Celebrating over 1 Million Downloads and 50,000 Free CEUs on the Sound Bites® Podcast | NEW: Get 1 years’ worth of CEUs with the new 15-CEU Podcast Course
While there are many factors that affect fertility, diet is one of the few things that we can modify. Various nutritious dietary patterns have been linked to improved natural conception and fertility treatment outcomes, and none of those diets restricts gluten, soy, dairy, or specific food groups. For those who are trying to conceive, or who are pregnant, postpartum, breastfeeding or managing conditions such as PCOS and endometriosis, dietary and lifestyle changes may help support healthy outcomes. But what does the research show about weight and fertility outcomes?
Tune into this episode to learn about:
Why nutrition for fertility matters
Research on weight and fertility outcomes
BMI cutoffs for egg retrieval procedures requiring anesthesia
Research on dietary patterns and fertility outcomes
Fertility and disordered eating
Benefits of a weight-inclusive approach
Why working with a dietitian with experience in fertility is important
Rachelle’s 1:1 services and online course
Think of nutrition as a support tool to improve your chances of conceiving and having a healthy pregnancy, rather than stressing about everything you eat when trying to conceive.” – Rachelle Mallik
Rachelle Mallik, MA, RD, LDN
Rachelle Mallik is a dietitian and owner of The Food Therapist, a virtual private practice specializing in nutrition counseling and education for reproductive health. Rachelle supports clients who are trying to conceive, pregnant, postpartum, breastfeeding or managing conditions like PCOS and endometriosis with a weight-inclusive approach that focuses on nourishment rather than restriction. Rachelle is a member of the Academy of Nutrition and Dietetics, including the Women’s Health Dietetic Practice Groups. She is also an active member of the Nutrition Special Interest Group of the American Society for Reproductive Medicine (ASRM). Rachelle serves as the reproductive nutrition content expert for the Nutrition Care Manual. She has presented for the Chicago Academy of Nutrition and Dietetics and at the ASRM Scientific Congress, and advocates for the role of nutrition and dietitians in multidisciplinary reproductive healthcare.
[00:00:00] Announcer: Welcome to Sound Bites hosted by registered dietitian nutritionist Melissa Joy Dobbins. Let’s delve into the science, the psychology, and the strategies behind good food and nutrition.
[00:00:22] Melissa Joy Dobbins: Hello and welcome to the Sound Bites podcast. Today’s episode is about the relationship between body weight, diet quality, and fertility. What does the research show? My guest today is Rachelle Mallik. She’s a dietitian and founder of the Food Therapist, a virtual private practice specializing in nutrition counseling and education for reproductive health. Rachelle supports clients who are trying to conceive, who are pregnant, postpartum, breastfeeding, or managing conditions like PCOS and endometriosis with a weight-inclusive approach that focuses on nourishment rather than restriction. Welcome to the show, Rachelle.
[00:01:04] Rachelle Mallik: Thanks so much for having me.
[00:01:06] Melissa: So excited to talk with you. This is not an area of expertise of mine. We’ve had several conversations over coffee because we don’t live too far from each other, and I just found the work that you do really interesting. I do want our listeners to know that this episode is not sponsored, and we may be submitting it to CDR for continuing education credits for dietitians, diet techs, and certified diabetes educators. If that is of interest to you, stay tuned for that. You can always check my free CEU page at soundbitesrd.com to see what CEUs are available.
There are some ethics CEUs as well. There’s usually about 40 or 50 on any given time that you can access. Rachelle, I would love for you to share with our listeners more about your background education and the work you do. Maybe why and how you got interested in this topic. I know it was pretty early on in your career that you really started focusing in this area.
[00:02:05] Rachelle: That’s right.
[00:02:06] Melissa: Also, if there’s any disclosures to note, please do that as well.
[00:02:09] Rachelle: Thank you for this opportunity to speak about my work. Yes, I started working in the fertility field in 2006, so I’m it’ll be 18 years this year, which is hard to believe. I actually started as a pre-med undergrad with a degree in nutrition, and I was just trying to figure out the career path. I needed to get some more experience in the medical world, and so I got a job. I grew up in New York. I’d gone to school undergrad at Arizona State and then I came back to live in New York City. I got a job at the Cornell Center for Reproductive Medicine and Infertility.
My job there was an IVF patient coordinator, so I worked with 100s if not 1000s of patients over my years there. I worked there for almost five years, walking people through all the aspects of going through fertility treatments. The testing, all the procedures that they might need, looking at a calendar when their period was and when they expect to start their stimulation. I’ll get into some details about IVF in a little bit, but it was through that experience that I actually decided to continue my training to become a dietitian.
I stayed working there and then I went back to school for my master’s degree because I really wanted to focus on how nutrition can support people in preventing and managing diseases, and in this case specifically looking at infertility. That’s how this seed got planted if you will. I was only 23 years old at the time, so fertility was not something on top of mind for me. Then, let’s see, after I got my degree and became a dietitian, soon after I was in private practice with another dietitian in New York for some time, ended up moving to Australia for about two years with my husband. I don’t know if you and I have talked about that.
[00:03:52] Melissa: No, interesting.
[00:03:53] Rachelle: That’s a bit tangential to this, so I’ll keep moving forward but if you ever want to talk about Australia or Australian coffee in Melbourne, I’m happy to do so.
[00:04:01] Melissa: Okay.
[00:04:02] Rachelle: I’m now a coffee snob because of my time living in Melbourne. When I came back to the States, I started working in clinical nutrition. I worked in a hospital and then when I got pregnant with my son after he was born, I left that role and decided to start my own private practice. I’d had some experience in private practice from when I was in New York and then Australia, and then now at this stage of my life, I had been through getting pregnant, staying pregnant, and being pregnant, and then being postpartum and breastfeeding.
What I realized through that experience was that there aren’t that many dietitians, especially in 2016, that were specializing in that area. Certainly, not many that I knew that also had my background working in a fertility clinic. When I was pregnant, the nutrition guidance that I received that’s pretty much limited to take a prenatal multivitamin, which isn’t bad advice but it’s also not very comprehensive advice, nor are there any standardization. There’s no standards for what a prenatal vitamin has to provide.
Through all of that, I decided to start my own private practice specifically focusing on reproductive health. I work with folks who are trying to conceive, going through fertility treatments, pregnant postpartum, breastfeeding. Then I also work with folks who are managing reproductive conditions like PCOS and endometriosis. Let’s see, I started the practice in early 2017, so I guess we’re coming up on seven years, and over that time I’ve also shifted to a more weight-inclusive approach, which I know we’ll get into a bit and how that relates to fertility as well.
[00:05:37] Melissa: Absolutely. Did you say it was 2016 when you were pregnant with your son?
[00:05:42] Rachelle: Yes.
[00:05:42] Melissa: I did work at a maternal fetal medicine clinic at NorthShore Evanston, the years 2011 to 2013, and so I counseled pregnant women mostly with a diabetes focus, whether they had gestational diabetes or preexisting diabetes, and some multiples that was aside from the diabetes focus. I was pregnant. My son was born in 2008, so I concur that the nutrition guidance was pretty basic. Should I say lacking? I’m really excited to learn more about your experience and working with real people as well.
Let’s start with the main idea behind this podcast episode is that nutrition and diet matter more than weight when it comes to fertility. We’re going to dig into the specifics and nuances of the research related to this. I know in our previous conversations you would throw out some terms or acronyms and I would say, “Wait. What does that mean? That’s new to me.” Maybe if there’s a few major terms or acronyms that you want to define right now, and then of course, if anything comes up during the conversation, we can specify and define those.
[00:06:57] Rachelle: Sure, yes. There’s so many acronyms, and I think that’s true for a lot of medical fields,-
[00:07:01] Melissa: Oh, yes.
[00:07:01] Rachelle: -but we have very specific acronyms. Actually, just the other day I saw an Instagram, an REI who I follow, explaining what an REI is. She’s like, “It’s not just an outdoor store.” For me, I’d actually I’ve never thought of REI. When I say REI as a fertility doctor, I’ve never thought about the outdoor store. Yes, I guess it’s important to clarify that. REI is one I use a lot. That’s the proper term for a fertility doctor. It stands for reproductive endocrinologist and infertility specialist.
