Celebrating over 1 Million Downloads and 50,000 Free CEUs on the Sound Bites® Podcast | NEW: Get 1 years’ worth of CEUs with the new 15-CEU Podcast Course
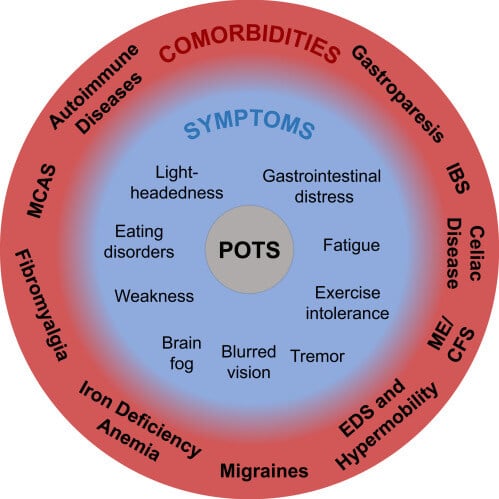
Postural Orthostatic Tachycardia Syndrome, or POTS, is the most common type of dysautonomia – a dysfunction of the nerves that regulate nonvoluntary body functions such as heart rate, blood pressure and sweating. POTS is characterized by symptoms in multiple organ systems and an abnormal increase in heart rate upon standing. Because POTS affects multiple organ systems, patients report a wide range of symptoms with approximately 90% reporting gastrointestinal distress. Front line management of POTS is diet and lifestyle, however medications may also be indicated.
Tune into this episode to learn about:
Current research on dysautonomia and POTS
Why POTS is often misdiagnosed and underdiagnosed
Why POTS is associated and confused with anxiety, eating disorders and other
The link between the autonomic nervous system and digestion
Dietary considerations and recommendations including salt/sodium and fluid intake
How some patients show a worsening of symptoms with high glycemic foods
Importance of screening for eating disorders
Managing digestive issues
Exercise recommendations
Cheryl’s story and “Miss E’s” story
The lack of funding of diseases based on gender disparity
POTS is a common, yet commonly overlooked, autonomic nervous system disorder that is easy to confuse with an eating disorder. Typically misdiagnosed and underdiagnosed, the onset of POTS is often post-viral, so we are seeing a significant increase due to COVID-19.” – Cheryl Harris
Cheryl Harris, MPH, RD
Cheryl Harris, MPH RD is a private practice dietitian specializing in digestive disorders for the past 15 years. She was recognized as one of the top nutritionists in the DC metro area by the Washingtonian and was selected as the “Emerging Dietetics Leader of the Year” for Virginia for 2012. She has presented widely on nutrition for the Virginia Academy Annual Conference, Maryland Diabetic Association, the Institute of Medicine, Villanova and more and taught the Academy’s Certificate of Training in Gluten-related disorders released in 2021. Her articles on nutrition and courses appeared in Today’s Dietitian, Simply Gluten-free Magazine, Gluten-free Living, Gluten Intolerance Group, and numerous DPG newsletters. She has been quoted by many media outlets, including the Washington Post, ABC.com, WebMD, Cosmopolitan, Prevention, the Food Network, and the Washingtonian.
Welcome to Sound Bites – hosted by registered dietitian nutritionist, Melissa Joy Dobbins. Let’s delve into the science, the psychology and the strategies behind good food and nutrition.
[00:00:00] Melissa: Hello and welcome back to the Sound Bites podcast. Today’s episode is about postural orthostatic tachycardia syndrome or POTS. It’s a common, yet commonly overlooked autonomic nervous system disorder that is often misdiagnosed and undiagnosed, and it has dietary and digestive aspects. And we’ve seen a significant increase in POTS due to COVID.
My guest today is Cheryl Harris. She’s a private practice dietitian based in Fairfax, Virginia, specializing in digestive disorders for the past 15 years. She has a Master’s in public health and was recognized as one of the top nutritionists in the DC metro area by the Washingtonian, and selected as emerging dietetic Leader of the Year for Virginia in 2012.
And I will also be submitting this episode for one free continuing Education credit through the commission on dietetic registration for registered dietitian nutritionists, dietetic technicians registered and certified Diabetes Care and education specialists. For more information, you can visit my show notes or my ceu page @soundbitesrd.com, and I have over 40 free CEUs at that page, so definitely want people to check that out.
Welcome to the show, Cheryl.
Thank you for having me.
I’m really glad to have you on this episode. I am fascinated in the work that you do and this syndrome called POTS. But before we dive into this, I would love for you to share more about your background. Perhaps why you decided to study nutrition in the first place and digestive disorders specifically?
[00:01:42] Cheryl: Well, I have always been interested in nutrition and when I say always, I mean from when I was a child, I was interested in nutrition. I come from a Middle Eastern family, and some of you may know in a Middle Eastern family, it is all about the food.
So, that was basically just how I was raised. So food has always been an area of fascination and passion. I didn’t intend really to go into digestive disorders until I actually had digestive disorders myself. I intended to go into public health because I was a public health nutritionist. That was what I studied.
I intended to serve underserved populations, except when I developed digestive disorders, what I realized was that digestive disorders were underserved populations, and so I went from running the breastfeeding programs for DC WIC and thinking that was what I was gonna do and work with underserved populations in the heart of DC to really redefining what underserved populations were and going into private practice and working with the digestive disorders there.
[00:02:52] Melissa: Now, you recently published your research on POTS and I saw your post on Twitter about it, and I, I love meeting people like you on Twitter. It’s wonderful. But your post caught my eye partly because a friend of my family had been diagnosed with POTS several years ago, and I had never heard of it. And when she mentioned that she could or couldn’t eat certain foods, that’s when I really thought, Wow, I’m a dietitian and I don’t know anything about this. And I didn’t wanna pry or ask her a lot of questions, so I didn’t think much of it at the time. But when I saw your post and how misdiagnosed and undiagnosed this is, I reached out to you and I said, Hey, would you like to come on the podcast and talk about this?
And since then I’ve learned a lot more from you. And I reached out to that family friend and asked her to share her story with me, and it was so compelling and very upsetting when I heard some of the details of what she experienced. I know you can share your story as well dealing with POTS, but let’s start with what is POTS and why are we hearing more about it these days?
[00:04:03] Cheryl: Yeah, and first of all, I just really wanna thank you so much for being willing to highlight POTS on your show. As you mentioned in the beginning, POTS stands for Postural Orthostatic Tachycardia syndrome, and what POTS means in a nutshell is when someone goes from a sitting or lying down position to an upright position, there’s an excessive increase in heart rate, and for someone who’s a teenager, that’s an increase in 40 beats per more per minute. Or for someone who’s an adult, it’s 30 beats per more per minute. Essentially what that means is the heart is working too hard, harder than it should be to keep blood flow to the brain, and that can cause all sorts of unpleasant kinds of symptoms.
There could be lightheadedness that could be tachycardia or excessive heart rate. There can be brain fog. It just all sorts of unpleasant kinds of things. Dizziness, fatigue, all sorts of GI kinds of symptoms as well can come along with it. But the other problem with those kinds of symptoms are kind of vague symptoms and so they can be mistaken for other sorts of things.
Part of the reason, in terms of your question, of why we’re hearing so much about POTS now is that POTS is often a postviral condition, and of course COVID, it’s a virus. And so many people are getting POTS now as a result of having COVID. And so we don’t know exactly how many people have POTS now because there aren’t great numbers, but it’s very clear that the number of people who both have POTS and dysautonomia, which is the umbrella that POTS fall under, have increased greatly as a result of the pandemic.
[00:05:57] Melissa: Right. I have a press release from the Dysautonomia International organization that says – this is from April. It says, An estimated 38 million Americans have developed an autonomic nervous system disorder following COVID 19. and it talks about how 67% of individuals with long COVID are developing this dysautonomia.
And as you said, POTS is one of the conditions underneath that umbrella. And, I had learned from you and you just shared that it can often have an onset after a viral infection. I also understand that it affects women more than men, a four to one female to male ratio.
