Celebrating over 1 Million Downloads and 50,000 Free CEUs on the Sound Bites® Podcast | NEW: Get 1 years’ worth of CEUs with the new 15-CEU Podcast Course
This episode offers the opportunity to earn 1 free CEU credit through Dietitians on Demand. Simply enjoy the podcast, complete the quiz and reflection, and download your CEU certificate. Get started here.
Disclosure: This episode is not sponsored.
A Primer on Food Allergies, Tests and Diet Therapy
A considerable amount of misinformation exists about food allergies among the public and health professionals alike. This episode delves into the prevalence and pathophysiology of food allergies, emphasizing the difference between self-reported and diagnosed cases, with around 6% of both US adults and children affected. The immune-mediated nature of food allergies and the various types of reactions they can trigger are discussed as well as the importance of clinical correlation with test results, because tests like blood, skin prick, and patch tests can yield false positives. The food elimination diet and oral challenge process are employed to eliminate and reintroduce suspected food antigens, however potential nutrient deficiencies can become a concern when eliminating multiple foods or food groups. Strategies to reduce the risk of food allergies, including early introduction of allergenic foods to infants are highlighted. The role of dietitians in managing complex cases involving multiple allergies, infants, and comorbidities is emphasized.
Tune into this episode to learn about:
What are the “Big 8” food allergens and what additional food has recently been added to that list
Prevalence of food allergies in the U.S.
The difference between food allergies and intolerances
The 5 different categories that food allergy reactions are classified into
Various types of food allergy tests
What you need to know about at-home tests
How the elimination diet works
What an oral challenge entails
The potential for micro- or macronutrient deficiencies
Current guidelines for infant feeding to help reduce the risk of food allergies
When and how dietitians should get involved
At-home tests should not be used to replace an official physician-provided test and subsequent medical diagnosis. The American Academy of Allergy, Asthma & Immunology states that at-home food allergy tests may not provide accurate results. It warns that using alternative testing such as IgG testing, home allergy test kits, skin titration and applied kinesiology. If a person does take an at-home test, they should follow up on any positive results with a doctor.
Sara Glanz, MS, RD, LD, CNSC
Sara Glanz has been a practicing dietitian for over 10 years. Currently, she is the Director of Clinical Education at Dietitians On Demand. She started working for Dietitians On Demand in 2016 as a traveling dietitian before joining the corporate team in 2018 to create educational resources for dietitians. Since 2018, she has had the pleasure of directing a team of talented Subject Matter Experts. Together, they have created a thriving library of clinical and professional resources that have reached nearly 10,000 dietitians and nutrition professionals worldwide.
Outside of work, Sara is an actively engaged member of ASPEN and has served on several of their committees, including the Nutrition Support Fundamentals, “Forward an Article,” and Malnutrition Awareness Week Social Media Committees. Currently, she is the co-chair of the ASPEN Self-Assessment Committee.
Owing to a very progressive-minded mentor early in her career, Sara believes dietitians deserve to be key members of the interdisciplinary team. To that end, she always advocates for dietitians to be present, speak up, and stay involved in patient care.
[00:00:01] Speaker: Welcome to Sound Bites, hosted by registered dietitian nutritionist Melissa Joy Dobbins. Let’s delve into the science, the psychology, and the strategies behind good food and nutrition.
[00:00:24] Melissa Joy Dobbins: Hello and welcome to the Sound BitesPodcast. Today’s episode is about food allergies, the prevalence, the pathophysiology, food allergy tests, and diet therapy, such as elimination diets, plus the latest research on reducing the risks for food allergies. My guest today is Sara Glanz. She’s the Director of Clinical Education at Dietitians On Demand. In this role, she has championed the continuing education program to empower dietitians everywhere to achieve their professional goals. Sara’s professional interests and expertise lie in nutrition support and critical care. Welcome to the show, Sara.
[00:01:02] Sara Glanz: Thanks, Melissa. I’m really excited to be here with you.
[00:01:05] Melissa: Yes, I am excited about this topic. I have not covered it in depth on the podcast yet. I have a few somewhat related episodes with intolerances and peanut allergies specifically, but I’m really curious about the topic and love that we’re going to dive into that today. I want our listeners to know that this episode is not sponsored and that we may be submitting this episode to the Commission on Dietetic Registration for continuing education credits for registered dietitian nutritionists, dietetic technicians, registered, and certified diabetes care and education specialists.
Sara, I would love to start off with learning a little bit more about you, your background, maybe your education, how you got interested in becoming a dietitian, and specifically the topic at hand, how you got interested in food allergies, and just the work you do, and anything about Dietitians On Demand that you wanted to share, and of course, any disclosures you have to know.
[00:01:59] Sara: Okay. I’ll start with disclosures. I don’t have any conflicts of interest or commercial sponsorships or anything like that, so we can get that out of the way. I’ve been a dietitian now for about 10 years, which is hard to believe it’s been that long. I’m from Kentucky, so I got my undergraduate degree at Western Kentucky University, and attended my dietetic internship and completed that through Baylor University Medical Center in Dallas, Texas. It was really there that I had such a great learning experience with a lot of dietitians who were experts in their field and really encouraged to do more, just be more, do more, be present, be vocal. That really stuck with me all these years.
When I finished up my internship, I stayed on at Baylor for my first job. I was a single site dietitian, so I really had the opportunity to learn a lot about everything really. Because I was the only dietitian there, and so I had an opportunity to be on different committees, and work really closely with the physicians, and have some food service interactions as well. It was an incredible experience. I learned a lot, and I knew that I just wanted to do a little bit more with my career and move up to the next level. I actually quit my job and went back to school full-time, which was a crazy idea that I had-
[00:03:22] Melissa: Wow.
[00:03:23] Sara: -but I did it, and I went back and got my master’s. As I was finishing up my master’s, I was in this limbo of, I was finished with my coursework but still had my master’s thesis to do, so I didn’t feel like I could commit to a full-time job. I was looking for something to do, and I came across Dietitians On Demand. They offer traveling opportunities for dietitians and I said, “What the heck, let’s give that a try,” and signed up to be a traveling dietitian. Within about 10 days, I had my first travel assignment in California.
[00:04:00] Melissa: Nice.
[00:04:01] Sara: That was, it started, kicked off that journey. About a year or so into traveling with Dietitians On Demand, I started writing some blogs for them, and doing a little bit more with content production. We hosted our first webinar together, me plus Dietitians On Demand. That happened in the spring of 2018. By the fall of 2018, I had a full-time job on the corporate team with Dietitians On Demand, doing some content creation, and like you mentioned, I’ve worked with a team of dietitians.
Now, I have my small but mighty team of subject-matter expert dietitians. They’re phenomenal because they bring to the table such a level of expertise in their own particular area. It makes it really special to be able to work with them because they have so much more knowledge than any one person really could ever hope to have. With them, we create all kinds of blogs. We have free infographics, which are these one to two-page handouts, printouts that you can hang up at your desk or use for patient education. We offer on-demand and live webinars, which are very popular for dietitians. We have our weekly fall conference called the Wild Week of Webinars. We call it WWOW for short.
[00:05:30] Melissa: Nice.
[00:05:31] Sara: During WWOW, we have two live webinars every day, so it really is a wild week, but dietitians seem to love it. We started offering NFBE training. Really, what we try to do is be a resource for dietitians. Whether they are looking for a job or if they’re not looking for a job, we have resources to support them in their careers. That’s kind of what we do over in my neck of the woods, but I’m excited to talk about food allergies.
Food allergies is such an interesting topic for me. Like many dietitians, I’m sure we have all encountered patients– My background is in clinical nutrition, primarily in acute care, so I’ve encountered a number of patients over the years who claim to have food allergies. They claim to be allergic to many, many things, or they have lots of food intolerances, and so it can be challenging working with patients who have or believe they have a lot of food allergy issues or food-intolerance issues.
What I have found is sometimes, they can create these unnecessary barriers for getting good nutrition, and there are lots of– We’re going to be talking a little bit about the at-home kits that you can use and the information, of course, that’s online, that you can test yourself for food allergies. I think a lot of people are doing that. If they’re having GI issues or skin issues, they want to get to the bottom of it.