REIs are typically who patients are going to see if they’re having trouble conceiving or if they have a condition like PCOS, that’s someone who they’d see. You might go to an OB-GYN for a preconception visit but after a certain amount of time if you’re having trouble getting pregnant on your own, they’ll usually refer you to an REI. Then a couple of other acronyms that I think would be helpful because they’ll probably come up in our conversation. ART. That stands for assisted reproductive technology. That typically refers to when eggs are handled outside of the body.
Whereas, intrauterine insemination or IUI, it’s happening in the body. The eggs are not being taken out of the ovaries. The semen is getting put into the body. Whereas, with IVF and ICSI the eggs are taken out. IVF stands for in vitro fertilization, and then ICSI, I-C-S-I, stands for intracytoplasmic sperm injection. I don’t know what you think about with IVF, but I think a lot of people envision the sperm being injected to the egg kind of video or image have you ever seen that before?
[00:08:38] Melissa: Yes.
[00:08:38] Rachelle: Whereas, IVF doesn’t always involve the sperm being directly injected into the egg. Sometimes they’re just in a Petri dish meeting just as they would inside the body, but outside the body, hence the in vitro. It’s happening in a dish.
[00:08:51] Melissa: Instead of in vivo, right?
[00:08:53] Rachelle: Exactly.
[00:08:54] Melissa: That I got.
[00:08:55] Rachelle: Yes, good. I’m sure we have a lot of medical professionals, RDs, who listen here so they’re probably familiar with those terms in vitro and in vivo. Does that help generally explain it?
[00:09:04] Melissa: Yes.
[00:09:04] Rachelle: Do you want me to go into IVFA little bit more
[00:09:06] Melissa: Maybe as the conversation develops and it warrants yes.
[00:09:10] Rachelle: Yes.
[00:09:10] Melissa: One of the things that struck me in our previous conversations was how knowledgeable you are about the research. I’m just curious in general, has there been a lot of research in this area, a little bit of research? It sounds like there’s so many different things that could be studied. If you could just give us the general top line on where that is in general.
[00:09:31] Rachelle: Yes. Especially compared to when I started working in fertility in 2006, in the past two decades, there’s been a ton more research. I think it’s a combination of both patients, people dealing with infertility who want to know how nutrition can improve their chances of getting pregnant, and staying pregnant, and having a baby. Also, because of that then researchers are more incentivized to study that because that’s what people want to learn about.
I think doctors and other healthcare providers are interested too because again, nutrition is one of the few modifiable factors, right? There’s a lot of things that we can’t control and nutrition may be one of those things that we can modify. Yes, over the past 10, 15 years, there’s been a lot more research on nutrition. Some randomized control trials. A lot more when it comes to dietary patterns of observational studies, looking at groups of people who are either trying to conceive on their own or the assistance of ART, fertility treatments, and how diet can play a role.
[00:10:29] Melissa: Yes, absolutely. I know just in general nutrition research, the bulk of it tends to be epidemiology, observational versus RCTs just by the nature of we’re humans. Then you hear a lot that it’s really hard to do research in pregnant women compared to the general population, so I guess we have a lot to dig into. Should we start by looking at fertility and weight and what the research shows there?
[00:10:56] Rachelle: Sure. Weight is always a very complex topic. I have had the opportunity. I actually just spoke at the American Society for Reproductive Medicine this past October in New Orleans on the topic of weight-inclusive care and supporting fertility patients. I think it’s important to first understand that, the differences between weight-inclusive care and weight-normative care. Weight-inclusive care is not saying that weight won’t change as a result of behaviors, but it’s really focusing on those behaviors.
Weight is not a behavior, but we can try to modify how often we’re eating certain foods, how we’re moving our bodies and focusing more on those actual specific nutrition behaviors rather than intentional weight loss because intentional weight loss comes with some side effects, so we can talk about those.
[00:11:43] Melissa: I’m glad you started there because obviously weight-inclusive care outside of pregnancy, I feel, is getting, no pun intended, but in its infancy.
[00:11:53] Rachelle: Yes.
[00:11:54] Melissa: This is something we’re hearing a lot more about and we’re starting to see more research supporting this approach, but it can be a hot button. One of the reasons we’re even having this conversation is because especially during pregnancy, then there becomes more of a hyper-focus on weight. We’ve all heard the weight gain guidelines and you already mentioned what we eat is one of the few things we can control and so there’s a lot charged with that. A lot for us to talk about for sure.
[00:12:27] Rachelle: Yes. I also want to call out too in the weight-inclusive approach, it’s also considering other factors that affect health and wellbeing. If we consider social determinants of health, modifying nutrition or exercise may not even be accessible to everyone. What we’ll be talking today is more about on the personal level of what people can do individually rather than fixing the social determinants of health because that is a much bigger challenge for sure.
[00:12:53] Melissa: Thank you for mentioning that because it’s definitely worth mentioning and repeating. Thank you. When it comes to some of the research studies that do focus on weight and fertility outcomes, what have you seen?
[00:13:07] Rachelle: I’m going to share some specific studies here and I’ll try to paraphrase them appropriately. In 2021, there was a review study. It showed two randomized control trials showed that intentional weight loss did not improve ART outcomes, those fertility treatment outcomes compared to control groups who were able to start fertility treatments right away. I think something to take away here is instead of gatekeeping people from starting fertility treatments until they lose weight, at least based on these two larger randomized control trials that intentional weight loss isn’t necessarily going to improve their outcomes versus if they’re just able to start fertility treatments right away.
[00:13:46] Melissa: Right, and time is of the essence. There is a window of time here.
[00:13:50] Rachelle: Exactly.
[00:13:51] Melissa: To put that off with the assumption that weight loss will improve outcomes, that’s really important research.
[00:13:58] Rachelle: Right, so yes, you absolutely have to factor in the age of the patient and all of their testing and things. Why are they going through fertility treatments in the first place? That’s definitely something to be mindful of. Then there was another randomized control trial that came out in 2022. That’s known as the “FIT-PLESE”. That’s the acronym F-I-T-P-L-E-S-E. What they found was a preconception intensive lifestyle intervention for weight loss did not improve fertility or birth outcomes compared to an exercise intervention without targeted weight loss.
[00:14:28] Melissa: Interesting.
[00:14:28] Rachelle: For me as a weight-inclusive dietitian, what I take away from some of this research, especially when we look into some more of the dietary patterns research, is that even if we’re not focusing on intentional weight loss, that doesn’t mean just because weight loss doesn’t improve IVF outcomes doesn’t mean don’t refer to a dietitian, but it means that everybody can be referred to a dietitian regardless of their body size, and they can work on using nutrition and some lifestyle modifications to help improve their chances of getting pregnant.
[00:14:55] Melissa: Right, because I can imagine– Well, obviously when I worked in the maternal fetal medicine clinic and worked with endocrinologists, they were coming because they had diabetes or again, the multiples, but outside of that sort of a clinic, people don’t typically get referred to a dietitian. “Oh, you’re pregnant. You should talk to a dietitian about your nutrition lifestyle.”
[00:15:14] Rachelle: Right.
[00:15:15] Melissa: It’s, “Oh, there’s a weight issue here.” That’s why you get referred.
[00:15:18] Rachelle: Yes. As you were talking about that in the beginning of our conversation about working in maternal fetal medicine and a lot of people, when they have issues, we’ll see the dietitian. When they have gestational diabetes, when they have multiples, and they’re higher risk pregnancies, that’s when they might see a dietitian, but why don’t we help people prior to that, or help prevent it, or just give everybody that opportunity, right? Not everybody has to see a dietitian, but give them that option or offer that and let that patient decide if that’s something they want to pursue or not.
[00:15:46] Melissa: Absolutely. Is there anything else in the weight and fertility outcomes? I know you and I talked about, there’s a BMI cutoff. I think this is really interesting and there’s a lot to dig into there.
[00:15:57] Rachelle: For sure. Actually, one thing before we even get into that BMI cutoff that I did want to also call out, when I was at ASRM this past year, that reproductive medicine conference I mentioned in October, there was a paper presented on the impact of increasing body mass index on in vitro fertilization treatment, obstetrical and neonatal outcomes. I thought this was really interesting because there was a pretty large study, included 2,069 fresh IVF ICSI cycles and frozen embryo transfer cycles. What they found was that among patients with a BMI from 30 to 60, and that would be in the “obese category”, correct?
[00:16:37] Melissa: Yes.
[00:16:37] Rachelle: In that group, those who conceived via IVF and received comprehensive prenatal care at a tertiary care hospital, IVF, OB, obstetrical, and neonatal outcomes were largely comparable. A lot of people, even if they’re not prevented on going through with IVF because of their BMI, because the clinic’s cutoff is not so low that they’re still able to proceed with IVF, they’re still typically warned about obstetrical issues of higher rates of– Let me look at specifically what they were including in here.
