dilemma.
So it becomes really easy as a dietician to sort of you know, draw that line
gently, but for us and for the client and say, oh, you know what, this isn’t my
area of expertise. Now it might be different if you’re talking to a friend, but
when you’re talking as a dietician, your area’s really the food and nutrition
aspects.
And so it becomes really I think obvious once you get there, but sometimes you
don’t get there until you’ve gone down a bit of a rabbit hole. So I’ll give the
example of someone who let’s say is talking to a dietician about their specific
way that they like to eat. And they mentioned that they went to someone’s
wedding and that person did not accommodate their eating style and they just
felt very left out.
And so the dietician is kind of going along this conversation, thinking, okay,
we’re talking about how they manage their eating and what did they do in this
situation? But over a few minutes, you realize, wait, this is not about food andeating. This is about feeling insulted. This is about their relationship with that
person.
And when you realize that that’s when you can say, oh, you know what? I
thought we were talking about your eating, but I realized this is really more
about your relationship with that person. So I think this might be better
addressed with your counselor, and then you bring the topic back to eating. And
the easiest way to do that is to say, how did that affect your eating?
Right. We can always bring it a – almost always there’s exceptions to everything.
We can almost always bring a conversation back to food and nutrition and be
right there in our scope. And just to comfort those dietitians that worry,
sometimes I’ll say this, what a client or patient brings to you and says to you
does not make you in or out of your scope.
It’s what you say back. So if someone tells you something, that’s not really a
dietician’s area, you just simply say. Oh, you know what? That’s not really my
area. Is there someone else in your life that you could talk to about that? And
that’s all you have to say, just because someone told you about some experience
or something that isn’t related to food doesn’t mean you’ve done anything
wrong.
And I know as a new dietician, I thought that sometimes I thought, why is this
person telling me about X, Y Z. This isn’t about nutrition. And I realized that it’s
not the patient’s role to determine what is, and isn’t about nutrition. It’s my job
as a dietician to sift through it and find out where the nuggets that I need to take
and help with nutrition related advice versus which are the nuggets that are not
in my area.
And sometimes that does take practice, but like I said, it’s not ever wrong to talk
through something with someone, as you think you’re going towards food and
eating, and then they realize, oh, you know what? That wasn’t about food and
eating after all. And as a hospital dietician, this is another question you
mentioned that we haven’t really talked about yet, but that idea that I don’t know
what to do with this person to help this person in a short term situation, there
isn’t a lot you can do. You don’t have to figure out the origin of someone’s eating
behavior. Really the key in a short-term situation is to figure out, is there
anything that can nourish that person that you can provide?
So is there anything that they can keep down? Is there anything they can
tolerate? Is there anything they’re willing to eat? And even if that’s not the mostnutritious combo then, can you provide that in a safe environment for someone
to eat? And that’s really the key to the whole operation. And I do remember
many times recommending things that I thought, oh, my internship director
would not be impressed with this meal plan that I just gave someone because it
wasn’t balanced at all, but it wasn’t about balance, right?
It was about, is there something that this person can use as sort of a starting
point for practicing nourishing themselves?
[00:31:46] Melissa: Thank you so much for illuminating the therapist aspect,
the scope of practice, because I can imagine that that’s a huge barrier for
dieticians and that reassurance and that those guidelines are very helpful.
[00:32:01] Jessica: People often say to me, well, how do I know I won’t make
their eating disorder worse? And I always just think, you know, what? If they’re
in the hospital with an eating disorder, it’s already pretty bad. So you having
some compassion and listening and trying to find a way to help is already a step
in the right direction.
There’s not, I mean, again, there’s exceptions to everything, but there’s not a lot
you can do to make someone’s eating disorder worse when it’s already in that
place. I would say that the number one thing you can do, and unfortunately this
does happen, hopefully not by dieticians, but that can make someone’s eating
disorder worse is to say, well, your eating disorder really isn’t that bad.
Or, you know, based on your weight, you don’t really have an eating disorder.
Those are things that can make someone’s eating disorder worse in a sense that
they can discourage someone from getting the care that they need. But other
than that, Trying to help is a great service. And then the other piece is trying to
get them to the appropriate care that can help them more.
And that often falls to the social worker. But sometimes as a dietician, you may
have, you know, a network where you can ask, you know, where would be a
good place to recommend for this person or who would be a good dietician to
see them for the longterm.
[00:33:06] Melissa: Wow. That’s a powerful concern. How do I know I’m not,
not just not helping, but making it worse.
What are some other common pain points or concerns that you hear that I
assume we could talk about your eating disorder bootcamp in a little bit aboutlike, you know, what you cover and what, what you really feel like most
dieticians who just want to be better practitioners, like you said, I think it’s a
really important point that you don’t have to want to specialize in this.
We need more practitioners to just be a comfortable with this. Like I’m a
certified diabetes educator, but a lot of dieticians will talk with patients about
diabetes, you know, it’s going to happen and what can you do to improve and
increase their comfort level?
[00:33:48] Jessica: There’s a couple of things that I would say to dieticians that,
you know, I sort of learned the hard way and maybe I can save you some time.
One is that people who find it easy to change, aren’t seeing a dietician, right?
They just did it. They just changed. Or they saw a dietician one time got some
advice changed or they read a book and changed. The only people who end up
seeing a dietician usually are people who find it difficult to change and need
support and help.