What I hope to do in today’s episode is to clear up some of the myths about food allergies, so that we, whether you’re a dietitian or not, you can have a better understanding about what food allergies are and what they are not. If you do truly have a food allergy, what dietitians can do to help you, or if you’re a dietitian, what you can do to help your patients and clients.
[00:07:29] Melissa: Perfect. I love it. Just curious, the Dietitians On Demand podcast, when did that launch?
[00:07:34] Sara: We launched that in 2020, and we had a season of– I think our first season was eight episodes, but we really got serious about it in 2023. In 2023, we committed ourselves to releasing an episode at least every other week, and so that’s what we do now. Our episodes are a mix of clinical crash courses, is what I call them. We have an episode on how to wean a TPN, we have one on ECMO, we have one on Alpha-Gal. Things like that. Basically, everything you need to know about Alpha-Gal in 20 minutes or less. Then, we also have some career-focused episodes. One of our more popular options is the How to Negotiate a Salary episode.
[00:08:22] Melissa: I bet.
[00:08:23] Sara: Lots of dietitians have listened to that. I know that getting paid and getting paid more is always a very hot topic and of high interest with dietitians. We’re available, of course, on Apple Podcasts, Spotify, and a handful of other applications as well.
[00:08:40] Melissa: Okay, excellent. Let’s focus on the food allergies now. Maybe a good place to start would be to talk about the prevalence of food allergies.
[00:08:48] Sara: Incidentally, if you’re a dietitian, you probably feel like you’ve noticed an increase in the number of people who are reporting food allergies. The prevalence is around 6% of US adults and 6% of US children have food allergies, and that’s according to the Asthma and Allergy Foundation of America. The prevalence differs significantly, as I mentioned, between people who are just self-reporting that they have food allergies, versus people who have gone through actual testing, food challenges, and they have a diagnosed allergy.
Many dietitians, I’m sure, can identify with that, that you may hear from patients that they say– I’ve had patients tell me they’re allergic to artificial sweeteners. I’ve heard patients tell me they’re allergic to honeydew or all kinds of things. Anything is possible certainly, but there is just a huge discrepancy between our self-reported allergies and truly diagnosed. Most dietitians are familiar with the Big-8 food allergens. Just as a refresher, you have cow’s milk, egg, wheat, soy, peanuts, tree nuts, fish, and shellfish. As of 2021, there was a new major food allergy that was announced, and that was for sesame. A sesame allergy is estimated to affect around one million people in the United States.
[00:10:21] Melissa: Wow.
[00:10:22] Sara: In addition to the Big-8 that you’re probably familiar with, you may start seeing more patients and clients who are being tested or reporting an allergy to sesame.
[00:10:32] Melissa: Okay, great. I know we hear about these Big-8, and my understanding is even though they’re the Big-8, the prevalence is still quite low, but they’re the most common food allergies, correct?
[00:10:45] Sara: That’s right, yes. Of the 6% of US adults and 6% of children who are dealing with food allergies, their most common allergens are going to be the Big-8 that I mentioned.
[00:10:56] Melissa: Okay. You said anything’s possible. I remember, like I said earlier, I have a few related episodes, and one in particular on– Actually, a couple on peanut allergies, and one of those episodes is focused on the school environment. Not to get into the weeds on what schools are doing with regard to allergies and everything, but that’s when it dawned on me during that conversation with Sherry Coleman Collins, the guest on that show, is that we might be focusing on peanut allergies or any of these Big-8, but somebody could be allergic to a fruit or other foods, and so keeping our awareness that it could be other things.
I think there’s a false sense of security if we’re like, “This is a peanut-free zone,” but especially in the school setting, I think the staff needs to be aware of what the food allergy reactions are, which we’re going to talk about in a little bit. I didn’t know if you had anything to say regarding the other fruits or–
[00:11:51] Sara: No, just to echo what you said that don’t get lulled into a false sense of security, because when I was growing up, it seems like a lot of kids in my grade were allergic to strawberries. I don’t know if that was a again, if that was a self-reported thing or more of a actual diagnosis, but it seemed like that was a common allergy when I was growing up. I actually have a personal friend who she’s had eczema for many, many years, and she underwent some food allergy testing, which we’re going to talk about later, but the test results came back with a whole battery of food allergies. Actually, many of them were fruits. Fruits, vegetables, and plant-based ingredients in food.
Again, anything is possible. Just keep an open mind, and if you do have patients who are reporting any kind of issue, whether it’s GI or skin-related issue with any particular food, it can be really challenging to narrow down. It’s important that you follow the steps to go through the testing and the food challenges, which we’re going to talk about here in a moment.
[00:13:00] Melissa: Proper diagnosis, right? Yes, just personal side note, my son was born in 2008, so he’s 15 now. He’s got this core group of 8 or 10 friends that he’s grown up with. I would say, like four of them still carry EpiPens because they have a nut allergy. When you’re talking about the prevalence being 6%, and I know we’re going to get to this a little bit later with the latest research on reducing the risks, but I’m wondering if it was that period in time where maybe, and I don’t know if you’ve seen anything in the literature, maybe there was an increase in food allergies for a certain age population, that now we’re trying to dial that back with reducing the risks, which again, I’m teasing that. We’re going to talk about it a little bit later, but I just think it was so interesting.
[00:13:50] Sara: Were they actual–?
[00:13:52] Melissa: Diagnosed.
[00:13:53] Sara: Okay, got you.
[00:13:54] Melissa: Yes. I don’t know. Maybe it’s the bubble I live in, I don’t know. We’re going to talk about the pathophysiology a little bit. We don’t want to get too sciency for the non-healthcare professionals, but this does help explain what is a food allergy and what’s happening in the body. Walk us through that.
[00:14:11] Sara: Yes. A food allergy is different than a food intolerance. A food intolerance might be something like lactose intolerance, so you’re not allergic to milk, but if you drink milk, you may have some tummy upset, diarrhea, you just not be feeling well. With food allergies, it’s actually an immunological response. It’s your immune system recognizing this food and reacting to it. Food intolerances are not immune-mediated, meaning they don’t involve the immune system at all. That’s the main difference between a food allergy and a food intolerance.
Now with food allergies, these can be either what we call IgE-mediated. That stands for immunoglobulin E, or non-IgE mediated, or mixed. Basically, just keep in mind that there are three different categories. That’s really the take-home message here. Your IgE-mediated reactions, those are going to be your most typical and traditional food allergies and produce what you would consider a typical food allergic reaction, like having a rash, having your lips swell, having your tongue swell, things like that.
Your non-IgE and your mixed IgE mediated include food allergy-adjacent conditions. You have your eosinophilic GI conditions like eosinophilic esophagitis or EoE for short, atopic dermatitis, which is commonly known as eczema, and celiac disease. If you take celiac disease for an example, that’s not a true food allergy per se. If someone with celiac disease, they can eat wheat and gluten without stopping breathing or anything like that, but what we see is that they have damage in their GI tract that occurs.
Like I said, these are your food allergy-adjacent conditions. You’re still having the immune reaction, but it’s not your traditional allergic reaction like you would expect to see. Foods can be a trigger for these non-IgE or mixed IgE reactions, but they don’t have to be the only trigger. Like with EoE, eosinophilic esophagitis, sometimes environmental allergens can also produce a reaction for that condition, like pollen, pet dander, mold, stuff like that. Food is not necessarily the only trigger for those conditions
[00:16:59] Melissa: With the EoE, correct me if I’m wrong, but some of those symptoms could maybe be like reflux.
[00:17:06] Sara: Yes. EoE is almost like a very severe form of reflux. Again, it’s not going to be that traditional, “traditional allergic reaction.”
[00:17:17] Melissa: Like the anaphylactic.
[00:17:18] Sara: Right. You’re not going see the anaphylaxis, and you won’t see a skin rash or anything like that. It more happens internally when you’re having damage to tissues internally.
[00:17:30] Melissa: Maybe we could talk more about the different food allergy reactions because you’ve mentioned some, but maybe you could outline that for us.
[00:17:38] Sara: Yes, absolutely. These are going to be more of your classic food allergy reactions that would be associated with the IgE-mediated reaction. They can generally be classified into five different categories. Skin, that’s probably one of the more common ones you would think if someone eats like I gave the example of strawberries. Let’s say you’re allergic to strawberries. You have a strawberry, and within a few minutes, you develop a rash on your face, or you have redness on your skin, your lips or tongue start to swell, things like that, break out in hives. That’s going to be a skin reaction.