[00:17:10] Melissa: Like complications during delivery?
[00:17:12] Rachelle: Complications, right, and higher rates of gestational diabetes, higher miscarriage rate, labor induction, cesarean delivery, preterm delivery, neonatal birth weight. What they found was that in this group from 30 to 60, there was really no difference. I think that’s also very interesting information that people are told, “Okay. Well, if you have a BMI of X, then you’re going to have higher chances of having basically pregnancy complications or birth complications.” This found that in that wide range of BMIs, that there really wasn’t any difference.
[00:17:43] Melissa: Okay, and did that look at comparing the 30 to 60 with lower BMIs or-
[00:17:49] Rachelle: No.
[00:17:50] Melissa: -is that a different study?
[00:17:52] Rachelle: Yes. That would be– I’d have to look into. I’m sure there are other studies on that too, but I just thought that this was interesting showing that–
[00:17:58] Melissa: That’s a wide range.
[00:18:00] Rachelle: That’s a big range, right?
[00:18:01] Melissa: Yes.
[00:18:02] Rachelle: Right, because sometimes the cutoff for a fertility clinic might be 40 or 45. That’s a big difference from 30.
[00:18:10] Melissa: Right.
[00:18:12] Rachelle: Just showing that there still can be safe pregnancies and safe deliveries even in increasing BMI.
[00:18:18] Melissa: I was not aware of these BMI cutoffs. Yes. Has this been going on for a long time? Does it vary? Is it just at whim? Tell me more about this.
[00:18:29] Rachelle: Yes, it’s a good question. It does vary by clinic. It’s not a national mandate or anything. In some other countries, there are some cutoffs, like nationally because of more public health systems, but that’s a different topic. We’ll focus on the US for today. There was a committee opinion from the American Society for Reproductive Medicine in 2021 that essentially said there’s not a good reason to have a national cutoff, a standardized cutoff for BMI, because it really has to be taken on an individual basis. The issue with outpatient clinics and more of those private practice, not the hospital-based IVF clinics–
When I worked at Cornell, that’s a hospital-based clinic. Northwestern is a hospital-based clinic here in Chicago. The smaller outpatient places have the cutoffs usually because of their anesthesia. Their anesthesia team has concerns about operating for the egg retrieval. The egg retrieval is done under sedation, so anesthesia is involved. I should have clarified that about IVF. Insemination doesn’t involve any sedation. A frozen embryo transfer doesn’t usually have any sedation, but the egg retrieval process involves a little aspiration needle, a little tiny vacuum going through the vaginal wall to the ovaries to retrieve the eggs.
That’s not a very comfortable procedure to have without some medication, so that is done under anesthesia. Then again, the BMI cutoffs are typically lower at some of the outpatient clinics compared to the hospital ones.
[00:19:57] Melissa: Okay, so the BMI cutoffs are directly related to having this egg retrieval and anesthesia.
[00:20:03] Rachelle: Yes.
[00:20:04] Melissa: Have you seen BMI cutoffs for any other reasons?
[00:20:08] Rachelle: Not that I know of.
[00:20:08] Melissa: Okay.
[00:20:09] Rachelle: Except, I guess I could say that if a doctor, for whatever reason, doesn’t feel comfortable doing that. There are some stories about just even if it’s not anesthesia-related, that a doctor might say certain things to a patient in a larger body about why they shouldn’t be doing IVF.
[00:20:26] Melissa: Okay. A lot of stories, I’m sure.
[00:20:29] Rachelle: Yes. Even if it’s not an anesthesiology concern, some doctors may not want to proceed with a patient’s egg retrieval or fertility treatment until they’ve lost weight. I think that’s where I was going with regards to, there may be some level of gatekeeping there of giving access to fertility treatment based on BMI alone.
[00:20:47] Melissa: Right, yes. That brings us full circle where we started. There are medical professionals who are delaying starting any sort of fertility treatment until the patient loses weight.
[00:20:59] Rachelle: Right.
[00:21:00] Melissa: What does the research show on that?
[00:21:02] Rachelle: I think some doctors too, based on some older research, the correlational research, which is true of nutrition research as well, but this correlational research that says “obesity” or X BMI is associated with some of these worse obstetrical outcomes or lower rates of implantation and such that that’s part of why they recommend weight loss, but what more recent research has shown, including specifically randomized control trials, which is a bit more robust data than observational, has shown that the intentional weight loss hasn’t necessarily improved those IVF outcomes.
To allow people to proceed with their treatments, and again, in my opinion, as a dietitian, offer any patient the opportunity to work with a dietitian to help them be empowered, make informed decisions about one of the few things they may be able to control in their fertility journey.
[00:21:56] Melissa: Okay, yes. That helps a lot. It’s the correlational research, which doesn’t show cause and effect but perhaps showing that higher BMIs may have more complications. Then the logical brain says, “Well, let’s get those BMIs down so that it is more comparable to somebody of a normal–” Do we say normal BMI? If not, sorry. I don’t know what–
[00:22:19] Rachelle: I say quote-unquote normal because that’s the technical category, so I say quote-unquote.
[00:22:23] Melissa: Right. A lower BMI, but then the reality from these randomized control trials are showing it’s not working like that.
[00:22:32] Rachelle: Exactly. One of the issues too, in some of these research studies is that if they’re not looking further below just the numbers, if they’re not looking at just beyond the change in BMI or the change in weight, it’s like, “What’s contributing to that?” Are those people exercising more regularly and are they eating more fruits and veggies and eating more consistently throughout the day of a balanced plate, or are they essentially starving themselves, which unfortunately some previous research studies had people on extremely low-calorie diets?
I’m talking 600 to 800 calories for eight-plus weeks and showing that that didn’t improve IVF outcomes. I just couldn’t imagine ever putting someone on such a restricted diet. That is really restrictive.
[00:23:13] Melissa: Right. Well, we know you’re not getting all your nutrition needs.
[00:23:16] Rachelle: Yes. Even if you’re getting pre-made nutrition shakes or something, it’s just not the same.
[00:23:22] Melissa: Thanks for that clarification. Then let’s look at the fertility and diet quality and what the research shows regarding dietary patterns and outcomes.
[00:23:32] Rachelle: Yes. I’d love to highlight a couple of research studies, one looking at preconception couples. These are not people undergoing IVF or fertility treatments. These are just couples that are planning to conceive. Then I’ll compare it with a couple of IVF-specific dietary patterns and research studies. Again, as we’ve already called out a little bit, observational correlational research is not because an effect. We can’t control for all of this. It’s really hard to do that. Essentially what I’ve seen in the body of research we have so far is that, for lack of a better word, healthy dietary patterns, nutrient-dense dietary patterns have been correlated with improved natural conception and IVF outcomes.
When I talk about IVF outcomes, I mean implantation, pregnancy, and live birth. At the end of the day, live birth is what matters the most, right? Having a better egg quality, better sperm quality is great, but people want to come home with a baby, not just have good eggs, right? I really like to focus on those research studies. With regards to natural conception, this is a 2022 study that looked at two cohorts, so two groups of couples who are planning conception. One group in the U.S., or one cohort in the U.S., and one cohort in Denmark.
They basically found that more anti-inflammatory, which sounds like a double negative in some ways, but the less inflammatory or the more anti-inflammatory “higher-quality diets” were associated with greater fecundability. Fecundability is a really big word, but it just means your chances of getting pregnant in one menstrual cycle. Basically, they showed that the more nutrient-dense, the more anti-inflammatory foods that were in the diet, the better chances they have of getting pregnant in one menstrual cycle. On the flip side, a less anti-inflammatory or potentially a more pro-inflammatory diet or a poor diet quality was associated with decreased fecundability or decreased chances of conceiving in one menstrual cycle.
Interestingly, because there is associations breaking it down a little further, they did find a stronger association among participants with BMIs above 25 and above 35 years old, just to call that out as well. If it’s helpful at all, the specific dietary patterns that were looked at were an alternate Mediterranean diet, the Healthy Eating Index 2010, and then the Danish dietary guidelines. Are you familiar with the alternative Mediterranean diet or the Healthy Eating Index, HEI?
[00:25:57] Melissa: I don’t think so.
[00:25:58] Rachelle: Would it be helpful to talk about what foods are in there?