And so there’s that aspect of what you had mentioned. I think at the beginning
of like, am I really helping? Or this is so frustrating. Well, yeah, if you’re
frustrated, believe me, that person who’s trying to change is frustrated too. And
so a lot of times my soundbite in that situation is something like, you know
what, you’re bringing a lot of work to the table.
I know I’m a good dietician, but it seems like the skills that we each bring to the
table are not adequate to manage this situation. So who can we bring in that
might be able to help us? Or who can we bring in that might have more
information and through that sort of involving family members, or maybe even
someone like a roommate.
Anyone that might be able to help support someone or provide more
information. I’m a big believer in getting more people on board. That could be
someone who’s a specialist in time management or in learning disorders. There
are so many different aspects that food intersects with that it’s really okay to say
as a dietician, I’m bringing my best to this situation.
And yet there doesn’t seem to be a lot of progress in the way that the client is
hoping for or that I’m hoping for. And so to bring more people on board, we
don’t need to fill ashamed – the same way someone, an individual shouldn’t feelashamed about their eating. We, as dietitians don’t need to feel ashamed that
we’re having difficulty helping someone.
We don’t even know what cures eating disorders. We don’t have a set protocol.
So a lot of it is creativity on the part of the dietician, trial, and error, seeing what
will help. And it’s really important not to judge yourself as a dietician. On the
other hand, if you feel like you’re outmatched, you can always get consultation
from another dietician who is a specialist in eating disorders.
And ultimately to me, I would rather coach someone who already has a good
relationship. So if you’re someone’s diabetes, dietician, and they need help with
an eating disorder I would rather coach you on how to help them because you
already have the relationship with them rather than sending them to me or to
another eating disorder dietician that they have to start over with.
Because to me, the relationship is so much of the de-shaming and the freedom
to talk about the things that are going on that I don’t want to disrupt that, but at
the end of the day, if someone listening feels like this is just not my bag. I get
too frustrated or I really feel like, I don’t know how to help no judgment on that
either.
It’s good to know yourself. And you can always simply say, you know what,
based on this new information or based on these symptoms that you’re sharing
with me, I’m really glad and honored that you shared, but I may not be the right
dietician for you. I’d like to help you find someone who specializes in that area.
And that’s okay, too. So there’s really no right or wrong, staying with a patient
and getting consultation to help you or saying I’d like to refer you on to
someone else. It’s really a decision that, that you have to make for yourself. And
I would say in consultation with a colleague, you know, our ethical guidelines I
have to say are very vague, but for the most part, what I take away from our
dietician ethical guidelines is the ethical dietician will consult with
knowledgeable colleagues when they have a dilemma.
And so it might make sense to talk it through with someone on your team and
say, you know, I’m not sure if I’m the right person, should I get consultation or
should I send them onward to someone else? I think that those are some of the,
you know, you kind of were asking about sort of pain points, but I think that’s a
lot of what I hear from dieticians is just that worry of, you know, am I
abandoning someone if I recommend someone else? And I don’t think that’s thecase at all. You’re actually bringing someone else on board the team in order to
help in a way that’s different from the skills that you have.
[00:37:35] Melissa: Oh, this is very interesting. And I can see, as you’re talking
for me, there’s some parallels with diabetes. I continue to learn with new
patients and new medications and new situations. And I find that invigorating. I
find that very interesting. I don’t find it daunting. I don’t feel insecure about that,
but with eating disorders, I can see that like some dieticians might find that
continual learning and growth in that particular cope very exhilarating as well
and very fulfilling. So I’m really glad that you’re bringing people into the fold..
[00:38:33] Jessica: Well, and that’s why there’s different specialties, right?
Yeah. But I do think a lot of people in school got the message that there is no
role for dieticians and eating disorders, or it’s a very rare job and that’s just
completely wrong.
We need more dieticians in the eating disorder field. If it’s an area, you have a
passion for. Absolutely. Let’s get you specialized in it. If it’s an area you don’t
want to specialize in. That’s great too, because we need dieticians in the other
areas too. It’s just helpful to have some knowledge of eating disorders, because
as we said before, just because you don’t specialize in this area, doesn’t mean, I
mean, maybe if you do research studies with, you know, rats, but that’s the only
situation I can think of anyone who’s doing any kind of counseling with humans
is encountering people with dysfunctional eating behaviors, but there’s a
difference between being an expert and having a working knowledge.
[00:39:20] Melissa: And I think that’s the most powerful thing that I’ve learned
from you, besides of all, all the interesting intricacies about like the different
types of eating disorders, but just the point that we can have more dieticians
have that comfort level and confidence. And that, that way we can help that
many more people. You just published an article I’d like you to tell us about –
you surveyed some dieticians.
[00:39:43] Jessica: Yes. So Paula Quatromoni and I surveyed 182 dieticians
responded. We asked questions about job satisfaction. And what’s your
workload like and where did you get your education on eating disorders? And
one of the biggest findings that we had when looking at the results was that
most dieticians who, and this is dieticians working in the eating disorder field,
most of those dieticians did not get any training in school related to eating
disorder care.We, and I include myself in this group, we got our education from continuing
education that we did separately. I mean, there’s some on the job training in
some cases, but for the most part, it seemed like dieticians were paying for their
own supervision and consultation with more experienced dieticians paying for
their own conferences and other kinds of continuing education.
There wasn’t a lot of support on the job either. And so what we found was that
the most acute patients are being seen by the least experienced dieticians. And
we thought that that might have an impact on patient care, which isn’t something
that we studied, but it was one of our sort of possible items for future research.