Respiratory is another category, and respiratory reactions typically don’t occur on their own. With respiratory, we’re going to be looking at things like shortness of breath, or the anaphylaxis, which is when your body basically goes into a state of shock. We can have cardiovascular shutdown, respiratory shutdown, things like that, associated with anaphylaxis. That’s a very serious reaction, but like I said, respiratory symptoms or reactions don’t typically occur on their own. They’re going to occur in conjunction with cardiovascular symptoms or a skin reaction, things like that.
The next is neurological. We don’t see this very often, but weakness, confusion, feel dizzy. In an extreme scenario, you may lose consciousness. Again, we don’t see that very often. Cardiovascular tachycardia, which is just a very fast heartbeat. Hypotension, which is low blood pressure, abnormally low blood pressure. Then cardiovascular collapse, so if your heart is struggling to beat or stop speeding. Typically, we’ll only see that with anaphylaxis.
Then finally, your GI. With the GI reactions, this is where the lines get blurred a little bit between a food allergy and a food intolerance because you can still have the nausea, the cramping, vomiting, abdominal pain, sometimes diarrhea with a true food allergy, but also, those are very common symptoms that we see with food intolerances as well. Again, I feel like a broken record, but just reiterating the importance of getting the official testing, meeting with the dietitian, and getting to the bottom of it essentially, as far as what food is actually causing your symptoms or maybe it’s not a food at all, and is it a true allergy or an intolerance.
[00:20:13] Melissa: Right, absolutely. Let’s talk about the testing and the process for proper diagnosis.
[00:20:20] Sara: Sure. I just want to preface this section by saying that there are tests out there. We’re going to talk about the specific types of tests, we’re going to talk about
some of the at-home test kits that you can get, but just keep in mind that these test results really don’t mean anything, unless you have a corresponding clinical reaction. I mentioned my friend earlier that had food allergy testing. I kid you not, she probably was allergic to 30 different things, according to the food allergy testing. She proceeded to start eliminating all of those things out of her diet, and so she was left with very little to eat. That is really what we don’t want to happen.
[00:21:04] Melissa: Right.
[00:21:06] Sara: Keep in mind that even if the test says that you’re allergic to X, Y, and Z, if you have a reaction to X, but not Y or Z, then you don’t need to eliminate Y or Z. That’s really important, I think, to keep in mind as we start talking about this or if anyone is on their own journey to trying to discover what their food allergies are.
[00:21:27] Melissa: Okay, great.
[00:21:29] Sara: The first type is a blood test, and the blood tests, all they do is just identify elevated levels of that IgE that I talked about earlier. This is not going to tell you that you’re allergic to anything specific. It just is going to let the clinicians know that there is an allergic environment present. Essentially, it just tells you that, “Hey, you’re having an allergic reaction to something. It could be food, it could be your cat, it could be mold in your basement, it could be anything,” but just letting you know that there is an allergic environment and there’s an allergic reaction taking place.
After you’ve get that blood test done really, that one can’t be a standalone test, so you need to go on a little bit further. There are a couple of options that you can take. A skin prick test is a pretty common one that a lot of people are familiar with, and you’ve probably known somebody who’s had this. Sometimes they do it on the back, they may do it on the arm.
They essentially are just inoculating the skin with either a real or a synthetic version of a food allergen and they wait to see if there’s a reaction. The skin will actually react it, it may get red, it may become inflamed or raised. That just indicates that there are a heightened number of these IgE molecules bound to mast cells. Now, again, not to get to sciency, but mast cells are a type of white blood cell, so that’s a part of your immune system.
Basically, what we’re doing is we’re just watching to see if the immune system reacts to any of these food allergens. Keep in mind that the skin prick test because it’s watching for the reaction of the IgE molecules, it’s not going to work well for the non-IgE or the mixed reaction like we talked about with celiac disease or EoE. Those are not going to jive with the skin prick test. The skin prick test won’t tell you anything about those conditions.
[00:23:39] Melissa: That make sense.
[00:23:39] Sara: That’s one option, and then the patch test is pretty similar. It’s a similar type strategy or technique with the skin prick test. You have the food allergens on a patch that’s applied to the skin. We leave it for two or three days, and then observe for any reaction or response. Again, these tests will probably come up with maybe some false positives. Meaning, they’ll report that you’re allergic to something when you actually are not. That’s why it’s important to follow up with a dietitian, an allergist, a medical professional, so that you can do a systematic food elimination challenge and actually, truly test whether you have a clinical reaction to each of these suspected food allergies.
I also want to talk a little bit about at-home tests. These are becoming much more prevalent. If you do an internet search for these, you will most certainly find several examples of at-home tests. These are just going to be tests that you can order from a website or you can purchase in the store. You can essentially test yourself for food allergies or food intolerance.
I want to mention that these are not a substitute for a physician-provided test, a physician exam, or a diagnosis.
Most of them use a blood sample, although, some will use a hair sample. With the blood sample, some of them use just a finger prick that you can do yourself at home. Then others require you to actually go to a lab and have your blood drawn professionally, and you send in that blood sample.
If you are thinking about using these options, we do have a couple of tips for you to try to get the best experience you can from these at-home tests. The first is to try to take steps to make sure that your sample that you’re taking and sending in is of good quality. If it’s asking a hair sample, make sure you follow the instructions as far as how to collect the hair.
They may not want just clippings off the end of your hair. Maybe they do, but just make sure you follow the instructions.
If you are doing your own finger prick to get a small blood sample, again, just make sure you’re following the instructions and you don’t have any contamination or anything with the sample. Also, I’d recommend that you do your research about the company itself, and specifically look for options, the kits that are processed in what’s called a CLIA certified lab. Basically, that just means they follow federal standards that the government has set out for laboratories who process human samples.
Also, just for your own safety and privacy, try to look to see if they adhere to any kind of privacy standards or HIPAA standards. After all, if you are sending in potentially your blood and your own personal medical information through the mail, so it’s always a good idea if you can verify as best you can that they’re going to keep your private information private.
[00:28:01] Melissa: Good point.
[00:28:02] Sara: Also make sure that your suspected food allergens are actually going to be tested by the kit. I mentioned strawberries, I’ll just keep using that example. If you think you might be allergic to strawberries and the test kit does not check for strawberries, maybe try to find one that does. Otherwise, you may be wasting your money and your time on something that probably won’t get you the answer that you’re looking for.
Finally, of course, beware of anything that seems too good to be true. If they’re using fear-mongering or villainizing particular foods, like it seems like the company is setting out to eliminate wheat in your diet or they’re setting out to try to get you to go gluten-free. Just be aware that that may not be as legitimate as some others. Like I said, if it sounds too good to be true, it probably is. Just keeping that in mind as you’re trying to select a company to do your at-home test kit.
[00:29:03] Melissa: That’s a great point. Yes, we often hear things like, “Oh, I’m going gluten-free, wheat-free, dairy-free.” The whole point is to not eliminate something that you don’t have to because as we know, we need a variety of foods to get all of our nutrients. When we start cutting out foods and food groups, it gets more challenging to meet our nutrient needs.
Speaking of diet and food, talk to me about these food elimination or food challenge diets or process. My understanding that it’s a temporary thing to try to figure out what you should be targeting and that it’s not so easy to just do on your own. I’m interested to hear your take on this.
[00:29:45] Sara: The food elimination challenges and reintroduction, like you mentioned, it can be really challenging for patients to do on their own. They are a really good follow-up step if you’ve had some testing done. Let’s say you’ve had a blood test and a skin prick test, or maybe you’ve done the at-home test, they can be a really good follow-up to that. Essentially, what the elimination part of it is, is let’s say you get your skin prick test and they report that you’re allergic to 10 different foods. That is probably going to be a little burdensome to try to eliminate all of those 10 foods for the rest of your life. Maybe we can determine if some of those are not a problem, that they are safe to consume.
The elimination portion of the food challenge, essentially what you’re going to do is totally eliminate all 10 of those potentially allergenic foods from your diet, and then you systematically introduce one at a time and see if you have a reaction. This can be really challenging because sometimes, depending on what you’re allergic to or what the food allergens are, they can be very prevalent in the diet and in our food supply. If wheat is one of them, wheat is in a lot of different things, and so that can be really challenging to eliminate and it can be challenging for patients and individuals to know what to eliminate.