[00:26:00] Melissa: Yes, that’d be great.
[00:26:01] Rachelle: I actually wrote these down because it’s hard to remember exactly. For what it’s worth, when you break it all down, there’s a lot of overlap between the foods. We can summarize that later. The alternative Mediterranean diet includes more vegetables, legumes, fruit, nuts, fish, whole grains, a higher intake of monounsaturated fatty acids to saturated fatty acids, and moderate alcohol intake. That’s a higher score. That was the more anti-inflammatory, whereas the more red or processed meat and low or high alcohol intake contributed to a lower score. I think that one’s interesting with the Mediterranean diet that actually calls out alcohol where most other dietary patterns don’t.
Then the Healthy Eating Index 2010 included more total fruit, total vegetables, greens and beans. That’s the words they used. Whole grain foods, dairy foods, total protein foods, seafood, and plant proteins, as well as more of the mono and polyunsaturated fatty acids and lower saturated fatty acids contributed to a greater score, whereas the more refined grains, more sodium, more “empty calories” as they put it here, I think that included fast food and soda primarily was what they defined the empty calories as. That contributed to a lower score.
As you can see, there’s a lot of overlap. It’s a lot of plant-based foods and more of those monounsaturated fats and polyunsaturated fats and less of processed red meat and refined grains.
[00:27:26] Melissa: Okay. The Danish diet?
[00:27:28] Rachelle: The Danish diet included more fruit, vegetables, fish, whole grain foods, and less of the red processed meat, saturated fat, or added sugar. They’re not exactly the same, but there’s a lot of overlap.
[00:27:40] Melissa: Definitely.
[00:27:41] Rachelle: There’s other studies too, but I think this is a more recent one and I liked that it included two cohorts from different countries, and it looked at several different dietary patterns and basically summarized that a more anti-inflammatory diet is better for chances of conceiving naturally. That’s a little bit of research on preconception couples, so people that are not undergoing any fertility treatments. I think then it would be helpful to also talk about studies on patients undergoing ART, again, assisted reproductive technology, things like IVF and ICSI.
I think a lot of people have heard of the Mediterranean diet, are familiar with the Mediterranean diet. There’s a lot of research studies looking at a Mediterranean diet. Two different studies looked at those recently. These were both systematic reviews. Sanderman et al in 2022, Alessi et al in 2023 found that a Mediterranean diet was linked with improved fertility, sperm quality and ART success, as they put it, so chances of having success with the IVF treatment. Then the Mediterranean diet also had the strongest, most consistent link with improved pregnancy rates.
There is some variability in definition of what’s included in the Mediterranean diet, but generally it’s favoring more olive oil, fruits, vegetables, legumes, nuts and seeds, whole grains with a moderate amount of seafood and dairy products and occasionally wines included, but not always in that moderate category, and a lower intake of generally red meat and added sugar. What I like about this because sometimes Mediterranean, people think, “Okay, it’s only Italian or Greek food,” but there’s one, a lot of countries that border the Mediterranean beyond those two. Two, in my opinion, you could use those food groups and put them into a lot of different cuisines, right?
It doesn’t have to be eating specific foods just within the categories of what are fruits and vegetables that you enjoy, legumes and whole grains and nuts and seeds. You can really apply it to your personal preferences.
[00:29:32] Melissa: Yes. It applies to a lot of different dietary patterns and as you said, personal preferences. I actually did a recent episode on the Mediterranean diet where we talked about all of those other countries. Actually talked about that a couple of times on the podcast and how, yes, it’s not just Greece and Italy and how you can take your favorite foods and make it Mediterranean. I’ll link to those in the show notes for people.
[00:29:54] Rachelle: Great. I did that podcast. I haven’t had a chance to listen yet, but I love that you have a whole episode on it.
[00:29:59] Melissa: Like you said, most people are familiar with the Mediterranean diet. In fact, it was just ranked number one best diet again this year by U.S. News and World Report. A lot of people are very “familiar” with it,, but there’s still a lot of myths that persist. At first I’m like, “Oh, everybody knows about the Mediterranean diet. I don’t know about doing an episode on that,” but it was fun to dig into some of those myths and really talk about the culinary aspect too, and making your food Mediterranean.
[00:30:29] Rachelle: Yes. Did the person you interview talk about the variability of the definition depending on the study that you’re looking at because it’s not always the same?
[00:30:37] Melissa: Yes. A little bit. One of the myths is that people think, well, I eat salmon and I drink red wine, so I’m good. It’s like, there’s so much more to it, and beyond the diet too, that it’s a lifestyle.
[00:30:47] Rachelle: Yes. Yes, for sure.
[00:30:48] Melissa: One of the things that I particularly liked that we discussed in that episode was the importance of sharing meals with family, friends, community, that that’s such a big part of the lifestyle because I think that gets overlooked sometimes.
[00:31:03] Rachelle: Yes. No, it’s a really important point to call out. I know when I’m working with clients one-on-one or even in my fertility nutrition course, I talk a little bit about it’s not just what we’re eating, but how we’re eating too. Both the social aspect, the emotions or guilt that comes up around food and eating. There’s so much stress in the fertility space, especially, that I don’t want nutrition to become another source of stress like, “I messed this up,” or, “I fell off the wagon,” or something. It’s not that black and white and nutrition can absolutely support people both physically and emotionally along their reproductive journeys.
[00:31:40] Melissa: Yes. That’s another reason that I wanted to have you on the podcast because fertility aside, just the whole relationship with food and behaviors that sort of get amped up during preconception, during pregnancy, even postpartum, there’s just a lot going on in that space. I know we’re going to talk a little bit about disordered eating and fertility and research there, but also just really want to put a finer point on the fact that, like you said, there’s a lot of stress, there’s a lot of guilt. You’re eating for two. It’s not just for you. Before we get into the fertility and eating disorders or disordered eating research, you had mentioned something to me about a pro-fertility diet. I’d love for you to talk about that a little bit.
[00:32:28] Rachelle: Yes. The pro-fertility diet came out of a research study done in 2019 by Gaskins et al. What they were looking at is they basically took previous research studies. I believe this is part of the EARTH study cohort. That’s E-A-R-T-H. It’s like Environmental and Reproductive Health Studies. They took various pieces of certain foods or nutrients that have been correlated with improved ART outcomes and made it a diet. For example, they had done a research study showing whole grains had improved rates of implantation and thicker endometrial lining. They put whole grains in the diet.
They’ve shown previous studies that higher folate intakes from food and supplements can improve ART outcomes. That’s part of it. Essentially the diet, “pro-fertility diet”, as you may also agree with this, the word diet can get thrown around a lot in a more of that restriction weight loss way, but we’re talking about dietary patterns. The pro-fertility diet featured higher intakes of whole grains, dairy, soy foods, seafood rather than other meats, a higher intake of lower pesticide fruits and vegetables, and lower intake of high-pesticide fruits and vegetables, and supplemental folic acid, vitamins B12, and vitamin D.
There’s, again, a lot of overlap with some of the food groups that have been called out in the Mediterranean diet, but there’s a little bit of variability and something that the authors noted on this about the pesticides is that a lot of research studies, say, on the Mediterranean diet have been done in European cohorts, groups of people in Europe versus the US where they have different restrictions on certain pesticides. It’s not to say that eating conventional is bad and eating organic is the only way to avoid pesticides. It’s not that simple. Just because something is organic doesn’t mean it doesn’t have pesticides.
Basically, what they found was that there may be some link because they also have done research studies on environmental toxins and how that can impact fertility. My takeaway here is, again, not to have people stress out about that they should only eat organic or something like that because that’s not what it’s saying, but to really just focus on a variety of fruits and vegetables, and then the other pieces too. Adding whole grains to the diet. If there’s foods that you have allergies to or don’t eat for ethical reasons, of course, I’m not going to say you should eat those.
If you don’t have any dietary restrictions, then including these types of foods, the whole grains, dairy, soy foods, seafood, more fruits and veggies, and then those supplements of folic acid, B12, and vitamin D are things that I think are worth trying, worth adding to the diet.
[00:35:02] Melissa: This pro-fertility diet you said is looking at ART or assisted reproduction technology?
[00:35:07] Rachelle: Yes. It was a group of people undergoing IVF, US couples, and I believe this was done in Boston. What they found was that the higher the adherence, the more similar people’s diets were to this pro-fertility diet, the higher chances they had of implantation, clinical pregnancy, and live birth. It increased. The closer the diet got to this standard diet that they created, the higher the chances were. Does that make sense?