And to me, every dietician should have, like we said, some education on eating
disorders and not just that one paragraph in a nutrition textbook that sort of
gives the diagnostic criteria, but it could roll into all counseling skills. And one
of the comments on our survey, which I thought was so crucial that we included
in the article was that they said that some level of eating disorder knowledge is
important for people working everywhere from corporate wellness to any other,
you know, area of dietetics. And I think that’s true. That really supports what I
think also. Simply because eating disorders – I’ve had conversations with
people who are sort of high up in different dietitian organizations.
And they say, well, you know what? Eating disorders is just never going to be in
our top 10 of priorities. And when I look at the top 10 of priorities, every single
one of them overlaps with dysfunctional eating behavior, food insecurity,
overlaps, dysfunctional eating behavior. Hunger and environmental nutrition
overlaps with dysfunctional eating behaviors, diabetes care, renal disease, every
single thing that’s in the top 10 is going to intersect with dysfunctional eating
behaviors in some way, whether it’s caused by them, whether it promotes them.
And so to say, it’s never going to make it into our top 10. I sort of laugh at that
and say, you’re right, it’s an umbrella over all of your top 10, but I haven’t quite
been able to get that message to the large organizations. That’s why I actually
ended up starting my own organization for eating disorder, dieticians or eating
disorder, interested students.
And we have a thousand members. So obviously there was a need for an
organization just for eating disorder dieticians.
[00:42:35] Melissa: Wonderful. Is that the eating disorder bootcamps or is that’s
something else?[00:42:38] Jessica: No, no. That’s the international Federation of eating disorder
dieticians, and we can put a link to that in the show notes.
[00:42:45] Melissa: Perfect. Wonderful. Well, I will say the diabetes world
hears you loud and clear. We’ve long known that diabetes and disordered eating
can very much go hand in hand more typically with type one because they tend
to be younger going through adolescence and puberty and everything, but
certainly with type two as well, you know, anytime that you have to, I shouldn’t
say, have to, but you’re called to change your eating habits and you’re
monitoring all of this stuff and your blood sugars and everything. It’s just, it can
be a lot and it can trigger a lot of things.
[00:43:18] Jessica: Well, sure. Because it triggers anxiety and anxiety can
influence food and eating behaviors. So, yeah, absolutely. I agree. And I’m not
talking about dieticians in the field.
I do think dieticians in the field, absolutely in many areas recognize the need.
It’s more of the organizations that are in charge of what students learn that I feel
like have not gotten the message.
[00:43:40] Melissa: Connecting those dots for sure. Well, you know, and I
could say the same thing about communications, but I do think that’s improving.
Gosh, you know, communications should be an integral part of everything that
dieticians do on every level. But I think that that’s improving.
So we talked about the four different origins and I would like to take an
opportunity to have you talk a little bit more about that fourth origin, the
external environment, diet culture because it’s, it’s just such a hot topic right
now, and I have not addressed it much on the podcast.
So I would love to kind of hear your little brain dump on what’s going on with
that origin and any insights you can share with us, whether, you know, we’re a
person struggling with this. And I think, I mean, I think everybody is impacted
by what we see in diet culture, from our own personal perspective, all the way
this during eating disorders awareness week. I just gave a talk last night to a
college kid. And, you know, a big piece of what we’re sort of seeing with the
rise in eating disorders during COVID has been building for a long time. Sothere have always been aspects of the culture that have promoted you know,
your body isn’t good enough. And therefore you need a product. Whether that
product is a diet, whether that product is shampoo for your frizzy hair or razors
to shave your legs, right? There’s, there’s so many economies, industries that are
based on the idea that your body isn’t good enough as is. There’s products to
make your body bigger, products to make your body smaller, products to make
different parts of your body bigger or smaller.
Right. And so it’s really important to keep in mind that this is not new. And
something that was new for me was to learn that racism is a big factor in that.
And that the ideal of whiteness is a big factor in some of the things that we sort
of imagine to be you know, that appearance ideal. So like I said, you know,
frizzy hair, less body hair, you know, having pale smooth skin, like there’s so
many things in sort of our cultural beauty ideal that are based on racism and
based on separating people into categories. And so it’s so not new. The only
thing that’s new is the difference in sort of technology in distributing those
messages. So where in order to look back at the messages, let’s say from the
1920s, you’re going to have to look at newspaper and magazine ads for
products. That’s where you’re going to see the beauty ideals of that era. Now
you look at Instagram or, you know, by the time this recording comes out, there
probably will be 10 new platforms. Right? You look at Tik TOK, you look at
social media and that’s where we’re getting our information about the body
ideals or the beauty ideals that supposedly we’re supposed to conform to.
And the bottom line is they’re all about things that we don’t even realize. We’ve
internalized them as being our own desires or we’ve even been, you know, sort
of lied to and told that these are sort of biological genetic constructs, like it’s
normal for, you know, let’s say men to be attracted to women with big boobs
and things like that.
We think we’ve been taught that’s in our genes and really its just a preference!
And it’s a preference we’ve been taught, you know, so that kind of thing, it’s
just, I wish we could look at bodies and just say, you know, basically there’s a
diversity of bodies, just like there’s a diversity of everything else. And I heard a
really good example.
I didn’t make it up. I wish I did, but it was something. You know, you don’t burn
a Picasso just because it’s not the Mona Lisa. Right. You can admire both of
them and think they’re both beautiful. And so it’s really about expanding our
minds to accept that even if we all ate the same foods and exercise the sameamounts and got the same haircut, we would still all look different and that’s
normal and that’s okay.