Reading food labels and knowing how to read a food label and read an ingredient label, that’s going to be really important for this process because if there is even one iota of wheat that you forgot to eliminate, then we can’t really move forward and we can’t eliminate wheat as a potential allergen or we can’t confirm it either because we didn’t have an accurate elimination.
This process, this food elimination is also, typically, it’s going to be the first step in identifying your non-IgE or your mixed IgE reactions. Remember, those were the EoE or the celiac disease or eczema-type conditions, but we always follow that up with endoscopy. If you’re thinking about celiac, for example, if you suspect that you may have celiac disease and you’re having GI issues digesting gluten, sometimes people will eliminate gluten just to see if their symptoms improve, just incidentally, not very scientifically. If they do improve, then you still have to move forward and get that upper GI endoscopy so they can check out your intestines, take a biopsy, and get the true diagnosis. Doing the elimination challenge may be the first step in that process, just to again, narrow down what foods may be the culprit.
[00:32:47] Melissa: Is it still the case with celiac? I know we used to talk about if somebody did eliminate gluten on their own and then tried to get tested and diagnosed, that could impact the result?
[00:32:58] Sara: Yes, that’s a very good point. Let’s say you truly do have celiac disease. You’ve eliminated it from your diet before you’ve gotten an official diagnosis. That damage that we would typically see in the villi of the small intestine, the little finger-like structures in your small intestine, that damage can start to improve and recover. The tissues can start to recover once you eliminate gluten. If you have the scope after you’ve already eliminated gluten and you’re not seeing that damage in your intestinal tissues anymore, then yes, that can lead to a false negative showing that you don’t have celiac, when in fact you do. If “rule it out” with your endoscopy, go back to eating gluten, then your GI symptoms are likely to reoccur.
[00:33:47] Melissa: What else do we need to know about these elimination diets? How long do they usually take? I assume doing it with a medical professional like a dietitian who might specialize in this would be helpful.
[00:33:59] Sara: Yes, absolutely. Doing it with a medical professional, particularly a dietitian who can help you understand where these foods and where the allergens are located, how to read food labels, I know that that’s something that can be very challenging, so working with a dietitian or an allergist to move through that process. There’s also, like in the case of EoE, there’s more of a standard– With EoE there are six allergens that are very commonly associated with EoE food allergens. It’s common to eliminate those six and then you reintroduce two, and if it warrants it, then you reintroduce two more. There is more of this structured step-by-step with EoE compared to typical food allergies, so working with a professional is very important.
It can really take several weeks depending on how many potential food allergens you need to eliminate, how many you need to reintroduce. Just a word about the reintroduction, if you do suspect that you may have a severe reaction, like you may have difficulty breathing, your tongue may swell and you have difficulty breathing, swallowing, speaking, anything like that, the food reintroduction should take place under medical supervision. It should be done in the office of a dietitian, the office of your physician. Literally, they will just have you eat the food or drink whatever it is, the food allergen, and then just watch you to see if you are going to have a reaction and just make sure if you do have a reaction, they can intervene with medical intervention quickly and nothing serious happens.
[00:35:45] Melissa: Just curious, you mentioned the six more common allergens for EoE. I wondered if you could say a little bit more about that.
[00:35:52] Sara: Yes. For EoE, there is more of the stepwise elimination diet like I mentioned. They call it the Six-Food Elimination Diet, but it is actually all of the Big-8 food allergens. They just group fish and shellfish together and they group nuts and tree nuts together. With this elimination diet, you eliminate all of these allergens, all the Big-8 allergens for six weeks, then you reintroduce one food group at a time. You may start with wheat, you may reintroduce that first. Then, what actually has to happen with the EoE is you have to have another endoscopy after each food reintroduction-
[00:36:35] Melissa: Wow.
[00:36:36] Sara: -just to see if the inflammation has recurred, and if it’s visible and present, if there’s any damage to the tissue. If the inflammation has reoccurred and it is present, then you know that that is a trigger food. If it is not present, then that food is now a safe food to eat, and you can move on with reintroducing the rest of the food. In the case of EoE, it can be extremely time-consuming. Obviously, require a lot of medical tests going into the hospital. It’s a very involved procedure, so you definitely want to do it right the first time, if you can, and having the aid of a dietitian, or an allergist, or typically, with EoE, it may be a GI doctor. Having them to guide you through that process is going to be very important.
[00:37:30] Melissa: Okay, thank you. As we’re talking about the elimination diets or even just people just trying to avoid whatever they think might be causing problems, talk to me about the nutrition status or potential for deficiencies.
[00:37:45] Sara: That can become a real concern, especially when you have multiple foods or especially entire food groups that need to be eliminated. This is, again, why it’s so important to make the distinction between an allergy that is self-reported or suspected, versus one that’s actually diagnosed and confirmed. Make sure that you’re not just taking the allergy tests and taking those results at face value, you do want to confirm with a food elimination and challenge.
The nutrient deficiencies can involve both micro and macronutrients. That means vitamins, minerals, but also things like protein, maybe even fats would be impacted. For example, let’s say a young child has a cow’s milk allergy and they obviously can’t drink milk, can’t eat yogurt, cheese, things like that, so that is really going to reduce a major source of protein in a young child’s diet. Plus, obviously, calcium and vitamin D, during this period when they are rapidly growing in height or length and we have this rapid bone growth.
Even just with one big food group or nutrient that needs to be eliminated from the diet, we can start to see these micro and macronutrients. It’s important if you have a patient that has had to make significant changes in their diet that you’re talking to them about supplementation or what else can we give this child that would supplement calcium and vitamin D for them? Are they getting adequate protein, and those types of things. Just looking at the big picture and making sure that we’re meeting nutrient needs, even if it has to be in an unconventional way.
[00:39:34] Melissa: Great. Sara, I’d really love to dive into this topic about reducing the risk of food allergies. As I mentioned earlier, like with my son’s age, it seems like maybe the maternal diet or the infant diet may have had something to do with this higher rate amongst my son’s friends. I’ve been seeing a lot more about early introduction of certain foods. Like I said, I have a podcast interview on early introduction of peanuts or peanut foods. Obviously, with a small child, you don’t want to give them nuts because they could choke. Just want to clear that up. Also, I understand with the new dietary guidelines, we might be seeing some guidance on early introduction of foods. I don’t know much about this, but I would love to hear what you’ve been seeing in the research and practical applications.
[00:40:28] Sara: This is a really interesting topic because like you said, with your son being born in the early 2000s, there was a belief at that time that children, we should avoid introducing food allergens too early. We should delay it because we don’t want them to develop food allergies or have a serious reaction. Now that conventional wisdom has really been reversed, and now the push is more for early introduction of food allergies, and the recommendations that are out there from the American Academy of Allergy, Asthma, and Immunology, plus its European counterpart, plus the American Academy of Pediatrics also recommend all three of these organizations, recommend introducing specifically peanuts and again, not the specific peanut, but a peanut food and then cooked egg between the ages of four and six months, which would be around the age that you would be introducing solid foods to a baby anyhow.
Peanuts in an appropriate baby friendly form and cooked egg should be introduced fairly early on around the time that they’re starting to take solid food. There’s also, they have put out some information about what the mother should be consuming during pregnancy and if mom is breastfeeding, if that has any effect. They say there’s no evidence to delay the introduction of allergenic foods to baby. There’s no evidence that you should be avoiding consuming allergenic foods if you’re pregnant or if you’re breastfeeding.
In fact, breastfeeding can actually have a little bit of a protective effect for children, for babies, particularly at reducing the risks of allergenic conditions like eczema and wheezing. If you are breastfeeding, there can be an additional perk to potentially reducing the risk of these food allergy adjacent conditions. The American Academy of Allergy, Asthma, and Immunology, they have some guidance, which we’ve actually linked in the show notes if anyone wants to read this document in full.
They have given some advice on how to introduce some of the Big-8 food allergens in age appropriate ways. Because again, a baby probably wouldn’t be interested in eating soybeans or can’t eat a Brazil nut or anything like that. How can we actually introduce some of these foods in a baby friendly way? For soy, for example, we can try baby soy milk, we can try soy yogurt. Babies and young children typically like yogurt or even tofu.