[00:35:34] Melissa: Yes.
[00:35:34] Rachelle: Increased rates of implantation, pregnancy, live birth, and lower rates of clinical pregnancy loss.
[00:35:41] Melissa: Again, we see some overlapping, seafood, whole grains, produce, things like that. You mentioned supplements. I don’t want to get off track, but even if we have the “perfect diet”, I hesitate to say that, I’m saying it in quotation marks, there are some nutrients that is hard to get through food alone. Can you just comment briefly on supplementation for preconception, perinatal, postnatal? I know that’s a big question, but I don’t know if there’s anything you wanted to call out.
[00:36:16] Rachelle: Sure. Yes, no, it’s a good question. Yes, as you mentioned, we could go off on a whole hour-long episode just about that. [chuckles] We know that the supplement industry is a very– What? A multi billion dollar industry probably? There’s a lot of marketing towards people who are trying to conceive that they have to be taking this and all of these other things.
I try to pare it down as much as possible and to your point, focus on the things that are harder to get from diet alone, as well as nutrients where Americans in general tend to fall short. Then the ones that have been linked to improving the ART outcomes. Basically in this pro-fertility diet, I think the recommendation for a preconception, anyone who could try to conceive is recommended to take 400 micrograms of folic acid daily in addition to folate-rich foods in their diet. What they found was that higher rates of folic acid, and I believe it was above 800 micrograms, had more benefit to people undergoing IVF.
We know that folate or folic acid is involved in methylation and DNA synthesis, which is really important when we’re talking about making eggs and conceiving in the early stages of embryonic development. That one, I think, is really important to focus on from food and supplements. Vitamin B12 is also involved in the methylation process and DNA synthesis, so that’s another one that they found that higher amounts than what’s the RDA for B12 may have some additional benefit from food and supplements.
If people are vegan, they’re not really getting any B12 from food alone. They have to get it from supplements. If people are omnivores and consume meat or animal products, they’ll get B12 from food as well as getting it from a supplement.
[00:37:53] Melissa: Dairy, eggs, milk, yes.
[00:37:56] Rachelle: Then vitamin D. We were talking earlier, we’re here in the Chicago area. It’s gray and cold and I’m basically covered from head to toe with clothing, so I am not converting vitamin D from sunlight into active vitamin D in my body. Most people need to take supplemental vitamin D. Then again, in this dietary pattern, the pro-fertility diet, they found that a higher amount than the RDA, I think it was 843, something like that was above 800 IUs, seemed to have additional benefit. I think focusing on those nutrients would be important.
Then, I usually will recommend a multivitamin that has a combination of these things and also has iodine because that’s really important for thyroid hormones. It’s required for thyroid hormone development and it’s really important in pregnancy. The American Thyroid Association recommends 150 micrograms for people who could become pregnant or are pregnant or breastfeeding. That’s another one I’m typically looking for.
[00:38:50] Melissa: Interesting.
[00:38:51] Rachelle: Iron is not as– Well, if you have iron deficiency or anemia, then you may need supplemental iron prior to pregnancy, but it’s really important once you get to the second and third trimester that iron needs increased significantly. Usually, a multivitamin that has iron in it can be helpful, but some people don’t tolerate it. It makes them constipated. If they are actually pregnant, it might make them nauseous. You may be able to hold off on that until you’re into the second trimester if needed. All of this should be discussed with your healthcare provider, dietitian, or a doctor, of course.
I wanted to add one more, the omega-3s. Omega-3s or fish and seafood are called out in a lot of these dietary patterns that have been linked with improved fertility and natural conception. Seafood and fish are very good sources of DHA. If you don’t include those in the diet, I would recommend supplementing that as well.
[00:39:41] Melissa: Right. Yes. I remember when I was pregnant, that was the new thing is getting your DHA, EPA supplement. I did do that and my son is really smart.
[00:39:51] Rachelle: Yes. That must be it.
[00:39:54] Melissa: Thank you for that little side tangent on supplements. I appreciate that and I agree. It could be an entire segment. Let’s go back to our thoughts on disordered eating or eating disorder sort of research regarding fertility. What are you seeing there? Obviously, like we already mentioned, eating pre, during, postnatal, there’s a lot that can be stressful about that.
[00:40:23] Rachelle: Yes, it’s very stressful, right? It’s really easy to blame your body and want to control what you can control. That’s where diet can come in. I’m always struggle with the word to use when I talk about nutrition being one of the few things we can control because control can be a slippery slope. We don’t want to be like micromanaging the diet, but we want to use nutrition to help improve our chances and feel good along the way, right? You have to eat, so let’s use nutrition to support your energy levels and feel nourished and feel like you have energy for physical activity and your bowel movements are good, et cetera.
[00:40:57] Melissa: Yes. Even the word control, we do not use that in the diabetes world anymore because of that negative connotation.
[00:41:04] Rachelle: Like glucose control?
[00:41:05] Melissa: Yes. We talk about managing blood glucose, not controlling blood glucose. That’s a loaded word in and of itself.
[00:41:14] Rachelle: Yes. Going back to what we were talking about earlier about some of the benefits of weight-inclusive care, research has shown that one, it may be as effective for improving physical, psychological, and behavioral outcomes. That was a 2020 review study. A 2022 study found that weight-inclusive approach had a positive or neutral effect on diet quality and a favorable effect on eating behaviors and that it’s less stigmatizing.
We know that weight stigma can increase body dissatisfaction, which is a significant risk factor in the development of eating disorders. Typically people that are in larger bodies have been told that’s a problem their whole life, right? That’s not news to them. When they’re now confronting fertility challenges and the thing that the doctors focused on is like, “You need to lose weight,” I just can’t imagine the emotional burden of that statement.
We have research, too, that the rates of current and past eating disorders are higher among women seeking fertility treatment than it is in the general population. Again, this is correlational. We don’t know exactly why that is. I think that was the 2021 or 2022 study. I don’t have it written down, but we can link it in the show notes. It’s something I want to be really mindful of is how do we use nutrition to support folks who are trying to conceive without it becoming a slippery slope of another diet or another way of some controlled eating or disordered eating behaviors because it’s not just eating disorders that are a problem?
There’s a continuum of disordered eating. You had a podcast on, was it Jessica Setnick?
[00:42:46] Melissa: Yes.
[00:42:46] Rachelle: It might’ve been a while ago now, but I was listening to it and she talked about that.
[00:42:49] Melissa: Yes. She talked about dysfunctional eating behaviors, I think is what she calls it, yes.
[00:42:54] Rachelle: That’s right. Even if someone doesn’t have an acute eating disorder, lots of people struggle with disordered eating, so we want to be really mindful of that when any dietitian working with anybody, but especially patients who are undergoing fertility treatments that are already at higher risk. A lot of people who are dealing with fertility challenges, PCOS is a common disorder among people with fertility challenges. They’re also at higher rates for eating disorders and disordered eating. If I could add one more thing, eating disorders are implicated in the HPG axis.
That’s the hypothalamic pituitary gonad axis, and their dysfunction, which we know that can result in missed periods, ligamentaria, amenorrhea, and ovulatory dysfunction. Ovulatory dysfunction is the most common cause of female infertility. There’s a lot there, and there’s a lot of context and nuance to be considering when we’re talking about nutrition and fertility. That’s why I focus on the nutrition more than the weight loss piece, focusing on the modifiable behaviors.
[00:43:54] Melissa: Right. I think anytime you’re in a situation that dietary changes are recommended or may be beneficial, that can in and of itself be a trigger, whether you’ve had previous disordered eating or not. I know we see this a lot with diabetes. “Okay, we’ve got to look at our carbs. We have to look at what time we’re eating,” and all of these things, and that in and of itself can trigger people to these harmful behaviors. Again, another plug for weight-inclusive counseling, right?
[00:44:29] Rachelle: Another plug for weight-inclusive care and also a plug for just dietitians, who even if you’re not specializing in eating disorders, we have skills to be able to know when to refer people on too, and to ask those questions that doctors may or may not, because if it’s not overtly in their medical history, if you’re not asking, how do you know?
[00:44:45] Melissa: Yes. I guess that’s a good segue into just nutrition counseling in general for preconception, prenatal. I know this is the work that you do. Our listeners are a mix of dietitians and other healthcare professionals, but also just the general public. What do we need to know about nutrition counseling around conception?