And so that is such a hard concept though, when you’re looking at yourself in
the mirror and whatever parts you don’t like seeing emphasized. It’s so
important that we recognize that we are being influenced by so much more than
our own beliefs. That’s what food fairytales is really about is looking back and
trying to figure out what messages you got.
And unfortunately, some of the messages conflict, and that’s because they’re not
real, right. If they were real, there’s only one truth. Right. But if, sometimes you
feel too big and sometimes you feel too little, neither one of those could
possibly be true. Right. If sometimes your hair’s too curly and sometimes it’s too
straight, you know, neither one of those is true because it can’t be the same
thing.
If you’re in a bad mood and suddenly you look down and your body seems to
have changed, that can’t be right. But we tend to think, we believe in our own
thoughts, let’s say. And so another sort of touchstone that I go to sometimes is
don’t believe everything you think. And maybe that will help someone who is
listening to this, you know, just very simple, write it down.
Don’t believe everything you think. Thoughts are just chemicals in a way, you
know, sort of like leaves floating down a river and you get to pick which one to
believe. So if your, your thoughts are equally not factual, why not pick the one
that says instead of the one that says I’m never good enough? And you know, it’s
not that easy to change, you know, I’m not saying it’s simple, but I think that you
know, accepting that diet culture or appearance culture or racism or genderism
or sizeism or ableism are all factors that are affecting us, whether we realize it
or not. I think that’s a first step, at least in untangling ourselves from, we cannot
untangle ourselves from culture unless you go live in a cave, but untangling
yourself from being so impressionable by the culture.
[00:49:10] Melissa: Very good. Very good. Yeah. I touched on the racism aspect
a little bit back on an episode, I believe it was called the science and culture of
obesity and it’s a two-part series. And I believe it was part two with Noel
Theodosiou. I will link to that in my show notes as well. If anybody’s interested
a little bit more, she’s a behavioral scientist you know, kind of just looking at the
origins of you know, some of the, what you mentioned, like thin ideal or youknow, the pale skin and, and all of that. And what culture says is attractive. So
just wanted to mention that.
As we’re wrapping up here, I want to hear any just general takeaways you have
or specific takeaways that you have for people who might be struggling with
disordered eating body image issues, and then also some takeaways for
healthcare professionals.
[00:50:03] Jessica: Sure. So for individuals who are struggling, which by the
way might also be healthcare professionals, right? It’s not two distinct groups.
Exactly. But anyone who is thinking, you know, well, my problems are so
minor, no one wants to hear about them or they don’t rise to the level of, you
know, you can’t see my finger quotes, but an eating disorder.
It’s not that big of a problem. I would just encourage you to think about the way
that what I learned from the college speakers when I was on a college speakers
bureau, they talked about alcohol abuse and they speak about it in a different
way that I remember when I was you know, that age and I, it’s not about how
much you drink.
It’s not about what you drink is not about which kind of alcohol you drink. It’s
not about how early in the morning. It’s about do problems happen when you
drink? That is the key issue with food as well. Do problems happen when you
eat or don’t eat? Because like I said, the same person could eat the same six corn
dogs and they’ll really fueled for their marathon.
Whereas there’s another person can eat six corn dogs and feel like they don’t
deserve to live. And not sure why I thought of corn dogs. I must be craving corn
dogs, but my point is, don’t worry about how you compare to others or how you
compare to even to yourself at a different time when maybe you did feel like
you had an eating disorder, think of it as do problems happen when you eat and
whether those problems are mental or physical or anything else, social.
Do you feel like you have to eat by yourself, you have to eat alone because
you’re embarrassed of your eating? I mean, these are things that are problems,
even if, you know, we don’t recognize them as a society as problems. And so I
would encourage you to meet with an eating disorder dietician, even if you don’t
feel like you identify with the word eating disorder.
Because that eating disorder dietician is going to be the person who can help
you sift through and see what is nutrition related and what isn’t. Because ifyou’re trying to solve problems with food or with not eating, that aren’t really
food related, it’s going to be very discouraging. And so I really encourage you to
talk with someone, if not a dietician, then a counselor, if not a counselor then a
best friend or someone supportive, that can be a good listener.
[00:52:04] Melissa: I want to just jump in. And you mentioned a couple of
times about kind of realizing, and these are my own words, but it’s kind of
paraphrasing what you’re saying. I think. when you realize your behaviors are
not really connected to the problem, or like, it’s not about food, I think that that’s
really powerful.
I remember learning that and that was like a really light bulb moment for me.
And I talk a little bit about my eating journey. I’m not going to say eating
disorder – my disordered eating issues a little bit. In an, in an episode that I did
with ballerina dietician. And I’ll link to that in my show notes as well.
But when I made that connection, it just like, it was a light switch. It just really
flipped everything for me. So I think it’s really powerful to reinforce that idea
when it just sort of helps kinda take a step back and reassess everything. I don’t
know if that’s, if that makes sense.
[00:53:00] Jessica: Yeah, I agree. And I had that kind of epiphany too –
realizing what I was doing with my eating wasn’t really about food.
It was about my feelings, about a particular person I had a crush on. So, you
know, absolutely. I think. There are lots of ways that dysfunctional eating
behaviors are not about food, but I think there are ways that they are too. And I
think that it’s easy for a dietician sometimes to say, well, I have no role here
because if this isn’t really about food, but I think it’s so important that there’s
both roles because no, it’s not about food, but when someone has been doing
behaviors with food or believing things about food, they don’t just change just
because they may solve the underlying issues.