You can even mix these ingredients in other foods. That’s another way to introduce the food allergens. If they are not interested in tofu, you can make something that has tofu in it. That could be a way to introduce that food item. Then, for wheat, for another example, they recommend something like softly cooked pasta, so like a macaroni noodle or penne pasta noodle, something like that. Baked goods like pancakes or even low sugar cookies. If you cut up a pancake into bite-sized pieces, let baby have pancake. That’s a good way to introduce wheat and see what the reaction is. Again, it’s just not the conventional wisdom that we’ve always heard.
[00:43:57] Melissa: Right.
[00:43:57] Sara: I think in dietitians or other clinicians who are listening, it’s okay to tell your parents that they can give baby these potentially allergenic foods. Just do it one at a time and make sure you’re watching for any type of reaction.
[00:44:13] Melissa: Great. Like you said, we’ll link to those resources in the show notes. That’ll be very helpful. Yes, when I first heard about this idea, it seems so counterintuitive, but it’s so fascinating to see the research on this, and it makes sense in a way. [chuckles]
[00:44:29] Sara: I’ve heard the same thing related to pets. Babies that grow up in a household with pets, they tend to have less instances of asthma or environmental allergies. There must be something to it that having that early exposure. I don’t know.
[00:44:45] Melissa: Produces a healthy immune system.
[00:44:48] Sara: Absolutely.
[00:44:48] Melissa: Hopefully, a good gut microbiome too.
[00:44:50] Sara: Probably. [chuckles]
[00:44:51] Melissa: Before we wrap up, I’d love to hear more about the role of the dietitian in this process. We’ve talked about that a little bit so far, but maybe just emphasizing how dietitians can or should get involved.
[00:45:04] Sara: Yes, absolutely. Melissa and I are both dietitians, so we’re always pro dietitian and like I said in my introduction, I grew up in my dietitian training to be a dietitian who’s more involved and tries to be more involved. I personally think that dietitians should get involved, particularly when you have a patient who has multiple confirmed food allergies. If you’re eliminating more than one food group or several food items, really, you need to start thinking about talking with a dietitian because just learning how to read food labels is a thing in and of itself, but even making sure that you’re meeting all your nutrient needs, your vitamin and mineral needs, fiber, and you’re getting all these essential nutrients that your body needs when you can’t get them from conventional sources. That should be a concern and a time that you need to seek out help from a dietitian.
Also, if you have an infant or a very young child with food allergies, that can also be very challenging, especially when trying to navigate baby formula or how to introduce foods. Or let’s say, you’ve started to introduce foods and baby had a reaction, and now you’re scared to introduce other foods. That would be a good time to talk with a dietitian and try to more systematically or strategically introduce some of these food items in a safe way. Sometimes nutrient supplementation may be necessary. Again, speaking with a dietitian about what that actually looks like and how you can do it in a safe and affordable way. Then also, sometimes we have complex cases where there are other comorbidities present. Celiac disease and type 1 diabetes tend to happen frequently together.
[00:46:54] Melissa: That’s right.
[00:46:55] Sara: Those can be very difficult conditions to manage on their own, but when you put them together and you’re talking about it happening with a young child, that can be very challenging for the child. It can make them feel very alienated and alone, like at school or birthday parties because they can’t participate fully. If you have a child who maybe has texture aversions, if they’re on the autism spectrum maybe and they have texture aversions. Other GI issues, like maybe Crohn’s disease. You’re trying to balance fiber or what have you. Then, if you have a patient who’s receiving tube feeding, that can be really challenging as well because a lot of our tube feeding formulas are just standard formulations, and you can’t necessarily take out the soy protein isolate. If you have a patient who’s allergic to soy, what do you do?
Those are all situations where dietitians can be very valuable and good sources of knowledge and helping their patients navigate those situations. I just want to wrap up by saying hopefully, this was a good episode to learn a little bit more about food allergies and get the facts about food allergies, and just know that there is a lot of misinformation out there about food allergies. It seems like food tends to be the culprit a lot of times when people have various issues. Food is an easy thing to blame, and so as dietitians, we should get out there and educate the public, but also just our fellow colleagues about food allergies and early introduction of food allergens because I think that is a very important role for us to play as well.
[00:48:38] Melissa: I agree 100%. Thank you so much. If people want to find out more about this topic, like I said, we’ll have some links in the show notes if there was anything in particular you wanted to point out that you already didn’t mention. Also, Dietitians on Demand, you’ve got a lot of great resources there. You can share the website link, a URL, and I’ll put the links in the show notes at soundbitesrd.com.
[00:49:01] Sara: Yes. In the show notes, you’ll actually see a link to some of the research articles we talked about. Then also, I included a link to, it’s like a little flow chart actually for the elimination diet and oral food challenge protocol. If you are a dietitian and you need to help a patient through that, you can download a free copy of that in our store. We’ve linked that in the show notes, but visit us on our website, dietitiansondemand.com, or you can see all of our resources in our store, which is shop.dietitiansondemand.com. Yes, thank you, Melissa, for having me. It’s been wonderful to talk with you today.
[00:49:38] Melissa: It’s been great having you on the show. I encourage people to check out the podcast as well. It’s dietitians only, but I’m sure anyone can tune in. I know on my show, it’s a mixture of the general public and health professionals. I encourage people to check that out. Thanks again, Sara.
[00:49:55] Sara: All right, thanks, Melissa.
[00:49:57] Melissa: For everybody listening, as always, enjoy your food with health in mind. Till next time.
[00:50:04] Speaker: For more information, visit soundbitesrd.com. This podcast does not provide medical advice. It is for informational purposes only. Please see a registered dietitian for individualized advice. Music by Dave Burke, produced by JAG in Detroit Podcasts, copyright Sound Bites, Inc. All rights reserved.
[00:50:31] [END OF AUDIO]
LISTEN, LEARN AND EARN
Listen to select Sound Bites Podcasts and earn free CEU credits approved by the Commission on Dietetic Registration (CDR) for registered dietitian nutritionists and dietetic technicians, registered. Get started!
Get Melissa’s Sound Science Toolkit here!
Partnerships:
Sound Bites is partnering with the Association of Diabetes Care and Education Specialists (formerly the American Association of Diabetes Educators)! Stay tuned for updates on the podcast, blog and newsletter!
Sound Bites is partnering with the International Food Information Council! Stay tuned for updates on the podcast, blog and newsletter!
I find it irresponsible that this episode recommends the use of at home food sensitivity tests. These are not clinically approved or appropriate as a “place to start” for anyone.
Hi Lauren,
Thank you for listening to the podcast and sharing your comment. To clarify, we agree that these tests should not be used to replace an official physician-provided test and subsequent medical diagnosis, as the guest, Sara, mentioned in the episode. We wanted to address the use of at-home tests because many people are using them.
This is an article that discusses the issue further: https://www.medicalnewstoday.com/articles/food-sensitivity-test#faq and includes this statement: “The American Academy of Allergy, Asthma & Immunology states that at-home food allergy tests may not provide accurate results. It warns that using alternative testing such as IgG testing, home allergy test kits, skin titration and applied kinesiology. If a person does take an at-home test, they should follow up on any positive results with a doctor.”
We feel that Sara shared this information during the interview but we will consider adding some more information in the shownotes and perhaps the episode itself to clarify this further.
Thank you,
Melissa
Sign up for my monthly newsletter and episode eblasts so you never miss an update!