[00:45:04] Rachelle: Oh, that’s a big question. I would say keeping in the back of our mind, the dietary patterns, the research on what foods and overall dietary patterns can help people with their chances of conceiving and having a healthy pregnancy, keeping that in the back of our mind. Then we’re breaking it down into actionable goals and behaviors and things that we can modify. Talking to them about what is their diet currently like and where’s there some area maybe for improvement that again, is accessible to them.
We want it to be realistic and accessible. We don’t want to have people do changes. In my experience, when people are very motivated to change, they are willing to do some pretty significant things, some pretty significant overhauls. I always try to pull people back a little bit because I’m like, “We need this to be sustainable.” Most people can do things for a really short period of time, but how do we make it sustainable? I don’t want them to– I think about exercise as one that comes up a lot. It’s like, “Okay, I’m going to work out five days a week,” and they’re doing nothing right now.
I’m like, “Well, maybe let’s start at one or two days a week and build from there,” because it’s– or they’re not eating any fruits or vegetables, or maybe they’re having one a day and they’re trying to have like one at every meal. It’s like, “Let’s start with two if you’re at one,” just making them more gradual and realistic changes.
[00:46:23] Melissa: I will say pregnant women are the most motivated patients on the planet. I’ve seen it firsthand.
[00:46:30] Rachelle: Yes.
[00:46:31] Melissa: To your point, just maybe reeling it in a little bit and saying, “Okay, these are great goals, but how do we really break this down and make it sustainable?”
[00:46:40] Rachelle: Right. Bringing it back to the weight loss piece, when people are told, “Okay, you need to lose weight before you can do an egg retrieval,” they come to me and they’re like, “Well, I’ve already been intermittent fasting and I’ve cut back on my carbs and fat and calories.” I’m like, “Whoa,” that’s just like you’re restricting nutrients that your body needs to function optimally and to support your reproductive system because that’s not necessary compared to your lungs and your brain and your heart function, We don’t want to be cutting back so much because yes, that might result in weight loss, but is that improving their health?
[00:47:16] Melissa: Right.
[00:47:17] Rachelle: No.
[00:47:18] Melissa: Exactly.
[00:47:18] Rachelle: Focusing on consistent meals throughout the day. I like to talk about the plate method, of some fruits or vegetables and usually favoring more of the whole grains or the starchy veggies for carbs, and the protein rich foods and using that as a meal planning tool, honoring hunger and fullness, being able to tune into your body. In my private practice, as well as in my nutrition course, I talk about tenets of intuitive eating and emotional eating and how that comes up, and your relationship with food when it comes to making dietary changes.
This isn’t just to help you get pregnant but to also have a healthy relationship with food and a healthy pregnancy and to continue that hopefully more lifelong and not just for this acute period of your life.
[00:48:01] Melissa: Yes. Tell us about your fertility nutrition course.
[00:48:04] Rachelle: Yes, thanks. It’s a newer course. I launched it in March of last year and it is a self-paced online course that is meant to be a standalone resource that people can do on their own time. I can’t work with everybody and not everyone can work with me for various reasons, whether it’s time or money or state licensure restrictions. I do telehealth so I can work with people in a variety of states, but I can’t work with everyone in every state. I wanted to create a resource that is evidence-based, weight-inclusive.
I call it Fertility Foundations because it is meant to cover the most foundational aspects of nutrition as it relates to fertility. I talk about some of the weight and weight bias and weight loss research, why I practice from a weight-inclusive approach. I talk about some intuitive eating and non-diet principles. I talk about macronutrients and micronutrients, some nutrition 101 stuff so that people– because we can’t talk about adding these “fertility foods” to your plate if you’re not eating enough, or not eating a variety of nutrients.
I provide a foundation of that. Then I talk about dietary patterns research and what are the key foods from all of these studies and how you can start to put it into practice. Then I also have an overview of caffeine, alcohol, and sweeteners because there’s also some research on– People always want to know about sugar and sugar substitutes. Then I also have a lesson on supplements, talking about what we were talking about a little bit with the multivitamin as well as some other supplements that have specifically been shown to have some positive effect on fertility.
Really paring it down as much as possible so people aren’t wasting their money on tons of supplements that may have no effect at all.
[00:49:42] Melissa: Great point. Right. It sounds like this course would be great for any healthcare providers, dietitians in particular, who want to learn more about fertility, nutrition, and/or to let their patients know about it.
[00:49:55] Rachelle: For sure. I don’t know if it’s my personality or if other people are like this too, but for me to make behavior change or to actually want to do something, I want to understand the why. Why am I doing this? What I do is I lay out– I don’t want it to be too scientific, too research-heavy in the sense of somebody can’t understand it, but it is very evidence-backed and lots of research to show like, “Okay, this study showed X. This study showed X,” and then what does that mean for you? How do you put this into practice? I’ve been working with fertility patients since 2006.
I’ve been doing this in some capacity for 17-plus years, so I have a lot of the evidence from the research as well as my experience as a clinician. It’s all informed with my approach to things.
[00:50:39] Melissa: Wonderful.
[00:50:40] Rachelle: It’s not for somebody with an eating disorder. I do call that out on my sales page, the description of the course, as well as in the first lesson, which is actually available through my website. You can get the first lesson for free. It’s basically just why nutrition matters for IVF. I go into some overarching research and then who this course would be good for and preparing to get started in it. That’s something that’s available for folks and they can see if this course would be a good fit for them.
[00:51:05] Melissa: Okay, great. You also do some one-on-one counseling, so do you like to address who should work with you in that capacity versus the course?
[00:51:14] Rachelle: Yes, and I do have some folks now that do a combination. They have the course to do some educational modules on their own time so we’re not spending so much time on the–
[00:51:24] Melissa: Foundation stuff.
[00:51:25] Rachelle: Yes, the stuff that they can learn in a more educational way and consume versus the counseling piece in session like, “Okay, what are the barriers for you? What is coming up from your relationship with food that we need to address to help nutrition really work for you?” Also, for people with multiple medical conditions, someone who’s dealing with IBS and PCOS, or endometriosis and IBS. I also have some extra training on irritable bowel syndrome, IBS. I have some specialty area there, but those are just some examples. People have a lot going on.
Then again, somebody with eating disorder history or some really disordered eating I think would benefit from either just one-on-one counseling or a combination of the course and the counseling piece.
[00:52:08] Melissa: Great, and please share your website and any social media links where people can connect with you and find out more about this course.
[00:52:14] Rachelle: Thanks, yes. It’s pretty easy. Everything’s my first and last name. That’s Rachelle Mallik. The tricky part is the spelling. It’s R-A-C-H-E-L-L-E M-A-L-L-I-K.com. RachelleMallik.com. Then my handle on Instagram is @RachelleMallik. My email is just hello@RachelleMallik. Feel free to send me a message or follow me on Instagram.
[00:52:34] Melissa: Okay, great. Yes, any of the studies that we talked about that you do have links to or PDFs, I can put those in the show notes if people want to check those out.
[00:52:42] Rachelle: Great.
[00:52:43] Melissa: Thank you for coming on the show. I want to recap the top three takeaways that I’ve garnered is, why nutrition for fertility matters, why working with a dietitian with experience in fertility is important, and just the benefits of focusing on these health-promoting behaviors for fertility rather than just focusing on weight.
[00:53:04] Rachelle: Could I add to that, actually?
[00:53:04] Melissa: Absolutely. I was going to say, is there anything else that you wanted to share?
[00:53:07] Rachelle: Yes, because I don’t think we talk too much about why working with a dietitian with experience in fertility is important. I just wanted to add in, there’s no formal training at this time for calling yourself a fertility dietitian. Then there’s a lot of people online that they’re not even dietitians who focus on fertility. It’s not to say that they’re not giving good advice. I want to be clear about that, but I’d be careful about what advice is being given because where are they getting their training? Do they attend reproductive medicine conferences? Where do they seek out additional information? Are they staying up to date on the literature?
I’ve worked in an IVF center for five years, and again, have many years of practice as a clinician working with patients, which is very different than just putting content out there. I’m working with people in creating behavior change and I have a strong background in working in a fertility clinic, working with fertility doctors and nurses and genetics counselors and psychologists.
[00:54:07] Melissa: Definitely beyond the basics, for sure.
[00:54:08] Rachelle: Beyond the basics, right? Especially for people who are dealing with IVF, that they want to work with somebody who understands what they’re going through because it’s a lot.