Talk to me a little bit about the age, demographics and, the people that we’re seeing this affecting most often.
[00:06:50] Cheryl: So we understand the ages and the demographics very well for POTS prior to COVID, so that’s what I’m gonna talk about. We don’t really understand whether that’s changed in terms of how COVID has changed that.
So I’m gonna talk about the numbers prior to COVID, knowing that, you know, for long COVID POTS, some things may have shifted. So for numbers prior to COVID, there was the four to one leaning of female to male, and that it was generally people 12 to 50 that generally got POTS, even though it was generally in teens and 20 somethings who developed POTS.
Those were generally the people who were developing POTS. And the numbers also suggested that it was generally something that was diagnosed in white women even though I always give a caveat when I cite those figures, I don’t think that POTS had kind of like a racial leaning in that there was some sort of discrimination where people of color didn’t develop POTS as much as people of color often just didn’t get diagnosed.
I think it was more of an access issue versus that somehow people of color were protected against developing POTS.
[00:08:01] Melissa: Great point. Yes, and that’s one of the many issues with this syndrome. And we’re gonna touch on as much of that as we can during this conversation. Talk to me a little bit more about the symptoms, because this is a syndrome and it has a bunch of different symptoms and some people with POTS don’t have GI distress or GI symptoms, some people do, but run through the symptoms again and connect the dots with why this is so underdiagnosed.
[00:08:31] Cheryl: Sure. So common symptoms are things like lightheadedness, increased heart rate, brain fog, dizziness, fatigue. And 90% of people do have GI symptoms. There are also common issues that come along with POTS.
Those are things like IBS, joint hypermobility syndrome, which is also known, can be known as ehlers-danlos syndrome, migraines are very common. Autoimmune disorders are very common. So there are many things that come along with it that aren’t exactly symptoms of POTS, but they are often part and parcel.
[00:09:10] Melissa: Coexisting.
[00:09:12] Cheryl: The other piece is that there isn’t a better explanation. So, some of the things like lightheadedness and brain fog and dizziness and fatigue can just be if someone’s not eating, so that isn’t a better physiologic explanation, like anorexia. . . So there needs to be no better explanation for the symptoms.
[00:09:31] Melissa: So part of the diagnostic journey is to rule out other things. And one of the reasons we’re having this conversation is because a lot of healthcare professionals are not aware of this. A lot of dietitians are not aware of this, like myself. And, I believe you had told me when we talked earlier that it wasn’t even taught in medical school until the 2000s.
[00:09:52] Cheryl: Yeah, so the very first times that it was discovered anywhere was in Mayo Clinic, and that was in the late nineties, but the very first official conference on POTS, the first formal conversation was in 2019. There was an NIH conference on POTS to formalize many of the different definitions, 2019!
Wow.
And that just lets you know that even though it’s been around for a long time, or you know, 20 years, that’s not a very long time. Many doctors really didn’t learn about it in school. So it is very, it’s been historically underfunded. Many doctors aren’t aware of it. And one of the things that’s a great frustration to me, I still hear many doctors quote unquote, don’t believe in it.
And it is a condition that has objective markers. It’s not a religion. It’s not something that people should quote unquote believe in. They’re objective physical markers. It’s not . It’s not a matter of belief like the same way anemia isn’t something you believe in. It’s just objective physical markers. This shouldn’t be a matter of belief.
[00:11:05] Melissa: Right. And because of this orthostatic tachycardia and blood pressure, blood volume is involved. Talk to me about some of the diagnostic tests that can indicate that we’re looking at POTS.
[00:11:18] Cheryl: Absolutely. So what they do is they have someone lie down and they take their heart rate.
And then they have them go to a standing posture and they take their heart rate and they measure heart rate for the next 10 minutes. And they compare those different heart rates. And there’s the different cutoffs for adults and children. When you have a more in depth center, they can do more in depth testing, like tilt table tests, and more in depth testing can be done to differentiate between POTS and other forms of Dysautonomia.
[00:11:53] Melissa: Okay. Am I correct in saying that once there is a diagnosis, there’s no cure, but there are treatments and oftentimes it’s managing the symptoms, but diet and lifestyle management is considered the first line of treatment, which we’re gonna talk about more in depth in a little bit. But there’s also other treatments, medications, and so on.
[00:12:13] Cheryl: Yeah, so while diet and lifestyle is frontline, there are a range of medications, diet and lifestyle and exercise. But there are a range of medications. While diet and lifestyle is important, medications can be critical as well.
[00:12:26] Melissa: Okay, so before we get into some of the specifics about the diet, I mean, would you like to share your story?
And I do have permission from my family friend to share some of her experience.
[00:12:39] Cheryl: I’ll share my story and I’ll try to share the condensed version. I’ll mainly try to share the parts that overlap with what many people have experienced, I got the package deal because everything hit at once. So what many people can relate to is I was the kid that drank pickle juice.
I always craved salt as a child. I was always the kid that passed out at track meets that passed out at concerts that passed out at like choral events. Always as a child, whenever it was hot, that was me fainting in the corner. So, so I always had a tendency toward, if it was hot.
I was fainting. and sometimes just fainting for a minute. And other times, like, someone would find me on a path and have to carry me somewhere. So.,
[00:13:27] Melissa: oh my gosh.
[00:13:27] Cheryl: So, You know, out cold somewhere. It didn’t end up being a major issue until grad school where I was given a medication that affected my heart rate.
And that was what really made my POT’S symptoms a huge issue, and it took months because I didn’t know what was wrong, and all of a sudden I had this pounding heart rate. And generally my resting heart rate was, you know, 120, 130, 140. And when I would take my heart rate and realize, Oh my God, my heart rate is racing, I would get really anxious because it was like, Oh my God, there’s something wrong with my heart and I have no idea what’s wrong.
And I would go to the doctor and they would be like, You’re just anxious. And it would be like, . . Nope. No, that doesn’t make any sense. And I was really lucky that some really smart NP was just like, Get off this medication. And I did. And I still, like, I couldn’t go in hot tubs. Like I would still have some tachycardia, but things calmed down for a couple years until I got a tick bite. Then kind of all hell broke loose. I went, and many people will also be able to relate to this, so I went from being healthy hyper mobile to expressing ehlers-danlos, which is a very common comorbidity. So in terms of people with POTS, a quarter to a third of people with POTS do have ehlers-danlos or joint hypermobility syndrome.
So I’m kind of one of those lucky people. So I had profound joint pain and for me, it affected my feet and my shoulders most. So I was actually to the point where I couldn’t walk. So I just all of a sudden having, like I went from someone who qualified for the Pan Am games, and here I was not able to walk and having these, you know, profound GI symptoms to the point where I was in the bathroom 20 times a day and lost 40 pounds. And so nobody even really noticed the POTS symptoms because it was sort of like, all symptoms, lights flashing, like something is wrong. I was going to all these doctors and so I absolutely always felt better when I was lying down.
I would always, when I was working, always have to take calls lying down. I knew I only felt good when I was lying down. It was really clear that I had terrible brain fog. I couldn’t remember things, but as soon as I lied down, my symptoms would calm down. But nobody ever asked about that. It actually took five years to diagnosis.
And then when I was driving, there were a couple times that I felt really lightheaded and I had to pull over and I fainted in the car a couple times. Scary. Yes. Very scary. That earned me a trip to the cardiologist. I still wasn’t formally diagnosed with POTS, but he was really clear that my answer was potato chips.
And, I know my husband said it was worth taking a day off just to see my face because I said it was like potato chips. And he’s like, Yeah, potato chips a big bag. and I was just like, I don’t understand. Just tell me like how much sodium. He’s like, No, no, no. Just potato chips. And I was like, But isn’t there, Like, can’t you just tell me how many grams of salt?
And he’s like, No big bag, and drink it with a whole lot of soda. Oh. So this sort of blew my mind, but at least I understood that the answer was salt and fluid. So not a big fan of his answer or how he gave it. But I understood that the answer was salt and a lot of fluid. You know, I didn’t faint after that because I started being very careful about salt consumption and fluid consumption. . . So I don’t know whether he understood what was going on or whether he didn’t – clearly to some extent he understood, but bedside minors and communication skills not so much.