Listen on Stitcher (Android)
Install the Stitcher App
1. Search for “sound bites with melissa joy dobbins” 2. Choose Play Current Episode or Add to Playlist
Choose “Play Episode”
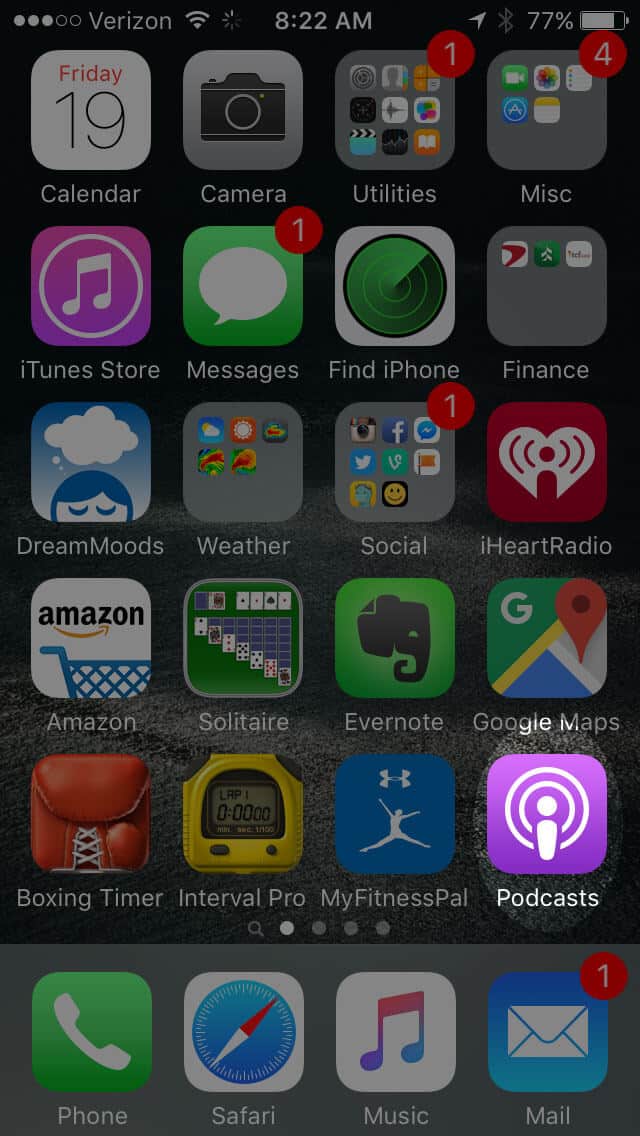
Subscribe & Review on iPhone
Open the “Podcast” app on your iPhone
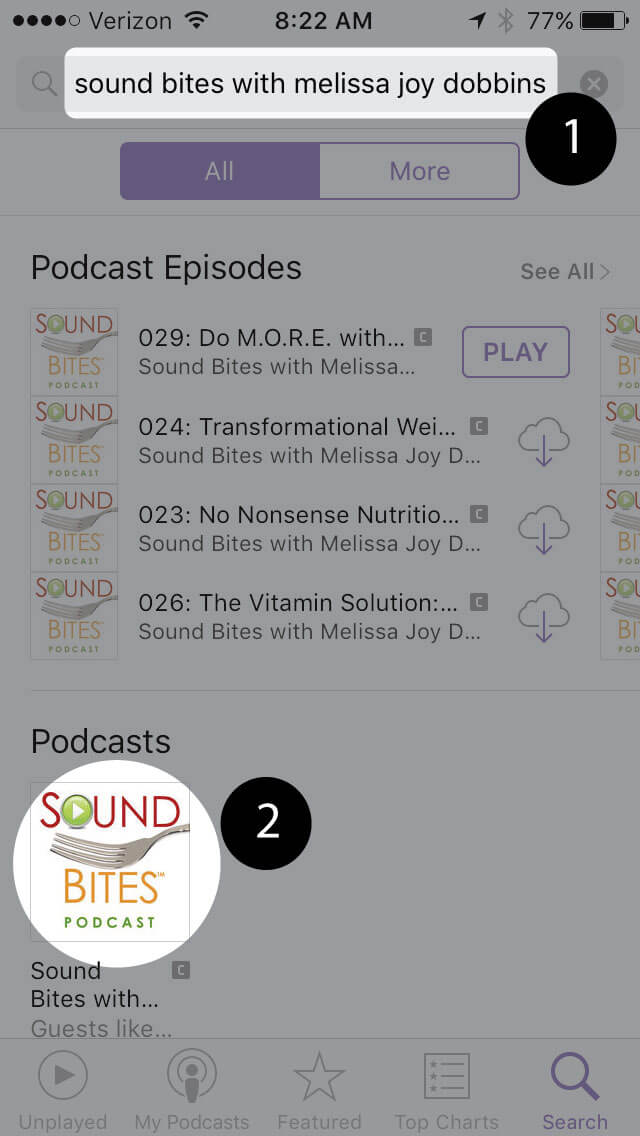
Search for “Sound bites with melissa joy dobbins”
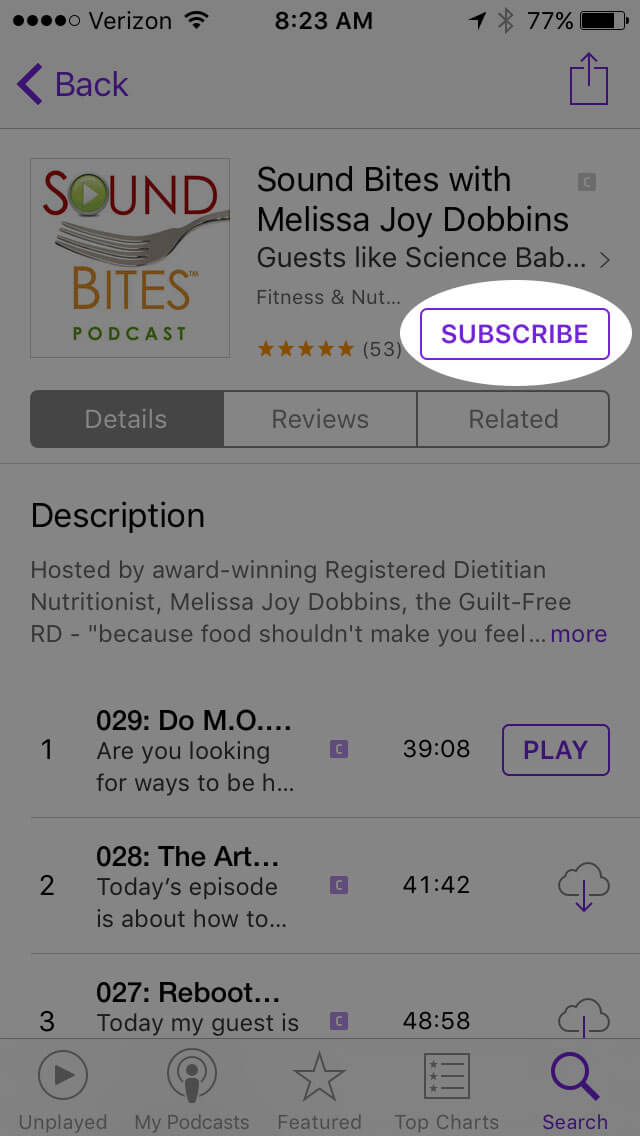
Open the podcast and click “Subscribe” and your done!
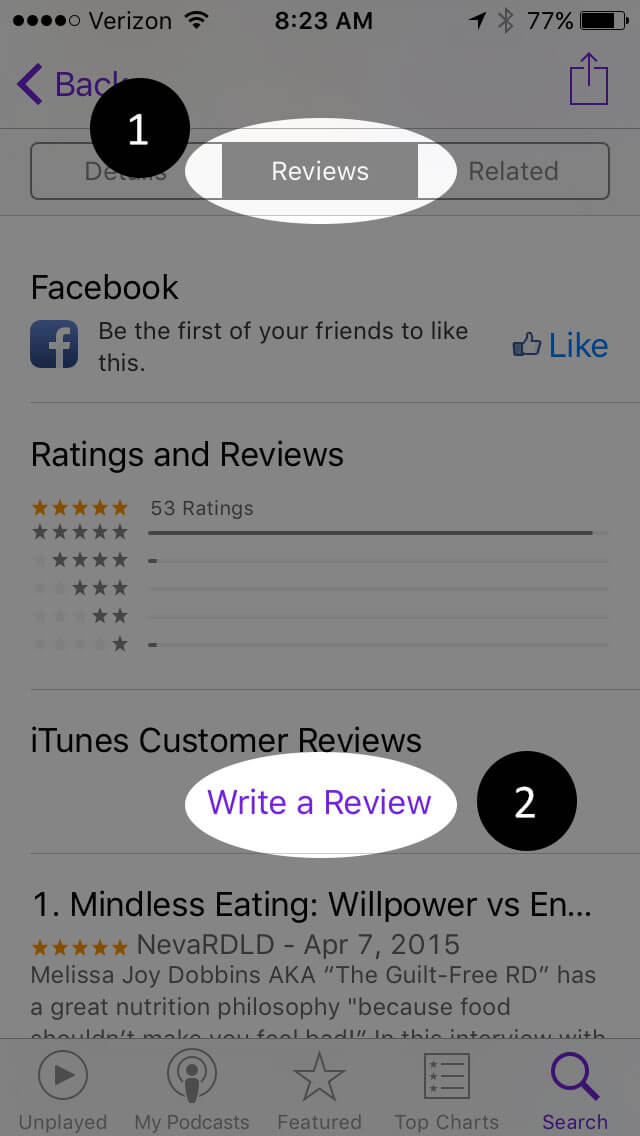
Write a Review
Click “Reviews”, then “Write a Review”.