[00:54:16] Melissa: Yes. Well, thank you for clarifying that. I appreciate that. For everybody listening, if you liked this episode, please share it with a friend or tell a friend about the podcast and also check out some of the episodes that we referred to in this conversation. I’ll link to those in the show notes again. I do an annual survey and people are like, “Well, where are these show notes?” They are at soundbitesrd.com. www.soundbitesrd.com. You can find everything there. Thank you again, Rachelle. I have learned a lot from you and I just think the work that you’re doing is so important and you’re helping so many people and just can’t say enough. Thank you.
[00:54:56] Rachelle: Thank you. I really appreciate having me on and being open to such a robust conversation about all these different aspects related to fertility and nutrition.
[00:55:03] Melissa: Absolutely. For everybody listening, as always, enjoy your food with health in mind. Until next time.
[music]
[00:55:12] Announcer: For more information, visit soundbitesrd.com. This podcast does not provide medical advice. It is for informational purposes only. Please see a registered dietitian for individualized advice. Music by Dave Burke, produced by JAG in Detroit Podcasts, copyright Sound Bites, Inc. All rights reserved.
[00:55:39] [END OF AUDIO]
LISTEN, LEARN AND EARN
Listen to select Sound Bites Podcasts and earn free CEU credits approved by the Commission on Dietetic Registration (CDR) for registered dietitian nutritionists and dietetic technicians, registered. Get started!
Get Melissa’s Sound Science Toolkit here!
Partnerships:
Sound Bites is partnering with the Association of Diabetes Care and Education Specialists (formerly the American Association of Diabetes Educators)! Stay tuned for updates on the podcast, blog and newsletter!
Sound Bites is partnering with the International Food Information Council! Stay tuned for updates on the podcast, blog and newsletter!
Sign up for my monthly newsletter and episode eblasts so you never miss an update!
Listen on Stitcher (Android)
Install the Stitcher App
1. Search for “sound bites with melissa joy dobbins” 2. Choose Play Current Episode or Add to Playlist
Choose “Play Episode”
Subscribe & Review on iPhone
Open the “Podcast” app on your iPhone
Search for “Sound bites with melissa joy dobbins”
Open the podcast and click “Subscribe” and your done!
Write a Review
Click “Reviews”, then “Write a Review”.
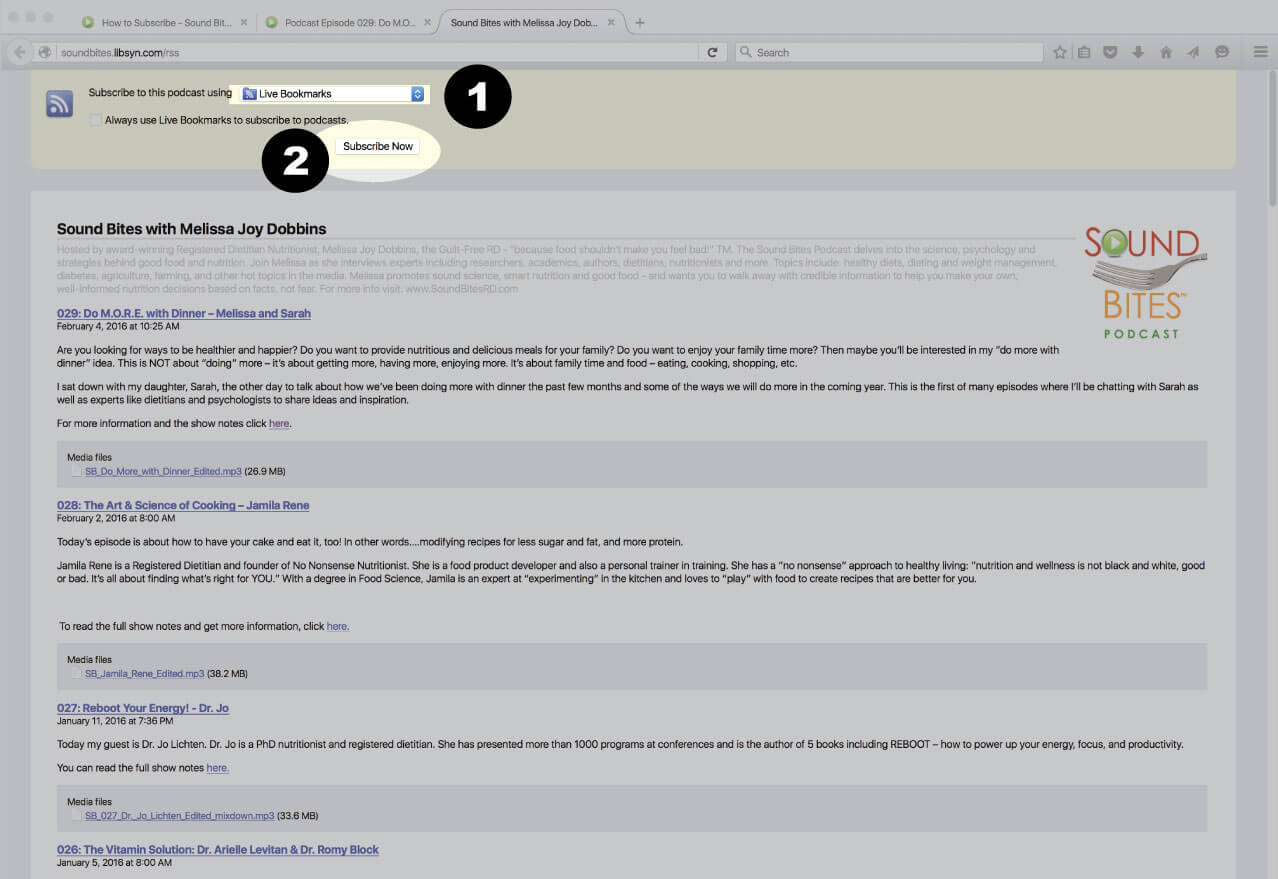
Subscribe via RSS Feed
Navigate to any podcast player . Click on the RSS feed icon.
Click on the RSS feed icon.
Click on RSS Feed
Choose which application you would like to use to receive the RSS feed
Click “Subscribe Now”
Confirm settings and subscribe.