[00:17:33] Melissa: Right. And I’m sure that’s pretty common. You mentioned that it was about five years before you were diagnosed and this press release that I have, That prior to COVID, and we are, you made this point, and we wanna keep clarifying this as we talk.
There are some things about POTS prior to COVID that are true or what they are, and then there are some things that are different with long COVID POTS and you’re gonna detail more of that, as we talk. But prior to COVID, the average diagnostic delay was about five years. Yes. And the friend of my family, I think it took her about three years for a diagnosis.
Yeah. So as you’re talking, it’s reminding me of some of the things, you know, Patients with POTS don’t necessarily look visibly sick. They might be told it’s all in their head, they might be told it’s anxiety. They might be misdiagnosed with an eating disorder or you’re gonna talk more about that eating disorder sort of connection. Either misdiagnosing or, you know, when you have GI disturbances and things going on there, those types of things can lead to anxiety and eating disorders or disordered eating and just, depression and all kinds of mental health issues.
[00:18:48] Cheryl: I’m so glad that we’re talking about this because there’s two parts and it’s chicken and the egg, and one is, I’m a really, really, really big advocate for therapy and mental health.
Because anytime someone has a chronic condition, it’s extremely stressful. It’s stressful for their person, It’s stressful for either their partner or their family. It’s a heavy load, and this is even prior to COVID and all the things that have come along with that. Having an outlet to talk about it so that someone doesn’t have to burden their family or has a way to process it is really critical.
But for many years, and even still, many people suggested that POTS was quote unquote just all in your head or just about anxiety, and that actually isn’t true and is a stigma that many people are still trying to debunk. And then there is the piece about eating disorders. So it’s very common that you know, 90% of people with POTS do have GI issues.
And part of the issue, as we’ve talked about before, is that POTS is about blood flow and the issue is that there’s often not enough blood flow to your brain, and when you’re eating, blood flow goes to your intestines. And so it’s not uncommon that when people with POTS eat, they feel worse because blood flow is literally going from their brain to their intestines. And so oftentimes what happens is people say, I know I’m supposed to be eating, but every time I eat, I feel bad. And so I’ll hear from people I know I’m supposed to eat, but I’m starting to, feel like I just shouldn’t be eating because either my stomach hurts or I’m feeling badly, or I’m having cramps, or just name your GI symptom.
and people will say, I just don’t know what to eat. Just tell me what to eat. And if I know what to eat and what won’t hurt, I’ll eat. Otherwise I feel like I’m afraid to eat. And the idea is that’s not an eating disorder. That’s someone who needs the guidance of a dietitian.
And so the idea is that’s where we can be so, Helpful in coming up with something, you know, a way of helping people eat to help them manage their symptoms, whether it’s the smaller, more frequent meals so there won’t be the blood sugar fluctuations or so that there won’t be as much of blood flow issues.
When people have larger meals, there’ll be a bigger change in blood flow and more blood flow will go to the gut. And so that’s one thing. We have also seen in recent studies, there was a study that came out, I believe it was in April, showing that higher glycemic meals caused a more rapid response in change in blood flow and caused an exacerbation of symptoms in people with POTS.
So these are all things that people can work on. The other thing that is important to keep on people’s radar is there is an increased incidence of eating disorders in people with POTS. So if you’ve got someone who does have an eating disorder, it’s also important to know that there are people who really shouldn’t be making shifts in what they’re eating and maybe would do better with GI hypnosis or GI C B T or other types of techniques where it isn’t about necessarily changing their food. And it’s more about other, looking at salt or looking at fluid. And so it’s really important to tailor what we’re doing to what the person needs and making it individualized.
[00:22:23] Melissa: Right. And in your paper, which by the way, I didn’t say earlier, but this is published in the Journal of the Academy of Nutrition and Dietetics. September, 2022. In your paper, you say an eating disorder specialist can help determine whether a patient is avoiding a food due to POTS symptoms or an eating disorder.
Knowing that the two can go hand in hand, or like you said, chicken or an egg. And to your point also in the paper, you say patients with a new diagnosis of POTS or patients with an existing diagnosis, particularly those with other comorbidities and disabilities, may experience a magnified sense of stress loss or trauma due to difficulty accessing needed care, or fears for their safety and current or future wellbeing. Patients need a compassionate provider to empathize with the difficulty navigating a complex diagnosis in the middle of a pandemic without the usual forms of social support and in a referral to a therapist may also be warranted.
So I wanted to share that to tag onto what you were just saying. And like I said, we are gonna walk through the specific dietary related management tips and the reasons for those. And, we’ve touched a little bit on those, but we are gonna, map that out, as clearly as we can for the audience.
Was there anything else about your story that you wanted to share before I share my family friend’s story?
[00:23:51] Cheryl: No, no, please do.
[00:23:53] Melissa: Okay. Well, I don’t normally do this, but like I said, I was so touched by what this family friend, and I will referred to her as Miss E. And like I said, this might be a little bit of a case study, but also kind of compare and contrast to your story.
I just asked her some things like, what were your symptoms? When did you know something was wrong? How long did it take you to get a diagnosis? How did that make you feel? Things like that. All the questions I probably could have asked her before. But I didn’t wanna pry.
But these are things that really do need to be talked about. And she said that she was so glad that I asked her because she’s very open about it and she wants more people to be aware of it. So I got her permission to share her story. I won’t share all the details, but I did pull out quite a few things that I wanted to share.
She said her first symptoms were fainting, and nausea, vomiting, extreme fatigue even after sleeping all day. And, said that this is something that a lot of people with POTS have the same story. Like you, prior to this happening to her, she was extremely active and healthy until one day she wasn’t.
And she had been sick with a viral infection prior to that. And, it wasn’t until she woke up after fainting at the beach and she was greeted by the EMS team, she knew something was seriously wrong. She had been a travel soccer player, played first chair in orchestra, straight A’s, and then all of a sudden she was bedridden for an entire summer, unable to keep any food down or walk up the stairs.
Like I said, it took her about three years to get a proper diagnosis, but she really makes the point that she feels fortunate that she had the access to care and the insurance and the family support. I mentioned she’s a friend of the family, so my niece is a really good friend of hers. You know, there were times when my niece would help her walk out of the school when she was trying to faint again, and that just, you know, that pulls up my heartstrings. But she really says people who don’t have access or can’t afford specialists go much longer without a diagnosis if they ever get one. Much less the treatment. I thought this was really compelling, she said that, she went to all these specialists she had all this access to treatment, and started looking at treating the symptoms until a lot of trial and error. And she ended up going to a pulmonologist and when he told her that she did not have a tumor in her lungs, he looked at her and said, You seem displeased about this. . . And she explained to him that she was so grateful that she didn’t have a tumor, but she was still desperate for a diagnosis.
[00:26:46] Cheryl: Yeah. And that really resonated with me because when people know there’s something wrong and their tests show that everything is good, that’s not good news. You know, when you know there’s something wrong because you feel really bad, having a result showing there’s something you can do is empowering.
[00:27:05] Melissa: Absolutely. And then she was so overjoyed, when she was finally diagnosed, but that was very short lived because that’s when she realized it didn’t necessarily mean there was a treatment or there was a lot of trial and error.
And so she had held onto this expectation for so long and now she felt more scared, and worried if she would ever be healthy again. And she made a lot of changes. She was really struggling to find foods that didn’t make her sick, she changed her sleep schedule, medications, the food she ate, she wore compression socks to help with her blood pressure and increased her fluids.
And some of these things worked better than others. But this is the last thing that, that I’ll share because it really spoke to me. She says, To be quite honest, each time I reflect on this time in my life, I try to make it sound positive, but the majority of the time following her diagnosis, she was even sicker because she was really sensitive to some of the medications.
And one of the medications even caused her to become suicidal. And she felt much better when she went off of that. But again, a lot of trial and a lot of error involved in that. And her symptoms did almost fully resolve around the age of 19 or 20. which she feels so grateful for.
So I don’t know if you could speak to that as well as far as like what the chances are for this to resolve. And a lot of that might be prognosis.