Let’s say someone’s depressed and it’s affecting their eating. Maybe in a very
few cases, solving the depression, solves the eating – houray! But in a lot of
cases, someone’s going to need help with their depression and help with their
eating. And so that would be the message that I would leave with the health
professionals listening is that, you know, there is a place for a lot of different
pieces of the puzzle, someone who is struggling with their eating, maybe
compensating for some kind of medical issue, that’s been undiagnosed.We need to get a doctor involved, right? Sometimes an endocrinologist.
Sometimes a cardiologist. Don’t feel like you have to be the person who is doing
this alone. It’s, it’s actually, in my opinion, not appropriate to be doing it alone.
And so, you know, the same way I would say to an individual who’s struggling.
Try if you can to remember my words that, you know, whatever you’re doing, it
may be causing problems, but it’s nothing to be ashamed of. It doesn’t mean
there’s anything wrong or broken about you. Same thing with a health
professional that feels outmatched by someone’s eating disorder. It doesn’t mean
you’re wrong or broken, or you missed that day in school, you’re dealing with a
very difficult issue.
And I’ve said many times, you know, sometimes we only realize later that your
eating disorder is more severe than what we wanted it to be, or it’s more tricky
than what we wanted it to be, because if it wasn’t, you would have solved it a
long time ago. And so that’s why we need to bring someone else on board onto
the team.
So I guess my biggest message that goes to both individuals who are struggling
with their eating and professionals is simply, you know, don’t try to do it all
yourself. It’s not a DIY project. I know nutrition is sort of promoted out there as
something you can wrangle yourself, but to me, you can’t solve a problem with
the same mind that created it.
You’ve got to get at least one additional pair of eyes, maybe sometimes more
than one with different skillsets. And it’s okay if those people don’t agree, but
it’s really important to get other people helping you. It, it just, I think eating
disorders thrive in isolation and we need to sort of open the doors to individuals
to get care.
And there’s a lot of barriers and I hope you will not let shame be your barrier.
[00:55:34] Melissa: Thank you so much. You’re saying so many powerful
things. I’m sitting here going. Oh wow. So thank you, Jessica. Where can people
find out more information? I know you have a website and your social media
handles, and also if you want to just share like what people can find in the
eating disorders bootcamp too.
[00:55:52] Jessica: So my umbrella homepage website is Jessicasetnick.com.That’s where you can go to, you know, bring me to your campus to speak or
anything like that, schedule a consultation and then eating
disordersbootcamp.com is where the information on eating disorders bootcamp
And it’s really comprehensive. There’s three audio workshops. There’s books
that come with it. I mean, it’s really more than I can say right now, but you
know, you’re welcome to check it out on the website.
I just rerecorded a new introduction to eating disorders bootcamp, and that is
available as a free download with the slides for anyone who wants it, whether
you’ve taken eating disorders bootcamp before or not. You can listen to that new
introduction if you’d like to. Okay. But, yeah, I mean, I feel like there’s also
other people’s courses and I have a list of other resources on my site.
There’s a lot more out there than there used to be. And we can put a link to that
list of resources, even in your show notes, for someone who’s more advanced
that might be looking for something more advanced. I’m happy to help in any
way I can, you know, I wish that I could say I foresee the end of eating disorders
in my lifetime, and I could just retire and talk about it as like this thing that we
used to deal with, like polio, but I don’t see that happening. So we’re just going
to need lots more people who want to help.
[00:57:05] Melissa: And hopefully talking about it more helps remove some of
the mystery and stigma and barriers to access. So thank you so much for the
amazing work that you’re doing and for coming on my show and sharing all of
this important information. I’ll have people check out your website, but like you
said, we’ll have links in my show notes as well at soundbitesrd.com.
And I hope to see you in person sometime soon.
[00:57:29] Jessica: Yes. Same. Thank you for the platform. I really appreciate
the opportunity to spread the word and yes, I hope we get to see each other in
person as in-person meeting starts coming back.
[00:57:38] Melissa: Absolutely. Thank you again. And for everybody listening
as always enjoy your food with health in mind. Till next time.
LISTEN, LEARN AND EARN
Listen to select Sound Bites Podcasts and earn free CEU credits approved by the Commission on Dietetic Registration (CDR) for registered dietitian nutritionists and dietetic technicians, registered. Get started!
Get Melissa’s Sound Science Toolkit here!
Partnerships:
Sound Bites is partnering with the Association of Diabetes Care and Education Specialists (formerly the American Association of Diabetes Educators)! Stay tuned for updates on the podcast, blog and newsletter!
Sound Bites is partnering with the International Food Information Council! Stay tuned for updates on the podcast, blog and newsletter!
Hi Debbie,
Thanks for catching that – I had forgotten to include that and the Eating Disorders Resource list which is now being added to the resource list above.
Thank you!
Melissa
I am just listening to this in December 2022, but this WAS SO GOOD. Jessica really made some excellent points and spoke a lot to some concerns I have been harboring (such as – can I made an ED worse, social media and disordering eating with the rise of the influencer). Thank you so much.
And yes, racism has largely factored in ED and I am glad this was also addressed. As a POC and RD, this is something that is present, but needs to be spoken about more frequently.
Sign up for my monthly newsletter and episode eblasts so you never miss an update!