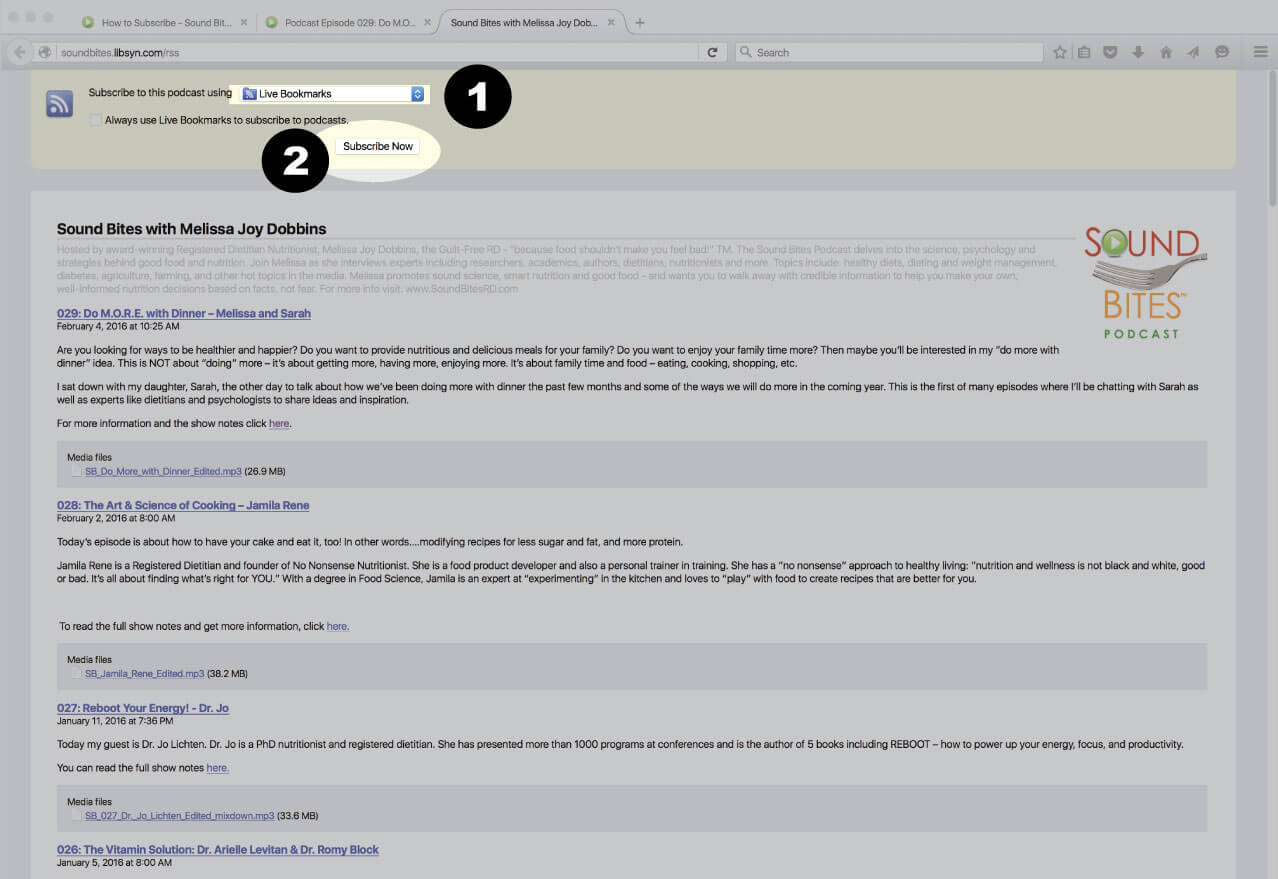
Subscribe via RSS Feed
Navigate to any podcast player . Click on the RSS feed icon.
Click on the RSS feed icon.
Click on RSS Feed
Choose which application you would like to use to receive the RSS feed
Click “Subscribe Now”
Confirm settings and subscribe.
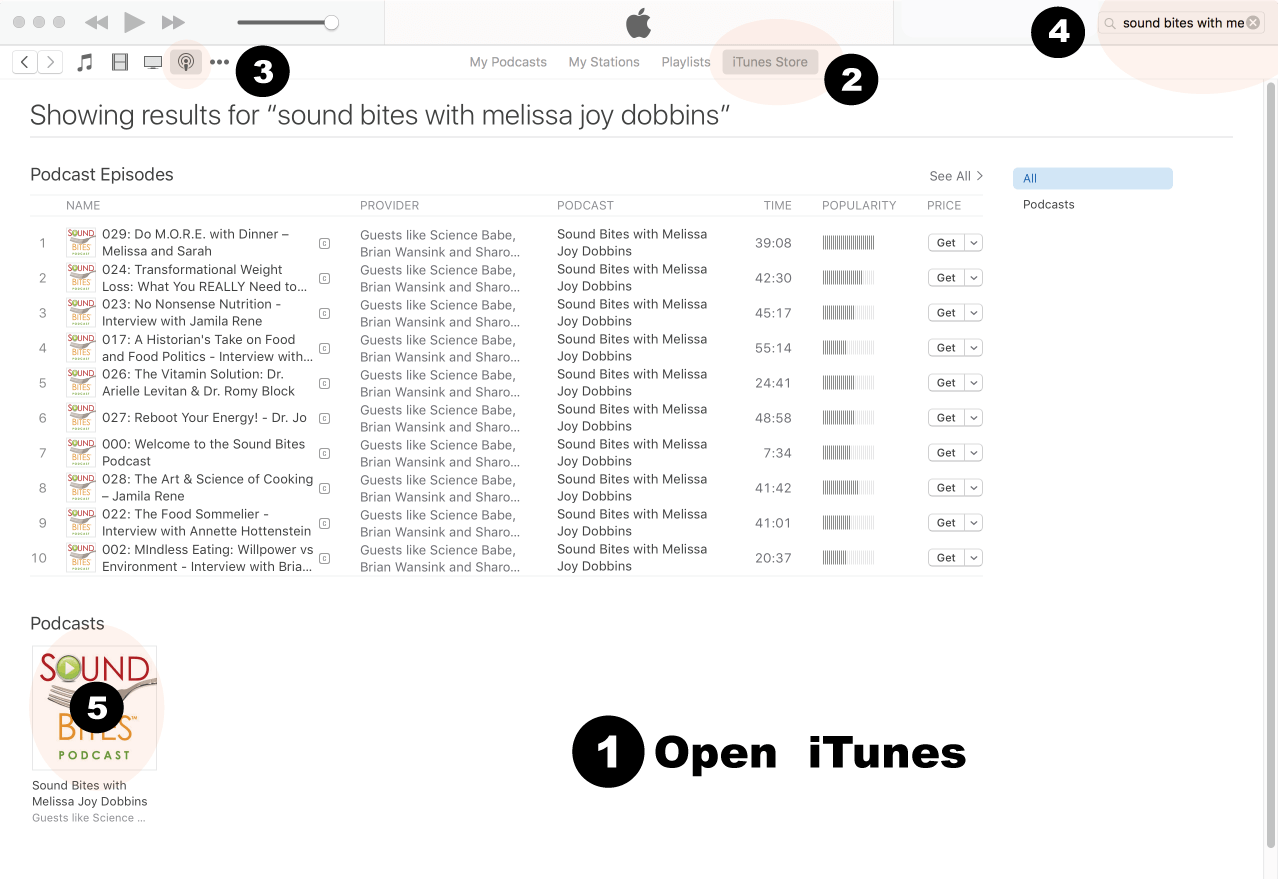
How to Review in iTunes
Open iTunes desktop application
Click iTunes Store
Click on Podcasts
Search for “Sound bites with Melissa Joy Dobbins”
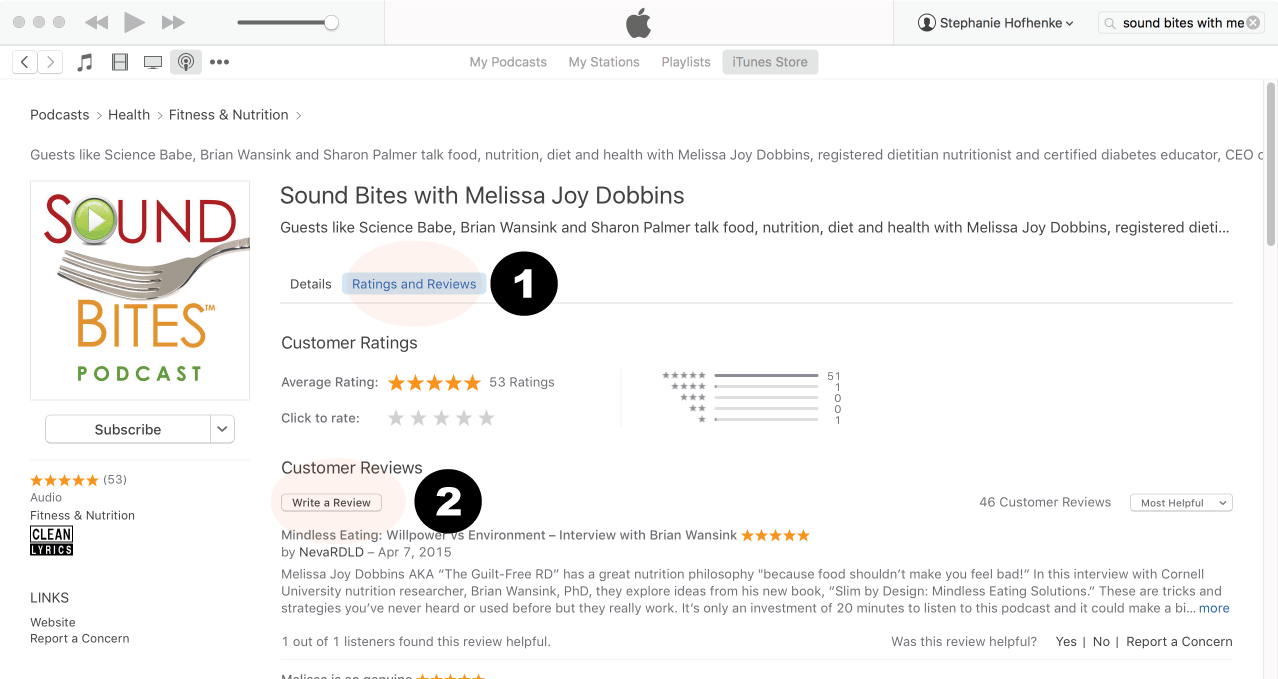
Click on podcast image
Search for Sound Bites podcast in iTunes
Click Ratings & Reivews
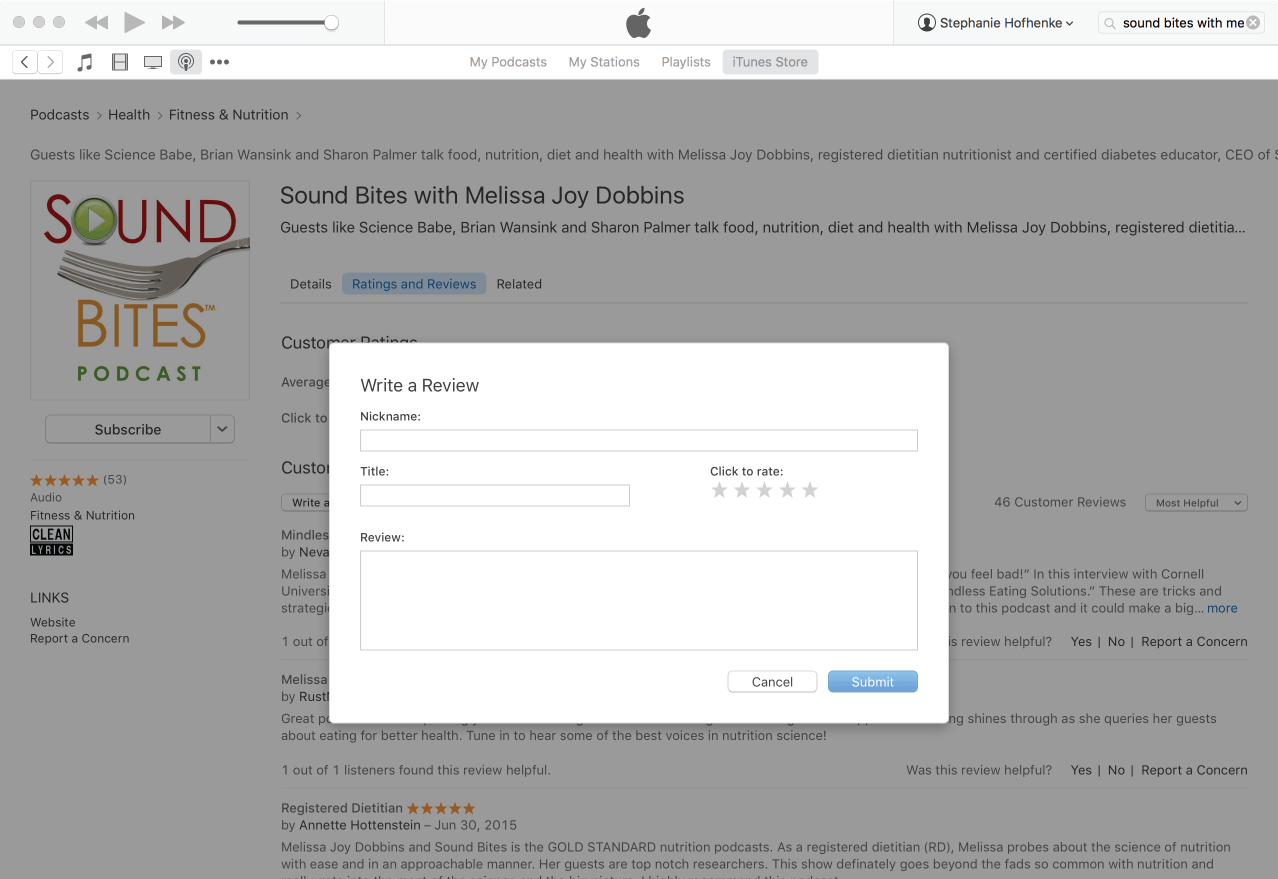
Click Write a Review
View reviews and write your own review.
Write your review…. Thank you!
Write your review!
How to subscribe via iTunes
Click here to view the Sound Bites Podcastin iTunes, then click the blue “View in iTunes” button. This will open your iTunes application directly to Sound Bites Podcast. Click the “Subscribe” button, and your done!













I find it irresponsible that this episode recommends the use of at home food sensitivity tests. These are not clinically approved or appropriate as a “place to start” for anyone.
Hi Lauren,
Thank you for listening to the podcast and sharing your comment. To clarify, we agree that these tests should not be used to replace an official physician-provided test and subsequent medical diagnosis, as the guest, Sara, mentioned in the episode. We wanted to address the use of at-home tests because many people are using them.
This is an article that discusses the issue further: https://www.medicalnewstoday.com/articles/food-sensitivity-test#faq and includes this statement: “The American Academy of Allergy, Asthma & Immunology states that at-home food allergy tests may not provide accurate results. It warns that using alternative testing such as IgG testing, home allergy test kits, skin titration and applied kinesiology. If a person does take an at-home test, they should follow up on any positive results with a doctor.”
We feel that Sara shared this information during the interview but we will consider adding some more information in the shownotes and perhaps the episode itself to clarify this further.
Thank you,
Melissa
Very good ,such a brainstorming session for allergy chapter
Sania,
Thank you! So glad you found it helpful!
Melissa