[00:28:34] Cheryl: In terms of prognosis. There are some people, especially when they develop POTS around menarche because it is typically women and often involved around hormones.
And often when people go through their period and shifts and fluctuations and hormones, and sometimes when they go through that period of time where there’s a shift in hormones and go through that sort of intensity. And sometimes they come through it and shift in hormones or whatever else, and they get better.
And I haven’t seen great numbers. And some of that is just because POTS has only been studied for 20 years. But there is a percentage of people who get better. There is also a percentage of people who resolve through a shift in physical activity. Again, there isn’t great data on what number. Often it’s more of people improve and there are also a percentage of people where they get better and their symptoms may come back when there’s a stressor of some kind at some later point in their life. When you have a disease where they’ve only been studying it for 10, 20 years, having a sense of. Okay, this is the prognosis. When people hopefully live much longer than 10, 20 years, it’s awfully hard to study the life course of a disease. For people, it’s learning how to manage it better versus quote unquote curing it. most
That is for most people what they’re after being able to manage POTS and being able to go back to work and play and having a good quality of life versus the idea of, Hey, I’m cured.
Yeah. Quality of life. Yes. Having better and improved quality of life is usually where it’s at. You know, being able to get back to the things people love. And enjoy.
[00:30:26] Melissa: Absolutely. Before we dive into the specific dietary lifestyle management recommendations, I wanted to share one more thing from my friend, Miss E. She has this analogy and I think as we’re talking about this syndrome and all of these symptoms, she says, This is the analogy that I use, comparing a patient to a car and I love car analogies.
I use that with diabetes a lot. So it’s difficult to manage POTS if you look at the symptoms individually, let’s say the GI symptoms are a flat tire and the fainting is the oil being low. Sure you could patch the tire, but if you don’t have any oil, the car still isn’t going to run.
You have to look at all the symptoms together to understand how each interacts with each other. And again, that speaks to the difficulty diagnosing and treating it. I don’t know if you had any similar or thoughts based on that analogy.
[00:31:20] Cheryl: Yeah. I really like that analogy because certainly when I first got sick, everything was wrong.
You know, just if it was the car panel and the engine light, like every single light would’ve been flashing and I think that was why it took so many years to get me back to a functional kind of state because there was some so much going on and it was all being treated. You know, a little bit here, a little bit there, and it took a long time to get things back to a more functional state.
But she’s absolutely right that most doctors treat it as like, Okay, we’ll work on this, so we’ll work on that, versus understanding how POTS is. For me, POTS was related to ehlers-danlos, which was related to digestive disorders, which was related to what’s known as myalgic encephalitis and chronic fatigue, and how those different things all interconnect.
And in the paper there’s that diagram and like I had almost all the things in the diagram. And rather than treating them as, Oh, this is a syndrome where people have all these things and let’s look at them all together. At that point in time when I was experiencing this, this wasn’t even established in the literature.
And so it, I don’t even fault my doctors because they would’ve had to be kind of before their time to understand how the things were interconnected. It’s difficult when you’re sort of before the research and sometimes that’s just how it goes.
[00:32:49] Melissa: Right, Absolutely. And do you feel like you are in a place where things are managed fairly well and you have the quality of life that you are wanting?
[00:32:59] Cheryl: You know, in terms of my POTS issues, my POTS issues are generally pretty well, fairly managed, and that’s something I’m incredibly grateful for. The main thing that inspired me to write the paper was seeing the rates of POTS go up as the rates of COVID have gone up and really understanding that I didn’t wanna see anyone have to go through what I went through and that your friend went through and wanting people to have an easier time than I did in understanding that I don’t think the system is that much better than it was 20 something years ago.
[00:33:39] Melissa: Right. Definitely appreciate the work that you do and raising awareness on this and getting the word out.
So let’s walk through the nutrition and lifestyle recommendations, what the recommendations are and why we’re making those.
[00:33:54] Cheryl: Absolutely. So I’m gonna start with fluid because that’s the one that’s most concrete. So the fluid, the beginning is just two to three liters of fluid, and that’s pretty easy.
That translates to eight and a half to, I believe it’s 12.7 cups of fluid. Usually I recommend people start drinking fluid even before they get out of bed, simply because that’s a lot of fluid to drink across the day. But it does really help because it increases the volume of the blood, which means there’s more blood that goes to your head, which is really key in terms of helping with the lightheadedness.
The second guideline tends to be a little bit trickier. This one is written as 10 to 12 grams of salt. And this one for many people is very tricky because as dietitians, often what’s drilled is low salt diets. And the idea is people with POTS actually need the salt. The other piece, and hopefully it’s okay if I explain and unpack this a little bit.
We’re used to talking in terms of sodium. The dietary guidelines are written in terms of sodium, 2300 milligrams of sodium. But the POTS guidelines are written in terms of salt. 10 to 12 grams of salt. And salt and sodium are not the same thing. Sodium is just pure Na. Whereas salt is NaCl, so they have different molecular weights, so they don’t actually convert into each other.
Even though they sound like the same thing, and I can actually give you a link to a converter so you can put that in the show notes. Okay. Because it’s knowing it’s easy to get confused, and there are times where I get turned around, but you actually have to convert one to another. So 10 to 12 grams of salt is four to 4.8 grams of sodium.
But the take home, is it’s adding one to two tablespoons of salt, and that’s on top of a typical daily intake. So you know, you have someone’s normal intake, and then on top of it you’re adding one to two teaspoons of salt in addition to someone’s typical intake. So you’ve got someone’s normal daily intake, and then you would ask the doctor for a sodium or salt goal because sometimes people need to have a particular amount of salt simply because of other conditions. So I always do try to check in with the doctor because I have one client where she only has one kidney. I have another client who needs to be on a different prescription simply because of other medications.
So I don’t always do the 10 to 12 grams. Sometimes it has to differ. Okay. But if I don’t get something from the doctor, then I usually start with one teaspoon of salt and gradually work my way up to two teaspoons. In terms of other dietary guidelines we talked about before, the smaller meals. Smaller meals can be helpful because then there’s less of, fluctuation in terms of blood volume because whenever you are eating some of the blood volume goes to the stomach versus going up to the head. So smaller meals can be really beneficial. And there has also been a study showing lower glycemic meals can be helpful.
[00:37:22] Melissa: Yeah, I was gonna ask you about that, and I think you mentioned this earlier. That’s more about the blood volume than the blood sugar or can you say more about that?
[00:37:33] Cheryl: Yeah, so for a long time, this was just observation that people seem to do better on lower glycemic meals, but there’s actually been one study and I can send you the link so that you can put it in the show notes where they compared people without POTS to people with POTS, and what they found is that people with POTS seem to have more adverse symptoms when they ate higher glycemic meals than people without.
So again, only one small study, but it backed up what people were observing for a long period of time.
[00:38:07] Melissa: So it sounds like maybe the mechanism or what exactly is happening there isn’t clear yet, but.
[00:38:13] Cheryl: Isn’t totally clear yet. But it’s something.
[00:38:15] Melissa: But there’s that association.
[00:38:16] Cheryl: Yep. That association. The other things, generally avoiding things like caffeine, avoiding things like alcohol that tend to be dehydrating. Simply because we’re trying to hydrate people really well. Got it. So those are things in terms of diet. Now switching gears to lifestyle, one of the things that can be really helpful is compression garments.
I know this was something that your friend Miss E mentioned can be really helpful. Part of it is because people with POTS tend to have fluid that pools in their legs and in their abdomen. So now if you’re wearing compression garments, it’s harder for things to pool. So in theory, best case scenario is you’re able to wear compression garments all over your legs and all the way up to your abdomen.
Some people don’t tolerate that. Sometimes people just can only tolerate compression garments on their lower legs or on their abdomen. Whatever people can tolerate tends to be helpful because it keeps fluid and blood from pooling where it’s not supposed to be pooling. Because the idea is whatever can keep the blood volume back up where it belongs, meaning at the heart or at the head, will tend to make POTS symptoms better.
Gotcha.