Listen on Stitcher (Android)
Install the Stitcher App
1. Search for “sound bites with melissa joy dobbins” 2. Choose Play Current Episode or Add to Playlist
Choose “Play Episode”
Subscribe & Review on iPhone
Open the “Podcast” app on your iPhone
Search for “Sound bites with melissa joy dobbins”
Open the podcast and click “Subscribe” and your done!
Write a Review
Click “Reviews”, then “Write a Review”.
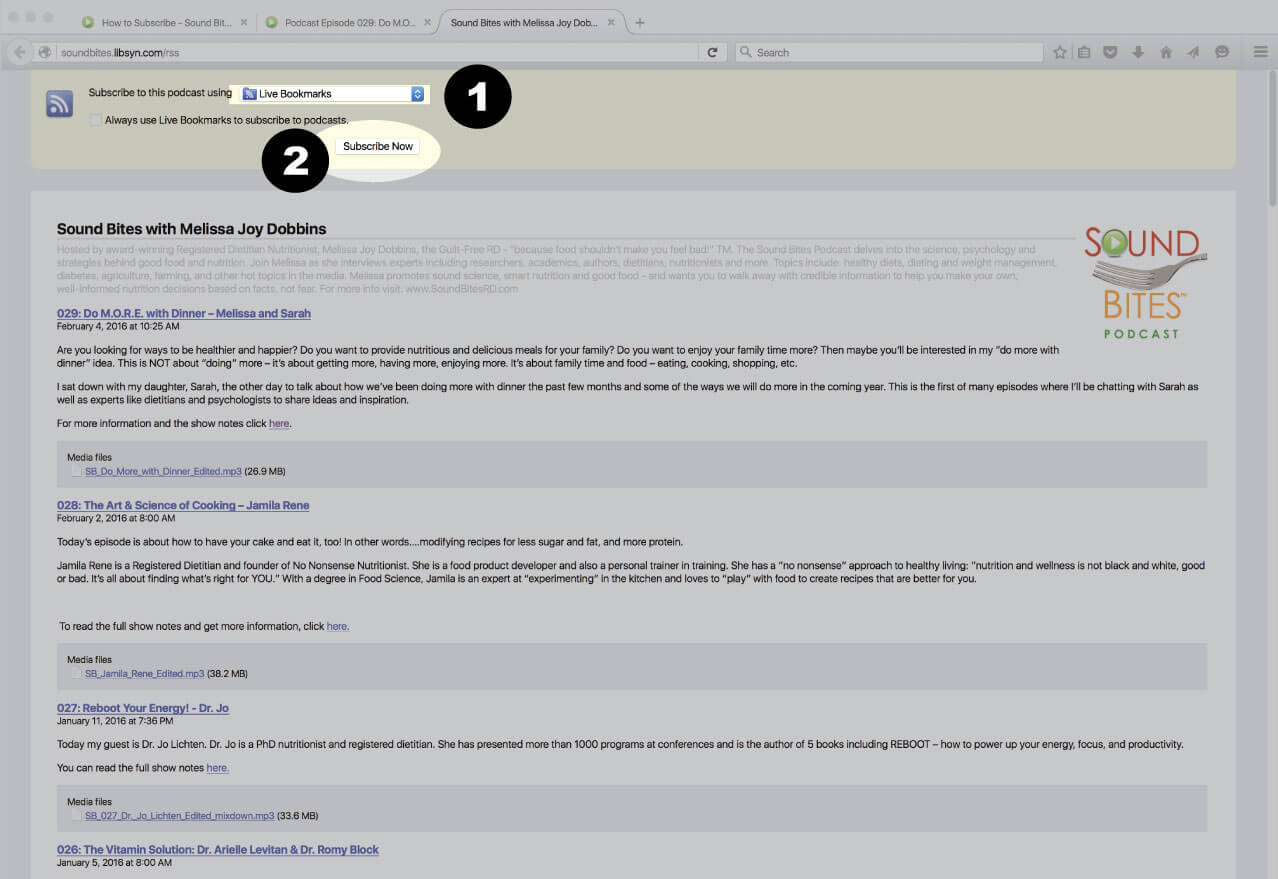
Subscribe via RSS Feed
Navigate to any podcast player . Click on the RSS feed icon.
Click on the RSS feed icon.
Click on RSS Feed
Choose which application you would like to use to receive the RSS feed
Click “Subscribe Now”
Confirm settings and subscribe.