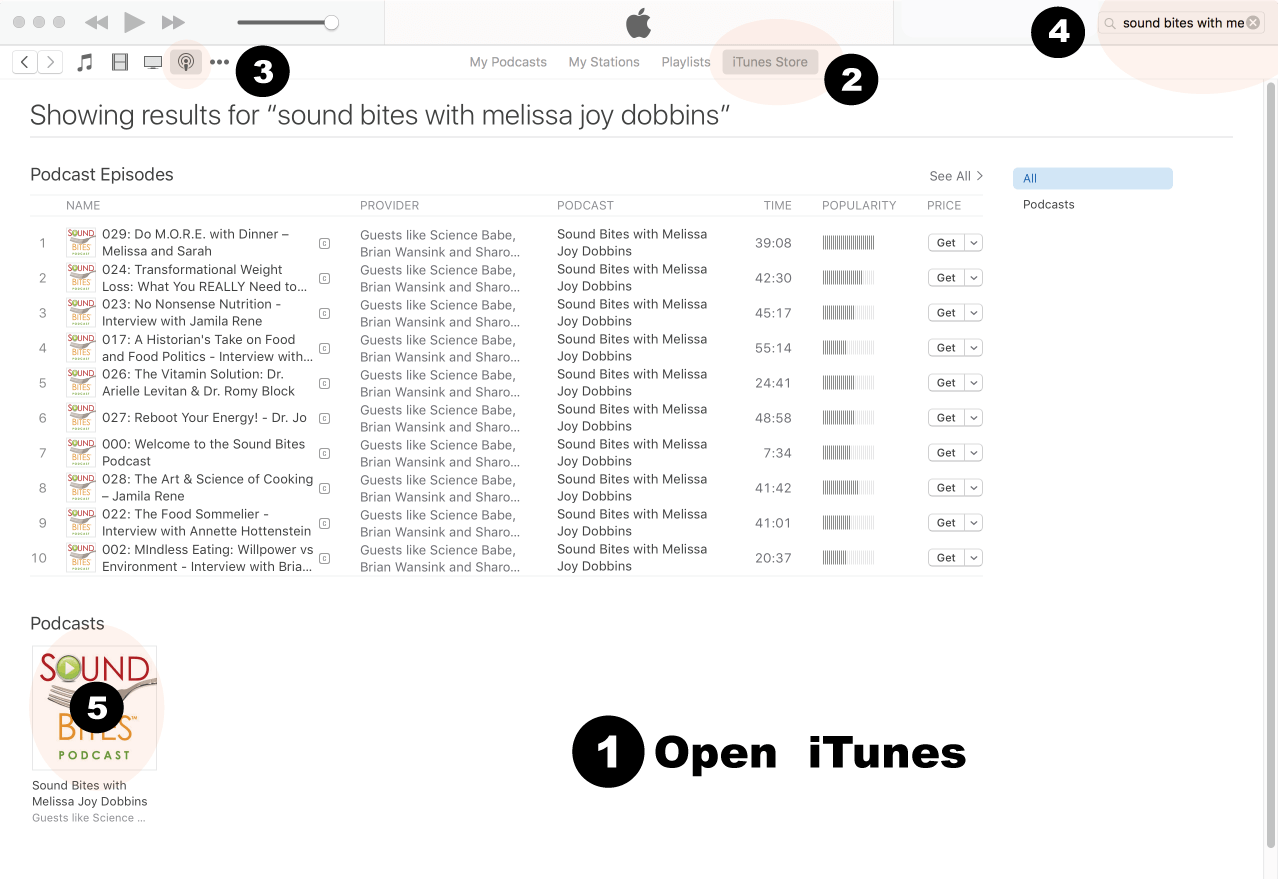
How to Review in iTunes
Open iTunes desktop application
Click iTunes Store
Click on Podcasts
Search for “Sound bites with Melissa Joy Dobbins”
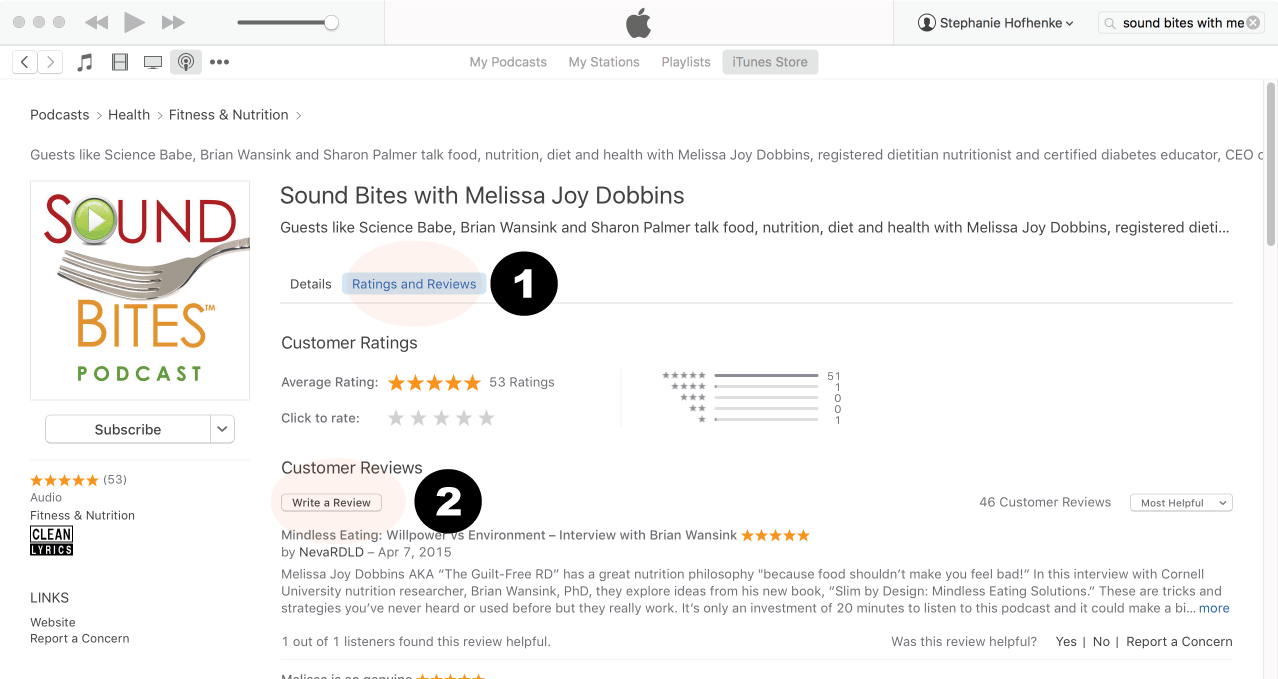
Click on podcast image
Search for Sound Bites podcast in iTunes
Click Ratings & Reivews
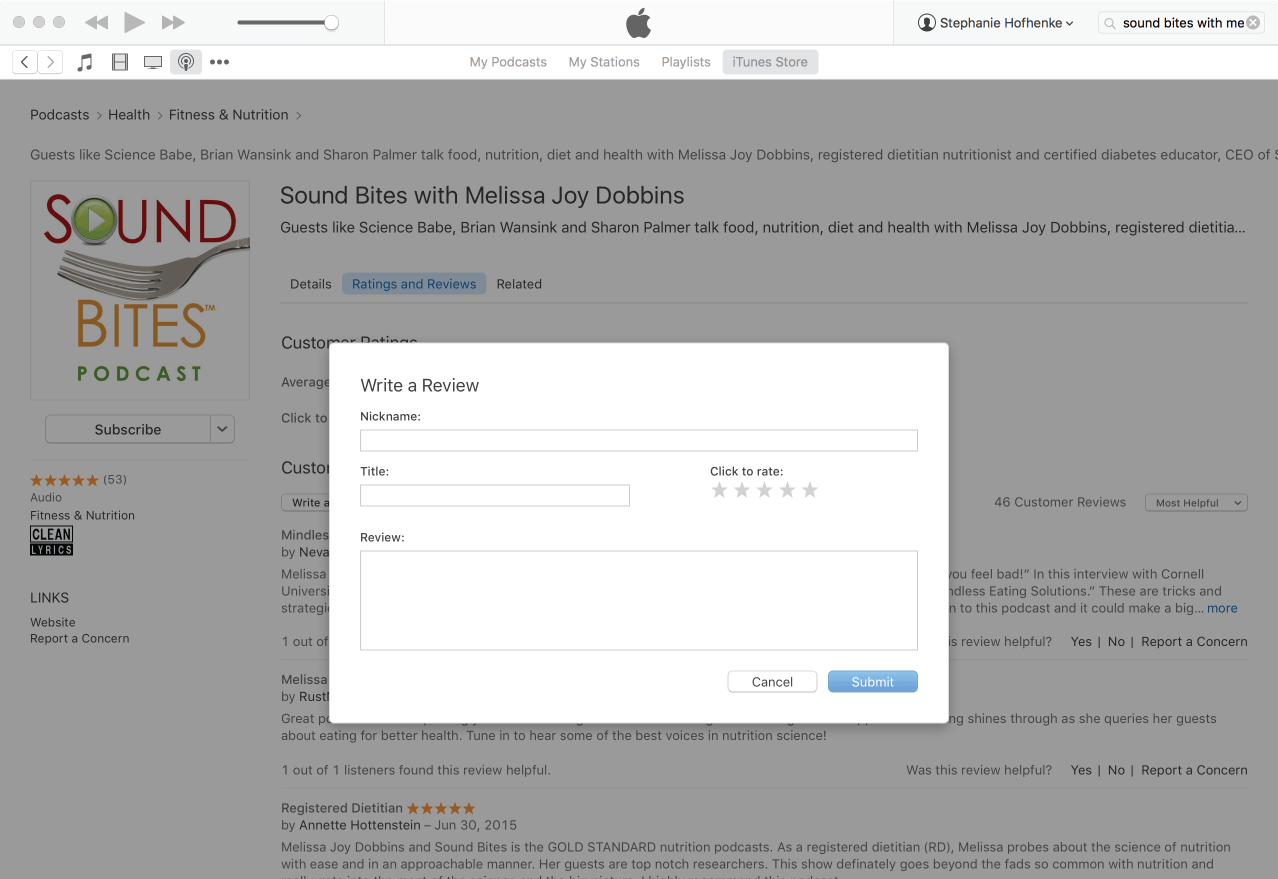
Click Write a Review
View reviews and write your own review.
Write your review…. Thank you!
Write your review!
How to subscribe via iTunes
Click here to view the Sound Bites Podcastin iTunes, then click the blue “View in iTunes” button. This will open your iTunes application directly to Sound Bites Podcast. Click the “Subscribe” button, and your done!