Oh, another big one is around physical activity. And this is one where we try to separate old school POTS, meaning POTS before COVID and POTS after. Generally for people who have POTS, physical activity can be helpful. And so I try to give a couple of caveats. So generally having people do recumbent exercise, meaning lying down exercise. This may be things like a recumbent bike or exercise in the pool or using a rowing machine. And generally this is starting off really slowly, so this may be doing a minute of exercise a day or two minutes, and so building up really slowly with an eventual target of 30 minutes a day.
Uh, the caveats that if you’ve got someone who’s hyper mobile and is dislocating everything, you want them working with a physical therapist. And if you’ve got someone with a condition called myalgic encephalitis, which is also known as chronic fatigue, who’s exercise intolerant, you want them working with a physical therapist because doing too much exercise can make you worse.
[00:40:42] Melissa: Right. And likewise, I can imagine if you’re not feeling well you’re not feeling up to exercising and then that could probably exacerbate some things as well.
[00:40:52] Cheryl: Absolutely. And it’s actually the same thing with long COVID. It’s very similar to myalgic encephalitis and that’s often used as analogy.
Often people have the perspective of no pain, no gain, and the more you do, the better you are, except that’s absolutely not the case. And so there’s a technique called pacing, and it’s often known as stop, rest and pace for people with long COVID and for people with ME working with someone who is experienced with pacing so that they’re absolutely working within what’s known as your envelope so that they don’t have you overdue can be really helpful. There’s, I’m gonna say more that we don’t know about long COVID than what we do. But the key around exercise and long COVID is making sure that someone doesn’t have you overdo and is having you work within your window of tolerance. But for most people around movement, less is more.
[00:41:57] Melissa: Yeah. And there’s certain, maybe you said this because I always try to listen and process at the same time, but there’s, like recumbent biking, swimming, rowing types of exercises that might be better tolerated.
[00:42:12] Cheryl: Yes. So for both regular POTS and long COVID POTS, recumbent meaning lying down exercise is better than upright exercise because when you’re lying down, you’re not fighting gravity with that blood volume.
And when people are stronger, then they can quote unquote, graduate to standing exercises and other things, but certainly as tolerated.
But certainly initially people tend to do better with recumbent exercise.
[00:42:42] Melissa: So there’s the diet recommendations. Of course, these are just things that would be suggested, but every individual has to be tailored to their specific symptoms and situation. We touched on this before, but also managing those digestive issues and screening for eating disorders.
[00:43:00] Cheryl: Yeah, I know I didn’t say very much about digestive issues because it’s absolutely going to be different based on different people. Some people have IBS, some people have gastroparesis, some people have reflux, some people have Celiac. So everyone is going to need what’s known as medical nutrition therapy that’s absolutely tailored to their own needs.
And there are some people who don’t have digestive disorders and more power to them. Lucky, right? So that’s gonna need to be very individualized.
[00:43:29] Melissa: We talked about the sort of correlation between. POTS and eating disorders. But I also read in your paper some interesting information about celiac.
So do you wanna share that?
[00:43:40] Cheryl: Yeah. Thank you for asking. So in the general population, 1% of people have celiac disease, but actually among people with POTS, it’s 4%. And this is an interesting statistic. Certainly that’s much higher than we would expect. We don’t really know why. Some of it may be that overall, there’s a higher rate of autoimmune disorders among people with POTS and some of it falls in the category of there are so many things we don’t know about POTS and there’s so much more research that needs to be done.
It may have to do with joint hyper mobility, and ehlers-danlos also has a link with POTS and a higher prevalence with celiac, so that may be part of what’s going on, but there’s more that we don’t know than what we do.
[00:44:26] Melissa: Yeah, that’s really interesting because like I know with type one diabetes, being an autoimmune disorder, we see an increased incidence of celiac.
And if somebody has celiac disease, we’re looking, Oh, is there any diabetes in your family? And vice versa.
[00:44:42] Cheryl: Yeah, so the take home is, you know, as a dietitian, sometimes when you have someone with IBS, you’d wanna try sometimes do something like a low FODMAP diet, or there are times where someone wants to try gluten-free diet.
But absolutely, when you have someone with POTS, you’d always wanna make sure someone was tested for celiac disease before ever taking gluten out of someone’s diet simply because the rate of celiac disease is much higher than it would be in the general population.
[00:45:08] Melissa: Right. I mean, we’ve been talking about how, uh, this seems simple, but it’s actually quite complicated.
You know, I have a ton of great resources, including your paper. Miss E gave me this YouTube video that has a really good explanation about POTS and, we’ve got the Dysautonomia International website that I’ll share as well. And Miss E shared that crowdsourcing with POTS can be depressing and inaccurate.
But understandably, a lot of people feel that it’s the only way to get some answers or validation or some sort of needle in the haystack that they’re looking for. So I’ve got some great resources to share and you’ve already mentioned some things that you’re gonna gimme links to as well.
But what else would you like us to know about POTS that you know, we can help raise awareness and if clinicians are listening, that they can be more able to maybe connect some of those dots and help patients seek proper diagnosis.
[00:46:09] Cheryl: Well, to your friend’s, point about there being so much crowdsourcing.
I think that’s because there’s been such a void around clinicians knowing enough. My hope is that clinicians step up and are more knowledgeable and there are more clinicians that are knowledgeable. They’ll be filling that space and that patients will have a place to go and get knowledgeable answers.
That’s certainly my hope of what will happen so that patients will feel empowered to go to someone to ask their questions. I’m hoping that this podcast will be a part of that.
I hope so too.
And that will ripple out. That, you know, a silver lining of the rate of POTS going up is that there’ll be more information out there.
[00:46:57] Melissa: I was thinking that earlier, and I didn’t know if I should say that, but it is true. It certainly is gonna help raise awareness.
[00:47:04] Cheryl: Yeah, it’s knowing that POTS has been, there are many conditions that have been overlooked and neglected for entirely too long and that there’s been at least an increase in funding and awareness, and they should have been funded beforehand, and my hope is at least now they’ll be better funded and hopefully there’ll be more movement toward better medication, better treatment. It’s knowing that people have been suffering for an awfully long time, and there have been many researchers who have been in this game for decades and have been working extremely hard for a long time.
[00:47:41] Melissa: And even I have a family member who ended up being diagnosed with severe anemia, but for months prior to that was told that she just had anxiety.
It’s such a shame.
Was sent to a therapist, which I mean, therapy’s good, but it’s not gonna cure iron deficiency anemia!
[00:47:58] Cheryl: No. And I’m gonna wager a guess that this is a female family member.
Yep.
Part of my frustration is more often than not, and my understanding of this is that it’s in the literature that diseases that are predominantly female, and again, this is from studies that I, that can put in the show notes too.
The diseases that are predominantly female are less funded, and it shouldn’t be this way. It’s so hard and that it’s important that there is at least equal funding and that there’s the funding that is needed for people to have adequate quality of life because POTS does have such an effect on quality of life for people.
And part of what’s so hard is that POTS affects people in their teens, in their twenties when people should be out, partying out, dancing out, having fun, out, going to school, living their life.
[00:48:48] Melissa: Or at least going to school. Right?
[00:48:49] Cheryl: There you go. But out living their life, not thinking about things not in bed and miserable.
And it can really have such a devastating effect on people.
[00:49:01] Melissa: Absolutely. One of the other resources is of course, your website, harriswholehealth.com, and people can follow you on Twitter at Cheryl Harris RD. You’re on Facebook. And like I said, I’ve got a lot of really great resources so people can go to the show notes at soundbitesrd.com for all of that.
And is there anything else that you wanted to share as far as like parting words of wisdom for us?
[00:49:25] Cheryl: Oh, I just wanted to thank you so much for highlighting such an important topic.
[00:49:30] Melissa: My pleasure. I’m so grateful that I stumbled upon your tweet. And by the way, people can go to your Twitter page, it’s your pinned tweet that talks about your paper, but I’ll have a link to it as well so people can read all about that and follow you on Twitter and stay tuned for any updates and hopefully we’ll see you doing some webinars and presentations on this within the dietetics community.