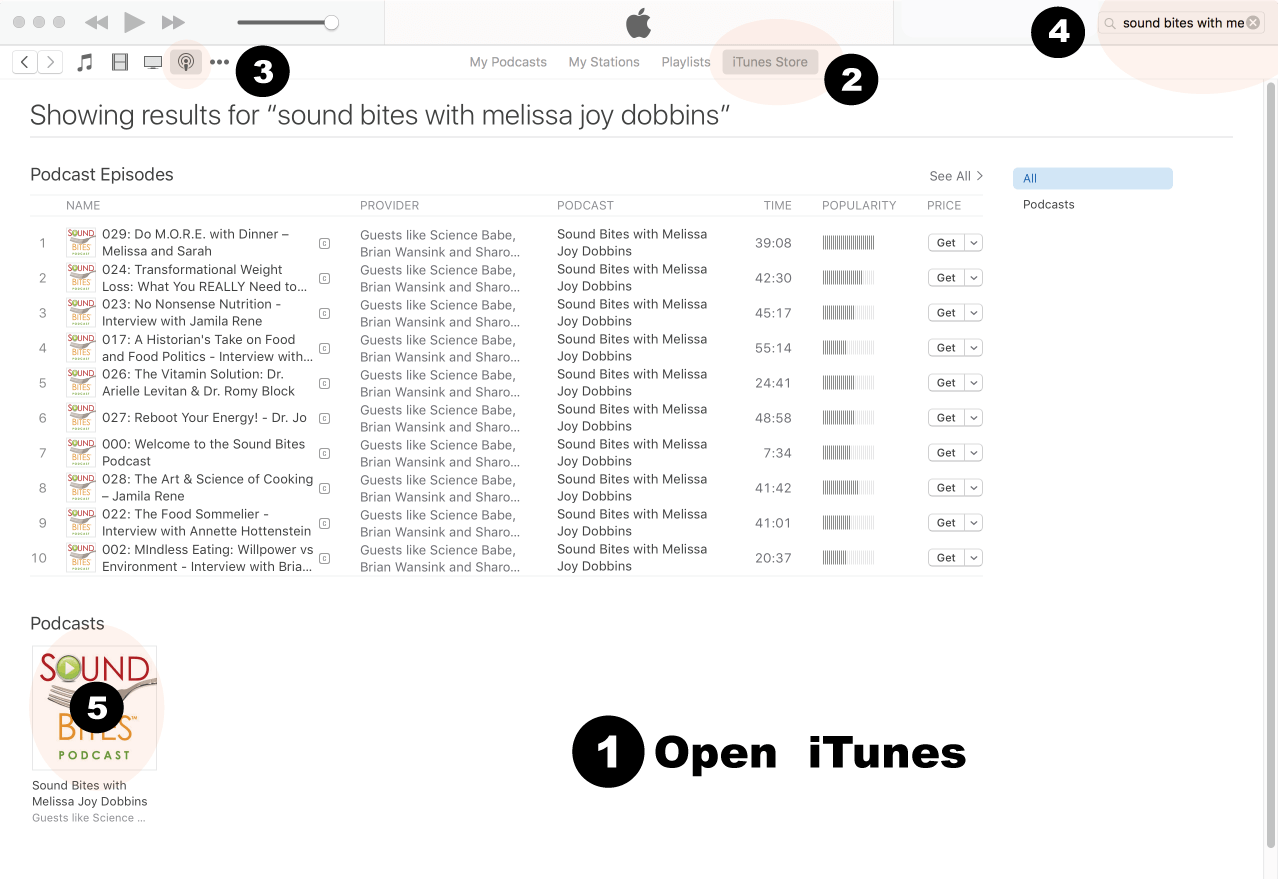
How to Review in iTunes
Open iTunes desktop application
Click iTunes Store
Click on Podcasts
Search for “Sound bites with Melissa Joy Dobbins”
Click on podcast image
Search for Sound Bites podcast in iTunes
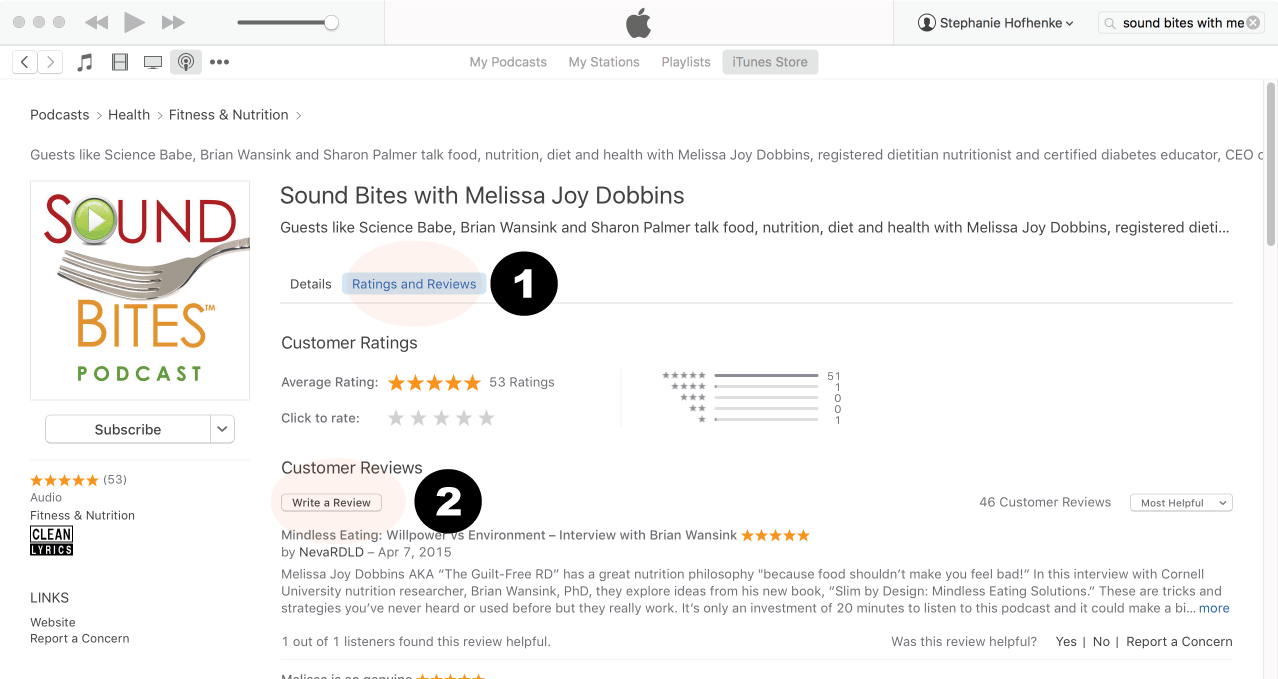
Click Ratings & Reivews
Click Write a Review
View reviews and write your own review.