[00:49:53] Cheryl: Absolutely. Yeah. I’m certainly very excited to get more information about POTS specifically and dysautonomia out there because there really just isn’t enough information about it, and it’s really something that dietitians should at least have a working knowledge about.
[00:50:10] Melissa: Absolutely. In your paper, you say it is critical that registered dietitian nutritionists have the expertise to provide dietary and lifestyle advice for proper management of POTS and to coordinate with the rest of the healthcare team. So amen to that. Cheryl, thank you so much for coming on the show and sharing this important information. I wish you the best.
[00:50:32] Cheryl: Aw, thank you so very much. Thank you so much for inviting me.
[00:50:35] Melissa: Absolutely. And for everybody listening, as always, enjoy your food with health in mind. Till next time.
For more information visit soundbitesrd.com. Music by Dave Birk. Produced by JAG in Detroit Podcasts.
LISTEN, LEARN AND EARN
Listen to select Sound Bites Podcasts and earn free CEU credits approved by the Commission on Dietetic Registration (CDR) for registered dietitian nutritionists and dietetic technicians, registered. Get started!
Get Melissa’s Sound Science Toolkit here!
Partnerships:
Sound Bites is partnering with the Association of Diabetes Care and Education Specialists (formerly the American Association of Diabetes Educators)! Stay tuned for updates on the podcast, blog and newsletter!
Sound Bites is partnering with the International Food Information Council! Stay tuned for updates on the podcast, blog and newsletter!
I don’t know how to thank you enough for the podcast on pots. My daughter was diagnosed with pots a year ago and is improving in health. Hearing your message made me feel hopeful that the word is getting out in the medical community about this little known condition. What an absolutely beautifully done recording! Thank you thank you thank you!!
Victoria,
Thank you for listening to the episode and taking the time to comment. I’m so glad you are feeling hopeful! I, too, hope this helps get the message out to more healthcare professionals. I’m glad to hear your daughter is improving!
Melissa
All I have to say is this is the FIRST TIME IN MY LIFE that I ever heard the words “this was me” come out of my mouth! My experience was almost the same as yours because I was bit by a tick and once the Lymes symptoms started they last for years and I couldn’t even put my hair up or drive down the street without falling asleep.
I am speechless right now that this is a real story because I was in the same situation not too long ago before I realized it was up to me to figure out how to manage my symptoms
Sign up for my monthly newsletter and episode eblasts so you never miss an update!
Listen on Stitcher (Android)
Install the Stitcher App
1. Search for “sound bites with melissa joy dobbins” 2. Choose Play Current Episode or Add to Playlist
Choose “Play Episode”
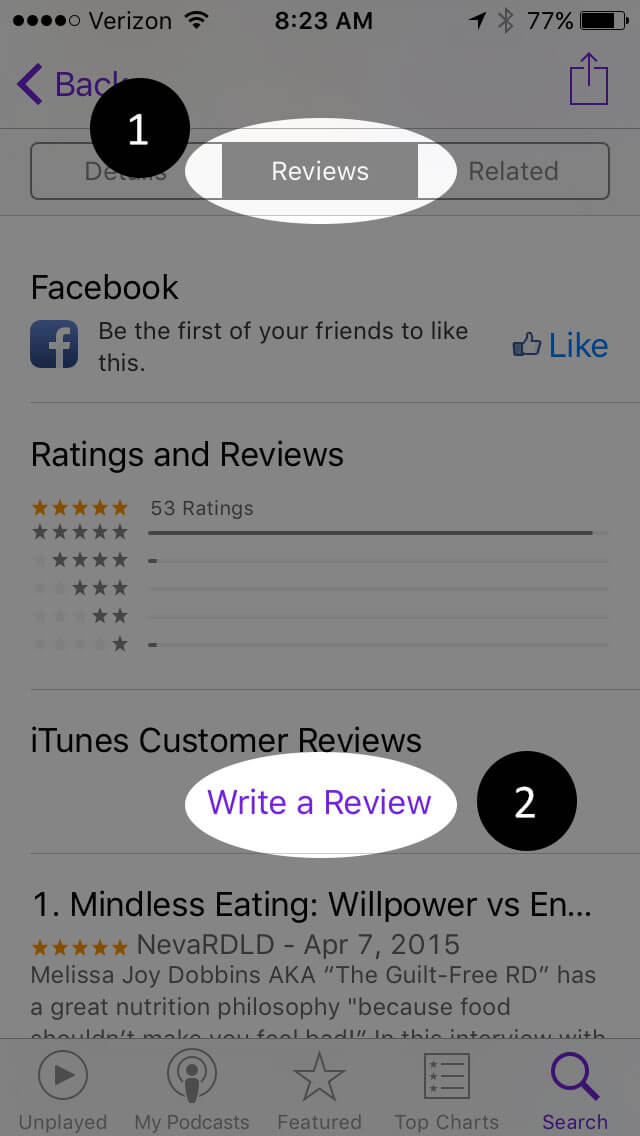
Subscribe & Review on iPhone
Open the “Podcast” app on your iPhone
Search for “Sound bites with melissa joy dobbins”
Open the podcast and click “Subscribe” and your done!
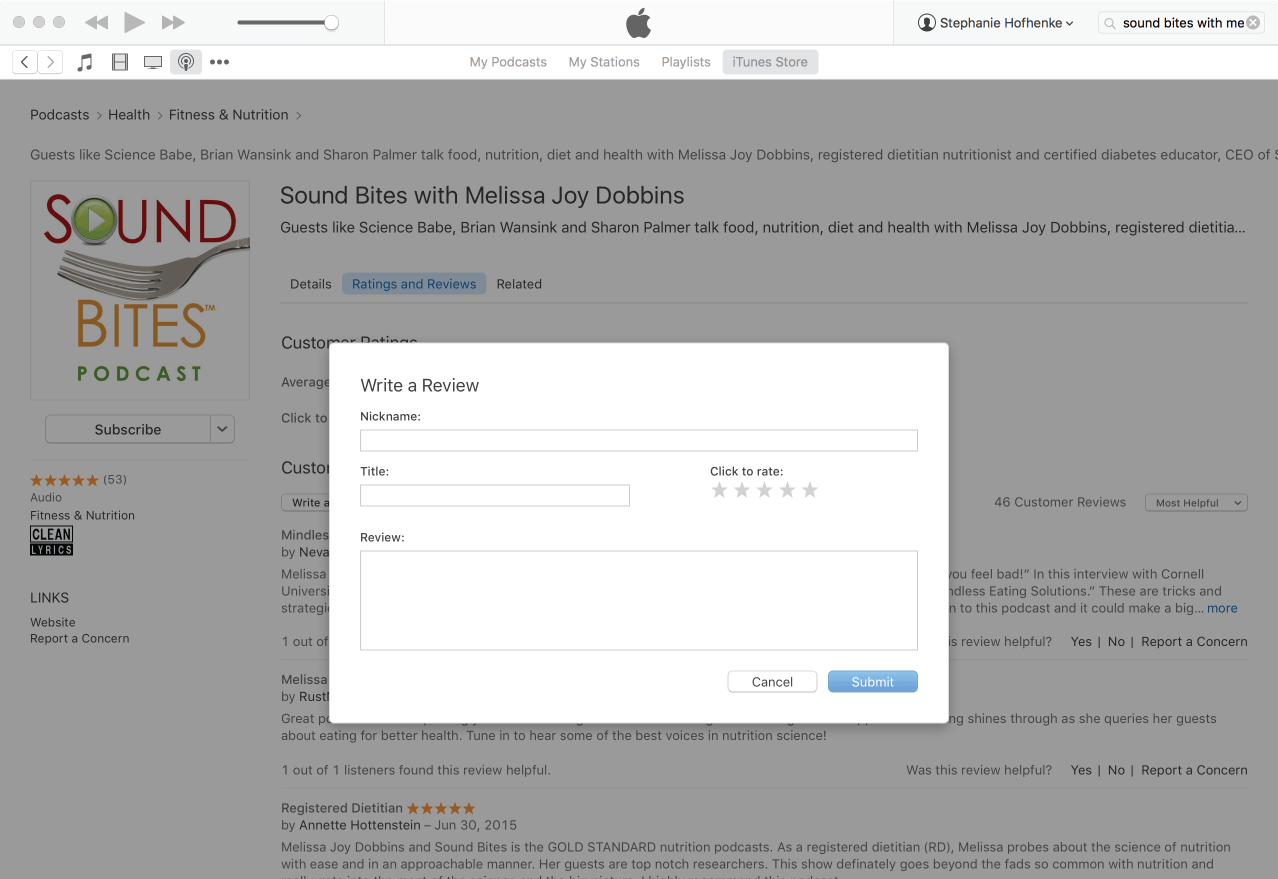
Write a Review
Click “Reviews”, then “Write a Review”.
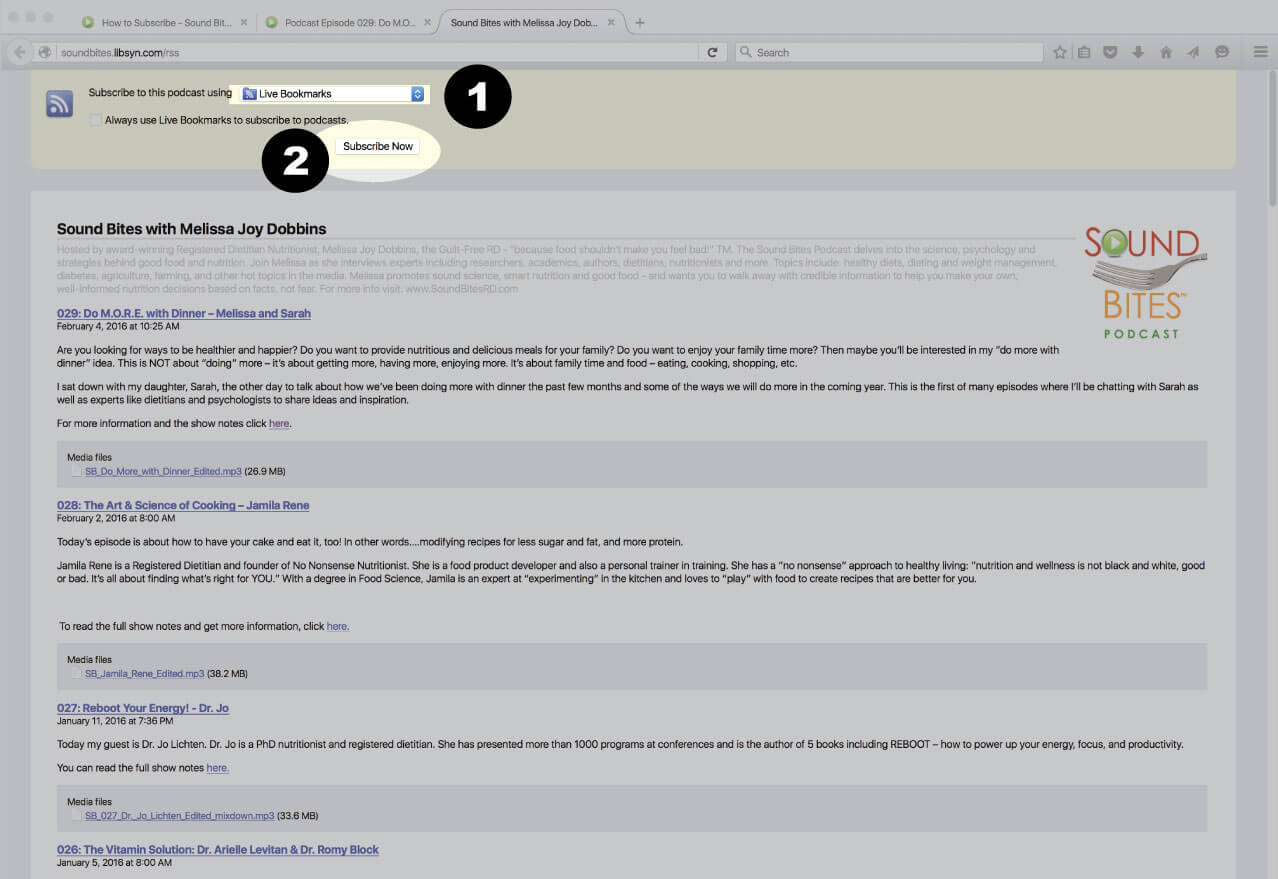
Subscribe via RSS Feed
Navigate to any podcast player . Click on the RSS feed icon.
Click on the RSS feed icon.
Click on RSS Feed
Choose which application you would like to use to receive the RSS feed
Click “Subscribe Now”
Confirm settings and subscribe.
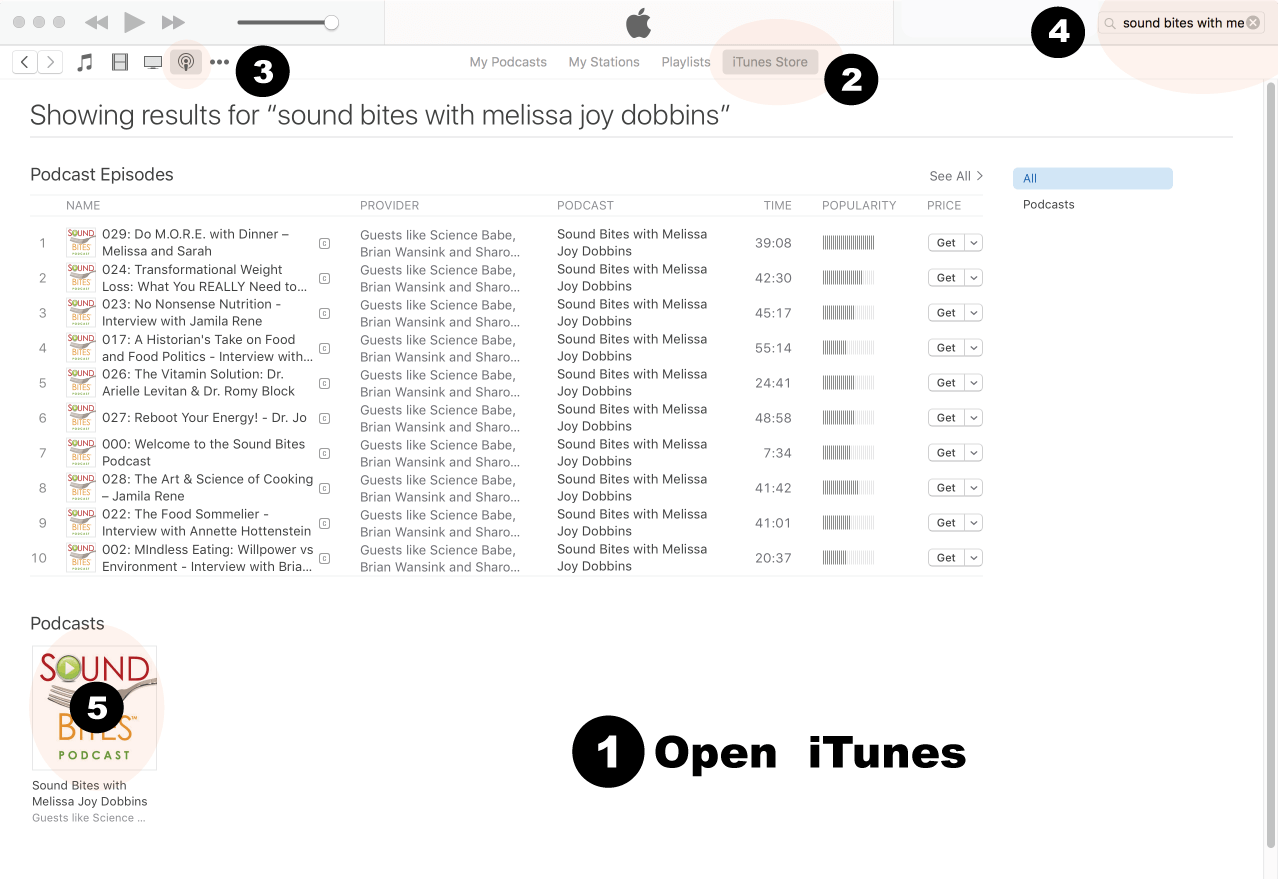
How to Review in iTunes
Open iTunes desktop application
Click iTunes Store
Click on Podcasts
Search for “Sound bites with Melissa Joy Dobbins”
Click on podcast image
Search for Sound Bites podcast in iTunes
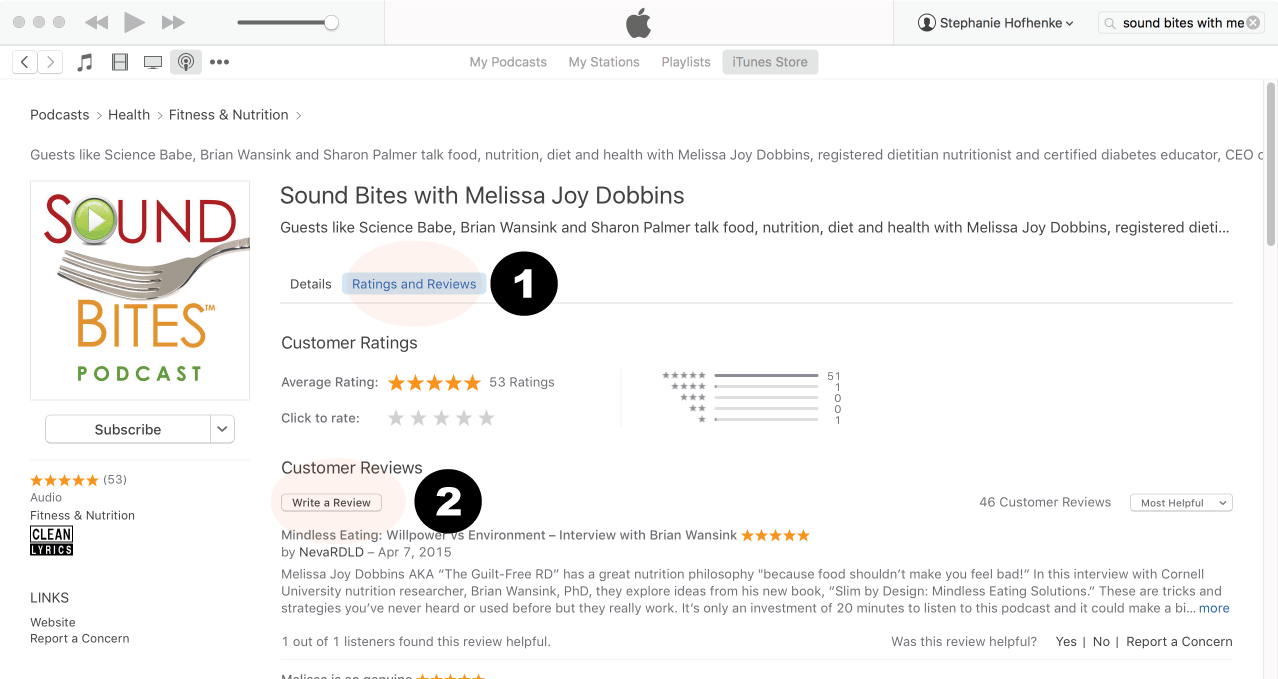
Click Ratings & Reivews
Click Write a Review
View reviews and write your own review.
Write your review…. Thank you!
Write your review!
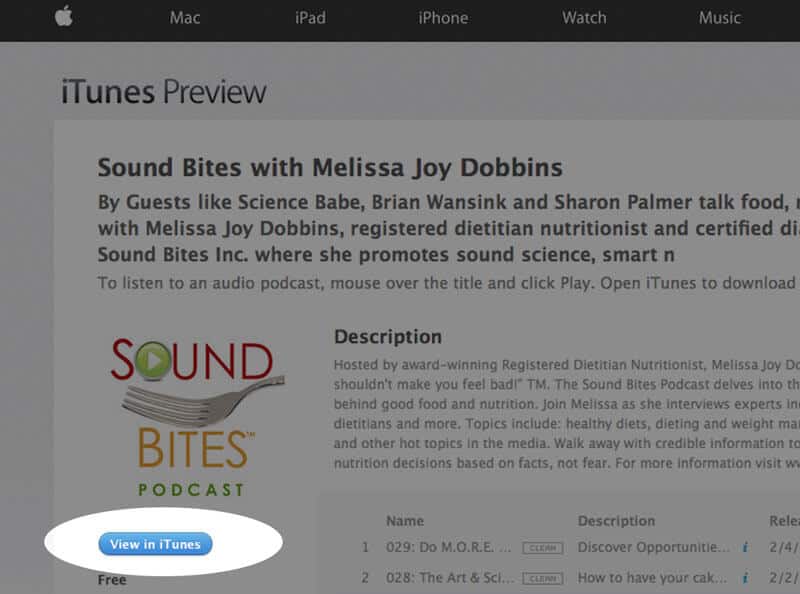
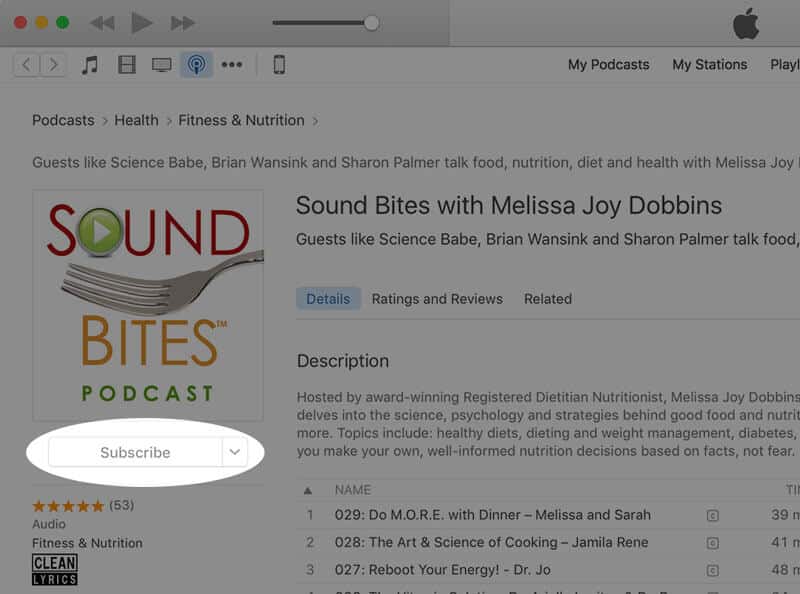
How to subscribe via iTunes
Click here to view the Sound Bites Podcastin iTunes, then click the blue “View in iTunes” button. This will open your iTunes application directly to Sound Bites Podcast. Click the “Subscribe” button, and your done!













I don’t know how to thank you enough for the podcast on pots. My daughter was diagnosed with pots a year ago and is improving in health. Hearing your message made me feel hopeful that the word is getting out in the medical community about this little known condition. What an absolutely beautifully done recording! Thank you thank you thank you!!
Victoria,
Thank you for listening to the episode and taking the time to comment. I’m so glad you are feeling hopeful! I, too, hope this helps get the message out to more healthcare professionals. I’m glad to hear your daughter is improving!
Melissa
Thank you for this podcast ! My daughter was diagnosed 3 weeks ago & I’m trying to learn all I can to help her get her life back . 🙏🏻
Christine,
I am so glad you found this helpful and I wish the best for you and your daughter!
Melissa
All I have to say is this is the FIRST TIME IN MY LIFE that I ever heard the words “this was me” come out of my mouth! My experience was almost the same as yours because I was bit by a tick and once the Lymes symptoms started they last for years and I couldn’t even put my hair up or drive down the street without falling asleep.
I am speechless right now that this is a real story because I was in the same situation not too long ago before I realized it was up to me to figure out how to manage my symptoms