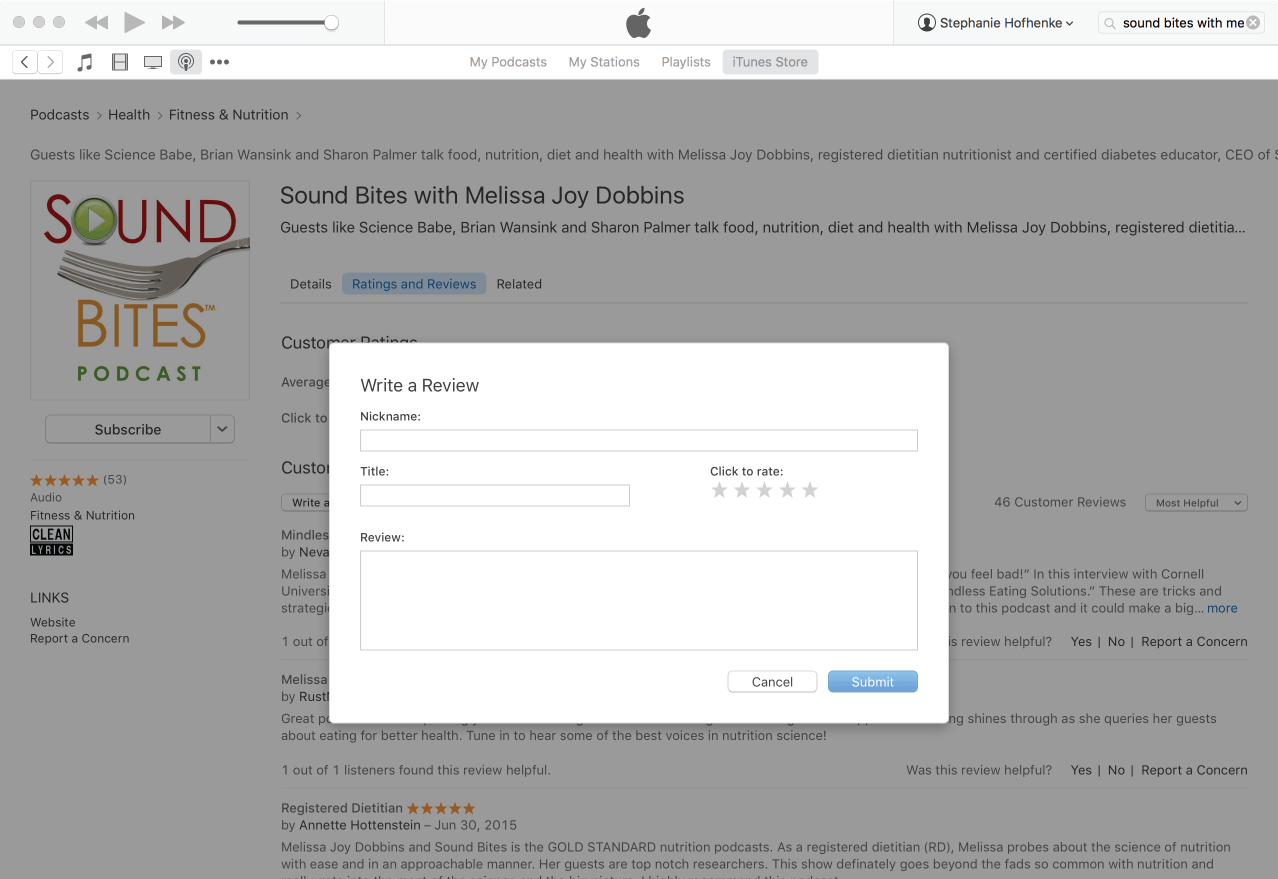
Write your review…. Thank you!
Write your review!
How to subscribe via iTunes
Click here to view the Sound Bites Podcastin iTunes, then click the blue “View in iTunes” button. This will open your iTunes application directly to Sound Bites Podcast. Click the “Subscribe” button, and your done!













Hi Melissa!
Love your podcast.
Looking for the handout about the 4 origins of ED, that was mentioned by Jessica-
she said it would be in the show notes.
Thank you!
Debbie Serenius RDN debbie@nutrition-advantage.com
Hi Debbie,
Thanks for catching that – I had forgotten to include that and the Eating Disorders Resource list which is now being added to the resource list above.
Thank you!
Melissa
I am just listening to this in December 2022, but this WAS SO GOOD. Jessica really made some excellent points and spoke a lot to some concerns I have been harboring (such as – can I made an ED worse, social media and disordering eating with the rise of the influencer). Thank you so much.
And yes, racism has largely factored in ED and I am glad this was also addressed. As a POC and RD, this is something that is present, but needs to be spoken about more frequently.
Hello, I LOVED this topic! Thank yall so much!
i tried to use the discount code for the Fairytale book but it is not working. is it expired?
Thanks Rachel! I reached out to Jessica and she is fixing the error with the coupon code. Please try again when you get a chance.
Melissa